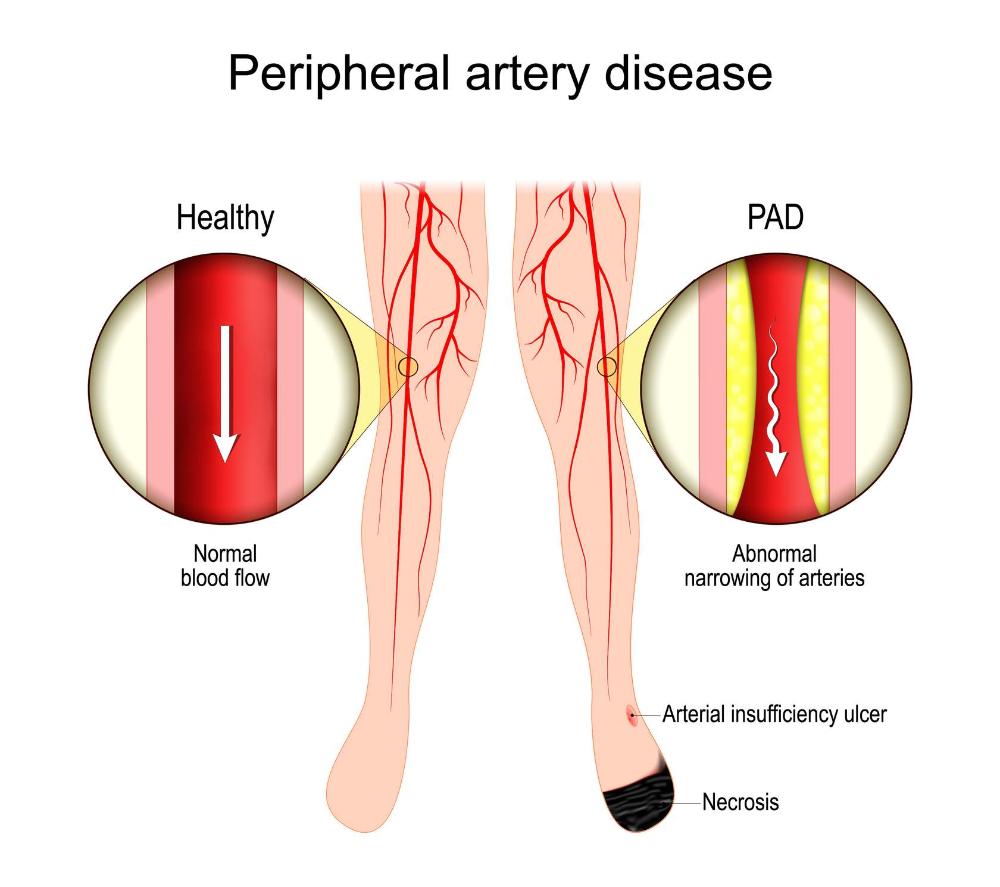
Lower extremity arterial disease (___) is a progressive narrowing or blockage of arteries in the lower limbs, often due to atherosclerosis (McNichol et al., 2021). It is commonly associated with PAD and defined by an ABI < 0.9, leading to ischemia in the lower leg.
LEAD
____ leg ulcers are often triggered by trauma, such as blunt force or chronic pressure from improperly fitting footwear.
Arterial
PAD
Critical Limb Ischemia
Is the most severe form of LEAD, where blood flow is so poor that tissues cannot survive (DynaMed, 2022). Most individuals with CLI also have diabetes. Without appropriate revascularization, these patients often face amputation, with the risk increasing as their ABI decreases.
Risk Factor for Arterial Disease Modifialble:
- Smoking
- Diabetes
- Dyslipidemia
- Hypertension
- Obesity
- Inactivity
- Stress
Risk Factor for Arterial Disease
- Age
- Male assigned at birth
- Postmenopausal status
- Family history of cardiovascular disease
- Race, specifically Black
Is the VLU, or ALU?
ALU
Wound Edges
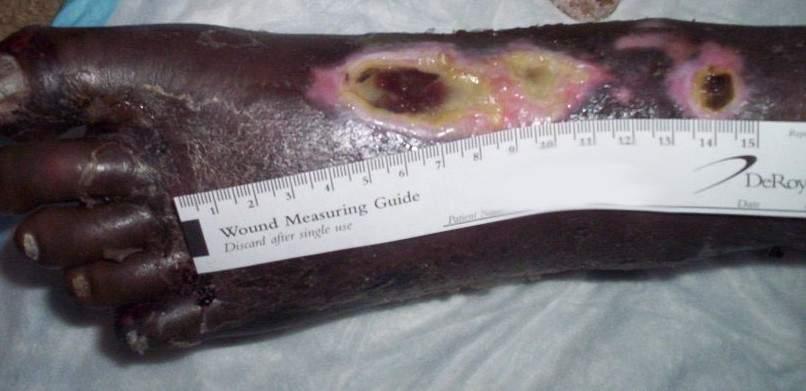
They have a well-defined, round, or "punched-out" appearance with sharply demarcated edges.
ALU characteristics
* well-defined, round, or "punched-out" appearance with sharply demarcated edges.
Wound bed pale, gray, or yellowish due to the lack of oxygen-rich blood reaching the area. The wound bed may also be dry and necrotic, with necrotic tissue ranging from thick black eschar to slough.
* Minimal exudate because of lack of blood supply
* Periwound Periwound -This is often thin, shiny, dry, and cool to the touch.
What does ABI stand for and mean?
An ankle-brachial index (ABI) is a painless test that measures blood pressure in your ankles and arms. It shows if you have peripheral artery disease (PAD), or plaque buildup in your leg arteries. Your ABI is the blood pressure in your ankle divided by that in your arm. * Can catch PAD before it gets severe!
When is an ABI test needed?
- if you have PAD symptoms, like leg pain when active. Your PCP may also suggest this test if you don’t have symptoms but are:
- Age 65 or older
- Age 50 to 64 and have certain risk factors for atherosclerosis (like diabetes, high blood pressure, high cholesterol, history of tobacco use) or a history of PAD in your biological family
- Under age 50 and have diabetes along with another risk factor for atherosclerosis
Below are preparations for what kind of test/procedure?
- Don’t eat or drink anything that contains caffeine on the day of your test.
- Don’t use tobacco products or alcohol during the hour before your test.
- Don’t exercise during the hour before your test.
- Wear loose, comfortable clothes so your provider can easily access your upper arms and ankles.
- Just before the test, go to the restroom and pee until your bladder is empty.
Be sure to tell your provider if you’ve had any procedures to improve circulation in your legs. This may affect how they do the test.
ABI test
What is this formula?
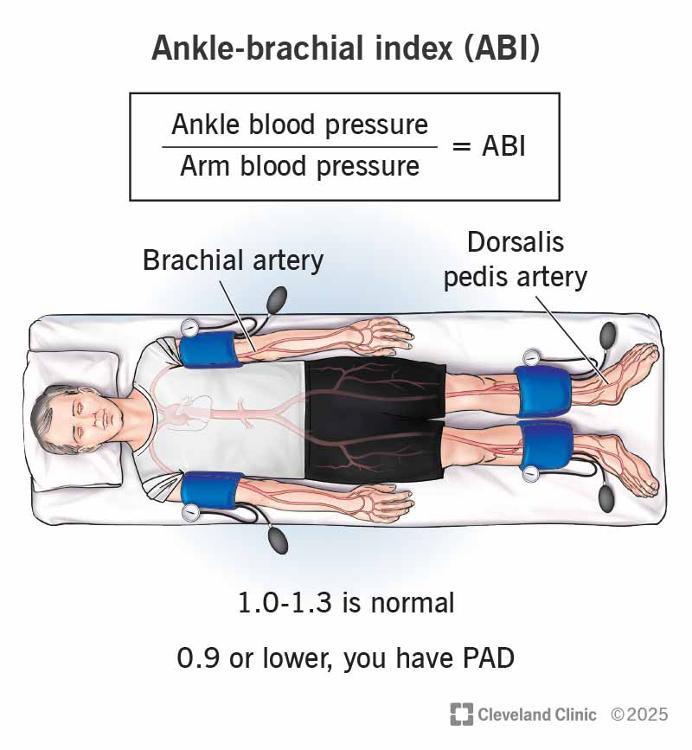
Ankel-Brachial Index
ABI: Ranges
_._-__._ is normal range
_._ or lower, you have PAD
1.0-1.3 is normal
0.9
What do these ABI results mean?
- 1.0 to 1.3: Normal
- 0.9 to 1.0: Borderline
- 0.7 to 0.9: Mild PAD
- 0.4 to 0.7: Moderate PAD
- Lower than 0.4: Severe PAD
Normal
Borderline
Mild PAD
Moderate PAD
Severe PAD
ABI Range:
Lower that 0.4 means?
Severe PAD
ABI Range:
0.4 to 0.7 means?
Moderate PAD
ABI Range:
1.0 to 1.3 means?
Normal
ABI Range:
0.9 to 1.0 Borderline
Borderline PAD
When your arteries are calcified, an ___ test can't reliably diagnose PAD. Other options Toe- Brachial (big toe)
ABI
Researchers found that people with an ankle-brachial index higher than 1.4 have in increased risk of _____ ____
CARDIOVASCULAR DEATH
Ulcer Stages:
Supervicial Ulcer
Grade 1
Superficial ulcer w/out subcutaneous tissue involvement
Ulcer Stages:
DEEP ULCER
Grade 2
Involves ligament, tendon, joint capsule, or deep fascia but no abscess or osteomyelitis
Ulcer Stages:
Osteitis
Grade 3
Deep wound with abscess or osteomyelitis
Ulcer Stages:
Partial gangrene
Grade 4
Gangrene affects a portion of the foot
Ulcer Stages:
Gangrene
Grade 5
Gangrene affects entire foot
Wagner Scale (Meggitt-Wagner)
The Wagner Scale, also known as the Meggitt-Wagner classification, is a simple grading system used to evaluate the severity of DFUs (DynaMed, 2024b).
The Meggitt-Wagner classification, is a simple grading system used to evaluate the severity of DFUs (DynaMed, 2024b). It classifies ulcers based on:
- Depth of the wound.
- If the wound is infected.
- The amount of tissue necrosis.
Which component of the blood is primarily involved in forming the initial phase of a blood clot during wound healing?
Red blood cells
Platelets
White blood cells
Plasma proteins
...
Which type of white blood cell is most abundant and acts as the first responder to bacterial infection?
Lymphocytes
Neutrophils
Eosinophils
Monocytes
...
What role does melanin play in protecting the skin from ultraviolet radiation?
Acts as a physical barrier by scattering and absorbing UV rays to decrease penetration
Increases transepidermal water loss to cool the skin
Produces antimicrobial peptides to defend against sun-induced pathogens
Stimulates the production of sweat to enhance evaporation cooling
...
What is the average pH of the acid mantle of an adult’s skin?
5.5
0 to 4.5
7.1 to 14
7.0
...
Which layer of the epidermis is responsible for producing new cells through mitosis?
Stratum Lucidum
Stratum Spinosum
Stratum Germinativum
Stratum Granulosum
...
Which choice BEST describes the function of tendons?
Attaches bone to bone
Connects muscle to bone
Provides a surface for bones to glide over
Surround muscles to reduce friction
...
What BEST describes the characteristics of healthy skeletal muscle?
White and shiny in appearance
Pearly white ribbon-like appearance
Pink to dark red in color with striation
Pale pink without striation
...
What is the primary composition of fascia?
Adipose tissue
Collagen
Keratin
Muscle tissue
...
What protein gives red blood cells the ability to transport oxygen?
Fibroblasts
Hemoglobin
Macrophage
Mast Cells
...
What BEST describes the responsibilities of collagen and elastin in the skin?
Transporting nutrients and waste products through the dermis
Killing parasites and helping with allergic responses
Protecting skin integrity and preventing water loss
Providing tensile strength and recoil to the skin
...
What best describes what “Skin of Color” refers to?
A specific skin type that is only found in tropical regions
Skin that tans easily and rarely burns under sun exposure
The broad range of skin types and complexions of individuals not of White descent
Skin that is overly sensitive to ultraviolet radiation and prone to sunburn
...
Which of the following best describes a systematic head-to-toe skin assessment?
Examining only the areas around and under medical devices
Inspecting and palpating the skin, focusing on bony prominences and skin folds
Using only visual inspection to assess the skin
Checking the patient’s clothing for signs of moisture
...