C - Cleaning the least-soiled areas prior to cleaning the most-soiled areas
The least-soiled areas should be cleaned first to prevent moving more contaminants into the cleaner areas.
A nurse is assisting a patient with personal hygiene care. Which of the following actions be the nurse will reduce the risk of infection?
- Washing the patient from the shoulder down to the fingertips with smooth, short strokes
- Washing eyes from the outer canthus to the inner canthus
- Cleaning the least-soiled areas prior to cleaning the most-soiled areas
- Massaging reddened areas of the patient's skin
B - Moisture from excessive diaphoresis can cause skin breakdown.
The greatest risk to the patient is skin breakdown, which can result from increased contact with the moist sheets causing skin irritation and promoting bacteria growth. Therefore, the linens should be changed frequently.
A nurse is caring for a patient who is on long-term bedrest and requires frequent linen changes due to excessive diaphoresis. Which of the following is the priority rationale for frequent linen change?
- It provides an opportunity to turn the patient from side to side to facilitate clearing potential fluid from the lungs.
- Moisture from excessive diaphoresis can cause skin breakdown.
- It provides an opportunity to frequently evaluate the patient's skin on his back side.
- Moisture on the sheets can cause discomfort to the patient.
C - Ask the patient in what order she typically performs her morning routine.
The patient’s plan for routine morning care should be tailored to the uniqueness of the patient’s typical routine.
When planning morning hygiene care for a postoperative patient, which of the following actions should the nurse include?
- Inform the patient when morning hygiene care is provided at the hospital.
- Schedule to provide care to the patient and her roommate at the same time.
- Ask the patient in what order she typically performs her morning routine.
- Plan to provide care before the next scheduled dose of pain medication.
- Gather all necessary supplies
- Place a rubber mat on the tub floor
- Assist the patient into the bathroom
- Instruct the patient on using safety bars when getting in and out of the tub
- Instruct the patient to remain in the tub for no longer than 20 min.
When assisting the patient with a tub bath, the nurse should first gather all necessary supplies and then prepare the room by placing a rubber mat on the tub floor to prevent the patient from slipping and falling. The nurse should assist the patient into the bathroom and then give instructions regarding the use of bars to prevent slipping and falling when entering or exiting the bathtub. Finally, the patient should be instructed to remain in the tub for no longer than 20 min due to the possibility of vasodilation from the warm water, which can in turn cause light-headedness or dizziness.
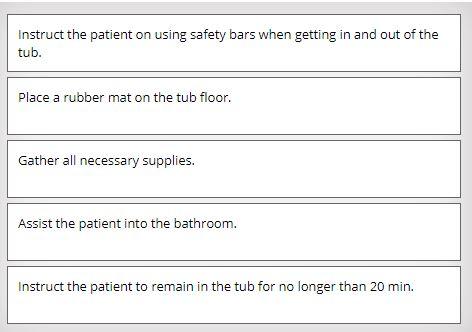
A nurse is preparing to assist a patient with a tub bath. Identify the sequence of steps the nurse should take?
(Move the steps into the box on the right, placing them in the selected order of performance. All steps must be used.)
D - The AP reuses the patient's blanket and spread.
The mattress pad, sheet, blanket, and spread may be reused for the same patient if they are not wet or soiled.
A nurse observes an assistive personnel (AP) make a client's bed while the client is out of the room. Which of the following actions by the AP is appropriate for this task?
- The AP records the task when it is completed.
- The AP makes a mitered corner with the blanket and spread.
- The AP wears sterile gloves while making the bed.
- The AP reuses the patient's blanket and spread.
B - I'll swab the patient's mouth with chlorhexidine (Diluted Hydrogen Peroxide)
Chlorhexidine is the correct solution to use for daily oral care for the unconscious patient because evidence-based practice indicates it improves patient outcomes by preventing microbial build-up.
A nurse is caring for an unconscious patient. Which of the following statements by the nurse indicates an understanding of providing good oral hygiene for the patient?
- I'll swab the patient's lips with a very small amount of mineral oil.
- I'll swab the patient's mouth with chlorhexidine.
- I'll swab the patient's mouth with mouthwash.
- I'll swab the patient's mouth with lemon-glycerin swabs.
C - raise the room temperature.
Raising the temperature of the room will help keep the patient warm while various parts of the body are exposed and washed.
While performing a complete bed bath for a patient, the nurse should
- add soap to the water in the basin before beginning the bath.
- completely remove the linens.
- raise the room temperature.
- complete the bathing for one side of the body at a time.
C - Oral care is still important even though you are not eating.
Bacteria are still present in the oral cavity regardless of NPO status. It is important to perform oral care to help reduce oral bacteria and keep the oral cavity moist.
A nurse is caring for an adult patient who is NPO. The patient is refusing oral care. Which of the following is an appropriate response by the nurse?
- Since you are not eating, we can wait and do it before bedtime.
- We will wait until your family gets here to help.
- Oral care is still important even though you are not eating.
- I'll give you a sip of water to swish around in your mouth, and then you can spit it out.
activities of daily living (ADLs)
tasks performed routinely during the course of a typical day, such as walking, eating, bathing, brushing the teeth, and grooming
adaptation
adjustment to changes in circumstances such as those resulting from illness or disability
alopecia
hair loss
athlete's foot
a chronic superficial fungal infection of the skin of the feet, typically between the toes
buccal
pertaining to or directed toward the bucca (cheek), the fleshy portion of the side of the face that makes up the lateral wall of the oral cavity
callus
a thickening of or a hard thickened area on skin
canthus
the angular junction of the eyelids at either corner of the eye
cheilosis
manifestation of vitamin B complex deficiency characterized by reddened lips with fissures at the angles of the mouth
closed bed
a bed prepared in a hospital room with the top sheet, blanket, and bedspread drawn up to the head of the mattress under the pillows
corn
often painful and inflamed circumscribed lesion of thickened skin, usually on the toes and caused by pressure or friction from ill-fitting shoes
cuticle
the narrow band of epidermis extending from the nail wall onto the nail surface
dentail carie
tooth decay
dental plaque
a sticky film accumulating on the teeth that is formed by and harbors bacteria; also called tartar
drawsheet
linen item placed under the patient's torso and used to lift and reposition the patient
excoriation
skin abrasion typically resulting from scratching
expectorate
to expel fluid or secretions from the mouth, throat, or lungs by coughing and/or spitting
fanfolding
applying the proximal half of a piece of linen in successive layers lengthwise for the purpose of tucking it under the patient and rolling the patient over it while stripping or making an occupied bed
fissure
a break, slit, or tear in soft tissue, often at the junction of skin and mucous membrane
foreskin
fold of skin covering the glans penis (head) of an uncircumcised penis; also called prepuce
gingiva
the part of the oral mucosa covering the tooth-bearing border of the jaw; also called gums (plural: gingivae)
ginggivitis
inflammation of the gums characterized by redness, swelling, and intermittent bleeding
halitosis
bad breath
hygiene
personal maintenance of cleanliness
hypoallergenic
unlikely to cause an allergic (hypersensitivity) response
incontinent pad
involuntary release of urine from the bladder or feces via the anus
ingrown toenail
painful condition in which the corner or side of a toenail grows into the soft flesh of that toe
labia
folds of skin on either side of the vaginal orifice
lanula
active area of nailbed growth at the base of the fingernails and toenails
maceration
softening or dissolution of tissue after lengthy exposure to fluid
mucosa
the moist inner lining of various tubular structures, including the mouth, esophagus, stomach, and intestines
neuropathy
any of numerous disturbances or pathologic changes in the peripheral nervous system, most often affecting sensation
NPO
nothing by mouth, derived from the Latin words nil per os
open bed
a bed prepared in a hospital room with the top covers folded back to make it easy for the patient to get into the bed
palate
the roof of the mouth separating the mouth from the nasal cavity, comprised of the hard palate (in the front of the mouth, separating cavities of the mouth and the nose) and the soft palate (the fleshy portion that separates the mouth from the pharynx)
pediculosis
lice infestation
perineum
area between the anus and the posterior portion of the external genitalia
periodontal
surrounding or near a tooth
periodontitis
inflammation or degeneration of the tissues surrounding the teeth
plantar wart
a skin lesion on the sole of the foot typically caused by any of the human papillomaviruses
sebaceous gland
oil-secreting organ of the skin
sebum
fatty lubricant secreted by the skin's sebaceous glands
semi-Fowler's position
position with the head of the bed raised approximately 30 degrees
smegma
thick, cheesy secretion that accumulates under the labia minora or the male foreskin
stomatitis
any inflammatory disorder of the mouth
tartar
a sticky film accumulating on the teeth that is formed by and harbors bacteria; also called dental plaque
thrush
a fungal infection in the mouth and/or throat caused by Candida albicans and manifesting as white patches and ulcers
urethra
a narrow tube through which urine passes from the bladder to the outside of the body
- remove sweat, oil, and micro-organism
- stimulates circulation
- promotes a feeling of self-worth by improving the patient's appearance
- time for socialization for patient who are on bedrest
- opportune time for the nurse and patient
- be able to perform a head-to-toe skin assessment:
palpation
skin's color
trexture
temperature
Bathing
- bed bath
- partial bed bath
- therapeutic bath
- shower
- tub bath.
For patients in critical and long-term care settings who are unable to bathe themselves, you’ll provide a complete bed bath using either a commercial bag bath or cleansing pack.
Types of baths (bathing) techniques
- bathing only those parts of the body that cause discomfort if not bathed. These include the hands, face, axillae, back, and perineal area. Patients who are dependent and require only a partial bed bath or self-sufficient patients who must remain in bed but cannot reach all body parts often receive a partial bed bath.
partial bath
- part of the treatment plan for such conditions as skin disorders, burns, elevated body temperature, and muscular injuries. Oatmeal, cornstarch, and commercial bath products are sometimes added to the bath water to relieve skin irritation. For patients who have had rectal or perineal surgery, a sitz bath is often prescribed to reduce pain and inflammation. To add this type of bath to a patient’s plan of care, you must obtain an order from the patient’s provider.
therapeutic bath

- When performing a bed bath with soap, water, and a washcloth, fold the washcloth into a mitt over your hand to keep water from splashing or dripping onto the bed or the patient. It also helps keep the edges of the washcloth from brushing against the patient.
- To fold the washcloth into a mitt, wrap one edge of the cloth around your palm and fingers. Wrap the other edge of the washcloth around your hand and hold it in place with your thumb. Finally, tuck the top edge of the washcloth under the edge that is in the palm of your hand.
Folding a washcloth mitt
- You’ll change bed linens after the patient’s bath or while the patient is in the shower, sitting in a chair, or out of the room for a test or a procedure. You’ll also straighten the bed linens throughout the day to remove any wrinkles and, of course, you’ll change them if you find them wet or soiled. Encourage patients on bed rest to participate as much as possible, as this can help maintain their strength, mobility, and a certain amount of independence with activities of daily living.
- It is ideal to change the bed linens when the patient is out of the bed. However, if the patient is too weak to get out of bed or restricted to bed rest, you’ll have to change the linens while the patient is in bed. Because this can be tiring for the patient, be sure you are organized before beginning the process. If the patient is experiencing any pain, administer a prescribed PRN analgesic about 30 to 60 minutes beforehand to help control the pain and make the patient as comfortable as possible while you change the linens.
- When changing the linens on the patient’s bed, you might not have to change all the linens each day. Typically, you’ll change the bottom sheet, top sheet, and the pillowcase. However, you can leave the same mattress pad, blanket, and bedspread in place if they are not wet or soiled.
- Follow standard precautions by wearing gloves if the linens are soiled and by keeping the linens away from your scrubs when throwing them in the linen hamper. Also, avoid shaking the linens since this can spread micro-organisms in the air. If at anytime during the linen change the clean linens touch the floor, place them in the linen hamper and use clean ones instead.
- Observing good body mechanics and patient safety is also important when changing the linens on the patient’s bed. Be sure the bed is at a comfortable working height so that you don’t have to bend or stretch over the mattress to remove the dirty linens or to put clean ones on the bed. Also, make sure the side rails are up when changing an occupied bed to keep the patient from rolling out of bed and to give the patient something to hold onto while moving from side to side.
- Before beginning the process of changing the patient’s bed linens, be sure that you have all of the necessary supplies. Try to plan ahead and bring only the linens you will actually use. You cannot place any extra linens you bring into the patient’s room back on the linen cart until after they have been laundered.
Bed making
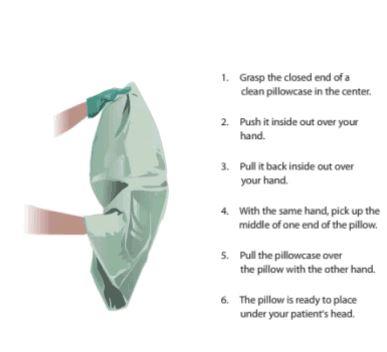
Changing Pillow Case

In addition to an open or closed bed, you’ll prepare unoccupied beds for patients who will be brought to your unit after surgery. With this type of bed, you won’t tuck in or mitre the corners. Instead, you’ll fold them to the bottom third of the bed to make transferring the patient from the stretcher to the bed easier.
After you have replaced the bed linens, lower the bed to its original position and make sure the wheels are locked to keep the patient from falling when getting in and out of bed. In addition, place the call light, bed controls, patient-controlled analgesia button, and any other devices the patient needs within the patient’s reach.
Bed making
- Encourage patients who wear dentures to care for them in the same manner as they would care for their natural teeth. Keeping dentures clean can help prevent the gums from becoming irritated and infected. To keep bacteria from building up underneath the dentures and to give the gums a rest, dentures should be removed at night.
- Before removing a patient’s dentures, be sure to break the seal on the upper denture by gently moving the denture up and down or by placing your finger on the edge of the denture and pulling down. Remove the upper denture by grasping the plate between thumb and index finger wrapped in gauze and pull downward. To remove lower denture, gently lift it from the jaw and rotate one side downward. Place dentures in emesis basin or sink.
- For patients who are unable to care for their own dentures, it is your responsibility to provide this care for them. Because dentures are the patient’s personal property and are costly to replace if broken or damaged, handle them with care when cleaning them. When preparing to clean dentures over a sink, place a towel or a washcloth in the bottom of the sink to avoid breakage if you drop them.
- When rinsing the patient’s dentures, be sure to use cool or tepid water. Avoid hot water because heat can soften the material that some dentures are made of, resulting in damage to the dentures.
- If dentures are stained, soak them in a commercial cleaner following the manufacturer’s directions. If the dentures have any metal pieces, avoid soaking them overnight as this can cause corrosion. Be sure to rinse them well before putting them back in the patient’s mouth.
- When the patient is not wearing the dentures, store them in a small amount of water in a denture cup or in a container with a lid. Label the cup with the patient’s name and room number and store it in a safe place to prevent loss. Discourage the patient from placing dentures in a napkin or a facial tissue because they can be easily mistaken as garbage and discarded.
- Because dentures improve the patient’s speech, appearance, and self-image, it’s important to put back them back in as soon as possible after oral hygiene or after the patient returns from a procedure. If the dentures are dry, moisten them with water before putting them back in the patient’s mouth. After cleaning, ask if the patient needs help inserting the dentures. Moisten the upper denture and press firmly to seal it in place. Insert the moistened lower denture.
Denture care
- Caring for the hair and scalp is important for the patient’s appearance and sense of well-being and is an essential component of personal hygiene. Hair care needs vary from patient to patient depending on health status and cultural preferences.
- Brush or comb the hair daily to remove tangles, massage the scalp, stimulate circulation to the scalp, and distribute natural oils along the shaft of the hair. Use a soft-bristled brush to prevent injury or trauma to the scalp and a wide-toothed comb or hair pick to comb through tightly curled or kinky hair.
- Begin combing the hair by dividing it into three or four sections. Then, brush or comb each section one at a time starting at the scalp and moving to the ends of the hair to minimize pulling. For tangled hair, use a wide-toothed comb and comb the tangles out from the ends of the hair toward the scalp.
- Shampooing cleans the hair and scalp and can also relax the patient. Start shampooing at the hairline and work toward the neck. To wash the hair on the back of the patient’s head, gently lift the head with one hand and shampoo with the other. Before rinsing, massage the patient’s scalp by applying light pressure with your fingertips.
- Depending on the patient’s health status, you can shampoo the hair in any of a variety of ways. If the patient is ambulatory, use the shower. If the patient is able to sit in a chair and lean back, shampoo the hair at the sink. For patients on bed rest, use a plastic shampoo trough. Dry or no-rinse shampoos and shampoo caps are also options for patients on bed rest.
- Place a folded or rolled towel behind the patient’s neck to pad the edge of the sink. Before beginning, make sure there are no contraindications to having the patient’s head and neck manipulated or extended back over the sink.
- When using a plastic shampoo trough for a patient on bed rest, place a small basin at the side of the bed to catch the water that drains from the trough. To keep the bed linens and the patient’s gown dry, place a waterproof pad underneath the trough and a towel around the patient’s shoulders. Also, place a washcloth over the patient’s eyes to protect them from the water and the shampoo.
- Another option for shampooing the hair of patients on bed rest is to use a dry shampoo, a no-rinse shampoo, or a shampoo cap. These shampoos are activated by heat and must be warmed in a microwave oven before you massage them into the patient’s hair and scalp. Although these shampoos are convenient and require minimal movement of the patient, they can make the hair and scalp dry.
Hair and scalp care
- Nail, hand, and foot care is performed on a regular basis to assess for lesions, dryness, and signs of infection. This is especially essential for patients who have peripheral vascular disease or diabetes mellitus and for patients with immunosuppression or who are otherwise at higher risk for developing foot and nail problems.
- You’ll perform nail, hand, and foot care during bathing. Soak the patient’s hands and feet in a basin of water for a short period of time while performing other hygiene procedures and then wash the hands and feet with soap and water. When drying the hands and feet, be sure to dry between each finger and each toe.
- If you trim the patient’s fingernails or toenails, cut them straight across to prevent injury or trauma to the surrounding tissue. Before cutting any patient’s nails, check your facility’s policy, as some settings and patient conditions require provider orders for foot care. In some cases, a podiatrist is required for toenail care.
- Be sure to clean underneath the patient’s nails using an orangewood stick or the end of a plastic applicator stick to remove debris that can harbor micro-organisms. Shape the nails and smooth rough edges using a nail file. Apply lotion to the patient’s hands and feet, focusing on dry or callused areas. If the patient’s hands or feet are extremely dry and the skin is cracked, use a deep-penetrating moisturizer.
- Your foot and nail care will vary from the standard when you care for a patient who has diabetes mellitus. Do not soak the feet due to the risk of infection and do not cut the nails. Instead, file them using a nail file. Do not apply lotion between the fingers or toes since the moisture can cause skin irritation and breakdown.
Nail, hand, and foot care
- Maintaining oral hygiene is important for preventing the development of plaque-related disorders. Regular oral hygiene includes brushing, flossing, and rinsing. Brushing cleans teeth of food particles, plaque and bacteria. It also massages gums and eliminates discomfort of unpleasant odors and tastes. Flossing removes tartar that collects at the gumline. Rinsing removes dislodged food particles and excess toothpaste.
- Inadequate oral care diminishes salivary production, which reduces the ability to fight effects of pathogens. Oral hygiene includes different components depending on the patient, the patient’s health status, and whether the patient has dentures or his natural teeth or both. When to offer oral care might vary with the facility, but the most common times are before breakfast, after each meal, and at bedtime. The frequency of care is also based on condition of oral cavity and patient’s level of comfort. Most often, though, oral hygiene includes brushing the teeth several times a day, flossing at least once a day, and rinsing with an antiseptic mouthwash once or twice a day. American Dental Association guidelines include brushing teeth at least twice a day with approved fluoride toothpaste and antimicrobial mouth rinse.
- A well-balanced diet is very important for developing healthy oral tissues. Patients may need to change their dietary habits. Regularly scheduled visits to the dentist for dental check-ups is advised for clients of all ages. Educating clients about common gum and tooth disorders and methods of prevention motivates them to follow good oral hygiene practices. Poor oral health is linked to risk of impaired nutrition, stroke, poor blood sugar control in diabetes, and nursing home-acquired pneumonia.
- When oral hygiene is not performed correctly or often enough, oral health problems can develop. The most common of these are plaque and tartar build-up, tooth decay, gingivitis, and periodontitis. Plaque is a soft, sticky, colorless substance that forms on the hard, rough surfaces of the teeth. If plaque is not removed and accumulates on the teeth, the gums can become irritated, the outer enamel of the teeth can be destroyed, and halitosis can develop.
- Another common dental problem resulting from the accumulation of plaque on the patient’s teeth is tooth decay, also known as dental caries or cavities. It is caused by the acid in the plaque’s bacteria destroying the outer surfaces of the tooth.
- Gingivitis is the early stage of periodontal disease. It involves inflammation of the gums and often times bleeding when the patient brushes and flosses the teeth. With proper oral hygiene, which includes both brushing and flossing, gingivitis can usually be reversed.
- If gingivitis is left untreated, periodontitis develops. This gum disease destroys the supporting structures of the teeth, including bone, and is characterized by red, swollen, bleeding gums.
Oral hygiene
- Perineal care is a part of a complete bed bath. Patients who are at risk for infection are most in need of perineal care. These are usually uncircumcised male patients, those with indwelling urinary catheters, or those recovering from rectal or genital surgery or childbirth, or women who are having a menstrual period. Patients need to be encouraged to perform their own care. Embarrassment can be a major deterrent for the nurse for performing perineal care. A gender-congruent nurse can perform this care efficiently. It is important to maintain a professional, straightforward attitude and to protect the patient’s privacy at all times during this procedure.
- Because your hands will come into contact with mucous membranes and possibly body fluids when you provide perineal care, follow standard precautions at all times. Not only does this protect you, but it also protects the patient.
- Perineal care is often included in bathing and involves cleaning the perineum, the external genitalia, and the surrounding skin. For patients who are recovering from rectal or genital surgery or from childbirth or for those who have an indwelling catheter, you might have to provide perineal care frequently to prevent skin breakdown, infection, and odor. Inquire about complaints of burning during urination or localized soreness, excoriation, or pain in the perineum. The vaginal and perineal areas can be inspected at this time, as well as noting any abnormal odors.
- Before beginning perineal care, position the bed at a comfortable working height. Position the patient with knees bent and legs slightly apart, unless contraindicated. This position exposes the areas you will clean and allows for more thorough bathing.
- While providing personal hygiene, keep the patient covered as much as possible to maintain privacy and comfort and to keep the patient warm. Before beginning perineal care, drape the area with a bath blanket or a towel. Your technique will vary depending on whether the patient is male or female.
Perineal care
- Shaving is often a component of personal hygiene care. For male patients, shaving is done after the bath or after you’ve shampooed the hair. Female patients need the hair on the legs and axillae shaved during bathing. Depending on the patient’s hair growth and personal preference, daily shaving might be required.
- For patients taking anticoagulants or high doses of aspirin or for those with low platelet counts or bleeding disorders, use an electric razor. Before using it, though, make sure it is in good working condition and will not harm the patient. Check your facility’s policy about using the patient’s electric razor or a hospital-issued electric razor. Check the razor for frayed cords or other electrical hazards.
- When using a disposable razor, be sure the patient’s skin is soft before beginning to shave it. To accomplish this, place a warm washcloth over the patient’s face for a few seconds before applying shaving cream. Softening the skin first helps prevent pulling, scraping, or cutting the skin during shaving. When patients are unable to shave themselves, the nurse will have to shave for them.
- To avoid causing discomfort and to reduce the risk of cutting the patient’s skin during shaving, pull the skin taut and use long, firm strokes to shave the larger areas of the face and short downward strokes to shave around the chin and lips. Shaving in the direction of hair growth is also helpful. Clients with tightly curled or kinky hair may experience ingrown hair, so they need to be shaved close to the skin.
- If the patient has a beard or mustache, he might need daily grooming. It is important to keep these areas clean, since food particles and mucus can collect in the hair. Comb and trim the patient’s beard and mustache as necessary. However, it is inappropriate to shave a patient’s beard or mustache off without the patient’s permission to do so
Shaving