Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Path 18
front 1 Hepatitis ___: This is typically an acute, short-term infection spread through contaminated food or water that does not lead to chronic liver disease. | back 1 A |
front 2 Hepatitis ___: It is transmitted through infected blood, sexual contact, or from mother to child during birth and can transition from an acute illness into a lifelong chronic infection (but rarely) | back 2 B |
front 3 Hepatitis ___: Primarily spread through blood-to-blood contact (often via shared needles), this type is notorious for being a "silent" infection that becomes chronic in the majority of cases. | back 3 C |
front 4 Hepatitis ___: This unique "satellite" virus can only infect people who already have Hepatitis B, as it requires the B virus to replicate. | back 4 D |
front 5 Hepatitis ___: Similar to Type A, it is usually spread via the fecal-oral route through tainted water and is generally acute, though it poses a significant risk to pregnant women. | back 5 E |
front 6 A patient is developing jaundice from rising
bilirubin levels. Which finding is most likely to appear
first on physical exam? | back 6 B. Yellow discoloration of sclera |
front 7 A patient has chronic hemolysis with
increased bilirubin production that exceeds
the liver’s conjugating capacity. Which condition best
explains this mechanism? | back 7 A. Extravascular hemolysis causing jaundice |
front 8 A patient with anemia develops jaundice and is noted to have a higher
risk of pigmented bilirubin gallstones. Which
underlying process best fits this presentation? | back 8 B. Increased bilirubin production from hemolysis this is Extravascular hemolysis causing jaundice |
front 9 A jaundiced patient has dark urine, but the bilirubin responsible for
the jaundice itself is not present in the urine because it is not
water soluble. What most likely explains the dark
urine? | back 9 B. Increased urinary urobilinogen excretion |
front 10 A newborn develops jaundice shortly after birth because the
liver temporarily has low activity of UGT needed
for bilirubin conjugation. What is the most likely
diagnosis? | back 10 C. Physiologic jaundice of the newborn |
front 11 A neonate with severe jaundice is at risk for bilirubin deposition in
the basal ganglia, causing permanent
neurologic injury. Which complication is this? | back 11 A. Kernicterus Physiologic jaundice of the newborn |
front 12 A newborn with jaundice is treated with light exposure that converts
UCB into a more water-soluble form. Which treatment was used? | back 12 B. Phototherapy Physiologic jaundice of the newborn |
front 13 A healthy young adult has intermittent jaundice only during periods
of physiologic stress, such as severe
infection. The disorder is otherwise not clinically
significant. Which diagnosis is most likely? | back 13 B. Gilbert syndrome |
front 14 A patient has an inherited disorder caused by mildly
decreased UGT activity and is otherwise
asymptomatic except during stress. What is the inheritance
pattern of this condition? | back 14 D. Autosomal recessive this is Gilbert syndrome |
front 15 An infant has a complete absence of UGT1A1 activity
and rapidly develops severe neurologic injury from bilirubin
deposition. Which syndrome is most likely? | back 15 B. Crigler-Najjar syndrome |
front 16 A child has profound jaundice due to complete failure of
bilirubin conjugation and develops
kernicterus. What is the usual prognosis without effective
intervention? | back 16 C. Usually fatal |
front 17 A patient has an inherited defect in the canalicular
transport protein (MRP2) that normally moves
bilirubin into bile. Which diagnosis is most
likely? | back 17 A. Dubin-Johnson syndrome |
front 18 A patient with chronic jaundice is found incidentally to have a
darkly pigmented liver, but is otherwise largely
asymptomatic. Which syndrome best fits this picture? | back 18 A. Dubin-Johnson syndrome |
front 19 A patient has a disorder very similar to Dubin-Johnson syndrome but
lacks liver discoloration. Which diagnosis is this comparison
describing? | back 19 B. Rotor syndrome |
front 20 A patient presents with jaundice, intense itching, pale
stools, and dark urine. Which mechanism best explains this
presentation? | back 20 C. Obstruction of bile flow to intestine Biliary tract obstruction |
front 21 A patient with jaundice is also found to have
xanthomas and pruritus due to
retained bile acids. Which disease process most
strongly fits this constellation? | back 21 B. Biliary tract obstruction |
front 22 A patient with obstructive jaundice develops greasy
stools and deficiency of fat-soluble
vitamins. What is the most direct explanation? | back 22 A. Failure of bile delivery impairs fat absorption Biliary tract obstruction |
front 23 A patient with jaundice is found to have a biliary obstruction. Which
underlying cause is specifically associated with this disorder? | back 23 C. Clonorchis sinensis infestation Biliary tract obstruction |
front 24 A patient develops jaundice in the setting of pancreatic
carcinoma compressing the biliary tree.
Which broader category does this belong to? | back 24 A. Obstructive jaundice |
front 25 A patient with liver inflammation develops jaundice because
both hepatocytes and small bile ductules
are disrupted. Which diagnosis best fits this
mechanism? | back 25 B. Viral hepatitis |
front 26 A patient with jaundice has dark urine, but the
mechanism is increased urinary bilirubin rather than
increased urinary urobilinogen. Which diagnosis
best fits that distinction? | back 26 C. Viral hepatitis |
front 27 what two are only increased in Conjucated Bilirubin? | back 27 dubin-johnson biliary tract obstruction |
front 28 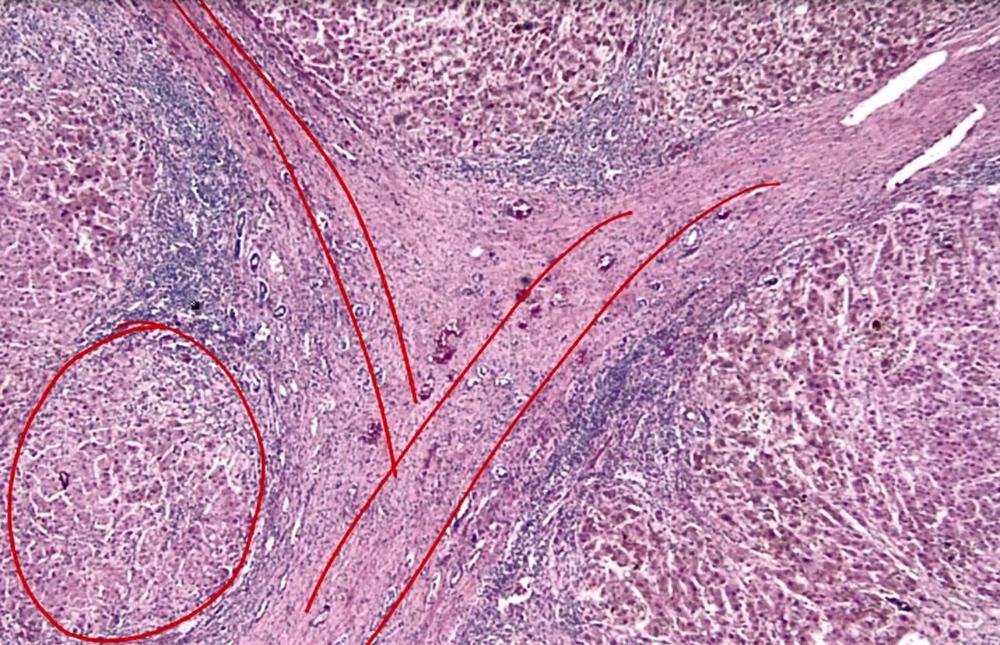 what is this? | back 28 cirrhosis |
front 29 A male patient with chronic liver disease develops gynecomastia,
spider angiomata, and palmar erythema. What is the most likely cause
of these findings? | back 29 B. Decreased hepatic metabolism of circulating estrogen |
front 30 A patient with liver failure develops jaundice. Which mechanism best
explains this presentation? | back 30 C. Decreased metabolism of unconjugated bilirubin |
front 31 A patient with cirrhosis presents with confusion and
a flapping tremor of the hands. Which underlying
mechanism best explains these neurologic findings? | back 31 A. Accumulation of ammonia due to impaired detoxification |
front 32 rmbr that the liver does protein synthesis and clotting factor synthesis, so messed up liver would lead to | back 32 less protein/albumin bleeding |
front 33 is pt or ptt used to monitor cirrhosis liver destruction | back 33 pt similar to warfarin |
front 34 alcohol-related liver disease: damage to hepatic ______ due to consumption of alc | back 34 parenchyma |
front 35  ______ ______ | back 35 fatty liver |
front 36 A patient presents with acute liver injury after a weekend of heavy
binge drinking. The hepatocyte damage is primarily mediated by
accumulation of which toxic metabolite? | back 36 A. Acetaldehyde |
front 37 A patient with alcoholic hepatitis develops liver injury due to a
toxic intermediate formed during ethanol metabolism. Which step in
ethanol metabolism produces this harmful compound? | back 37 A. Conversion of ethanol to acetaldehyde |
front 38 A patient with a history of heavy alcohol use presents with
right upper quadrant pain and
hepatomegaly. Laboratory studies show
elevated transaminases with AST significantly higher than
ALT. What is the most likely explanation for this enzyme
pattern? | back 38 A. Preferential mitochondrial injury increasing AST release |
front 39 A patient with obesity and no history of alcohol use
is found to have elevated liver enzymes on routine testing. Further
evaluation excludes viral, toxic, and other known causes of
liver injury. Which diagnosis best fits a disorder that can
range from simple fatty change to hepatitis and eventually
cirrhosis? | back 39 B. Nonalcoholic fatty liver disease |
front 40 An obese patient with chronically elevated transaminases undergoes
evaluation for liver disease. He denies alcohol use, and
workup for other known hepatic insults is negative. Which
laboratory pattern would most support the suspected diagnosis? | back 40 C. ALT greater than AST |
front 41 A 52-year-old man presents with fatigue, joint pain, and mild
hepatomegaly. Labs show elevated liver enzymes. Over time, he
develops diabetes and restrictive cardiomyopathy.
Liver biopsy shows iron deposition within
hepatocytes. Which mechanism best explains the cellular
injury leading to this patient’s organ dysfunction? | back 41 B. Free radical formation causing lipid membrane damage hemochromatosis |
front 42 primary or secondary hemochromatosis? damage to the HFE gene, most commonly C282Y | back 42 primary |
front 43 primary or secondary hemochromatosis? complications of transfusions | back 43 hemochromatosis |
front 44 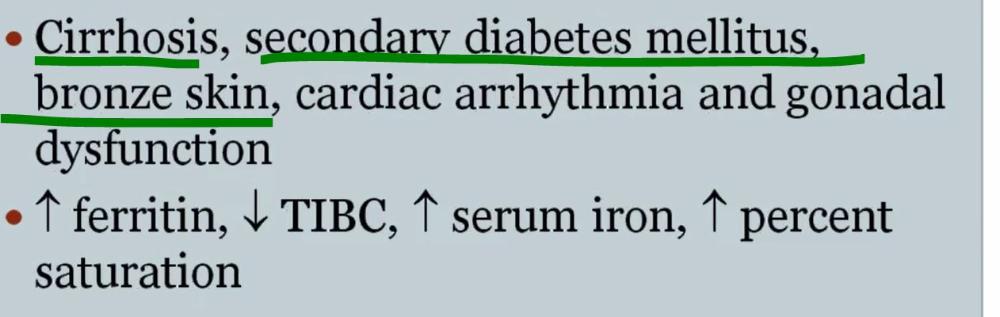 | back 44 hemochromatosis |
front 45 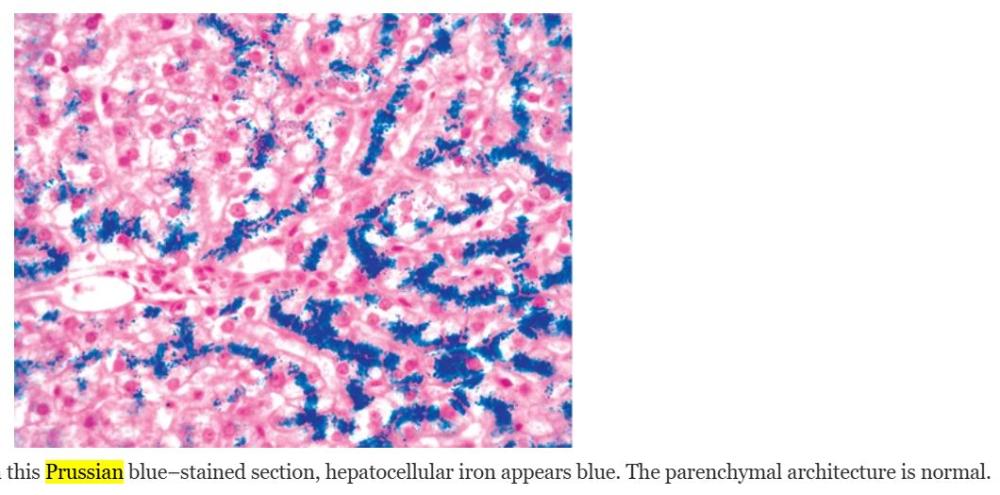 | back 45 hemochromatosis |
front 46 A patient is diagnosed with an inherited disorder affecting
copper handling in hepatocytes. The mutation
disrupts an ATP-dependent transport process. Which
immediate consequence most directly results from this defect? | back 46 A. Failure to transport copper into bile |
front 47 A patient with an autosomal recessive defect in the
ATP7B gene has impaired copper
metabolism. Which combination of abnormalities best reflects
the primary defect in hepatocyte function? | back 47 B. Decreased copper incorporation into ceruloplasmin |
front 48 A patient with a copper metabolism disorder develops
progressive liver dysfunction and later presents
with confusion and movement abnormalities. Which
additional finding would most strongly support the same underlying
disease process? | back 48 A. Kayser-Fleischer rings in the cornea |
front 49 Best initial treatment for Wilson disease: | back 49 C. Copper chelators (penicillamine, trientine) |
front 50 Typical diagnostic profile in Wilson disease: | back 50 B. ↓Ceruloplasmin, ↑urine copper |
front 51 Hereditary hemochromatosis is mainly a disorder of: | back 51 B. Excessive copper storage |
front 52 The commonest HH mutation: | back 52 A. Frameshift in HFE promoter |
front 53 HFE normally binds the transferrin receptor to help induce: | back 53 C. Hepcidin |
front 54 In HH, decreased hepcidin leads to: | back 54 A. Increased free iron |
front 55 HH is usually inherited as: | back 55 D. Autosomal recessive |
front 56 A middle-aged patient presents with fatigue and
pruritus. Liver biopsy shows lymphocytic and
granulomatous destruction of small intrahepatic bile ducts
(florid duct lesion). Which mechanism best explains
the underlying pathogenesis of this condition? | back 56 A. T cell–mediated autoimmune destruction of bile ducts Primary biliary cholangitis |
front 57 A patient with chronic cholestatic liver disease
undergoes biopsy showing bile duct destruction and hepatocytes with
feathery degeneration. What is the most direct
cause of this hepatocyte change? | back 57 A. Accumulation of bile components within hepatocytes |
front 58 A patient with inflammatory bowel disease develops progressive
cholestasis. Which additional finding would most strongly support a
diagnosis of primary sclerosing cholangitis? | back 58 A. Association with HLA alleles and autoantibodies |
front 59 A patient with chronic cholestatic liver disease is found to have
alternating strictures and dilation of
large bile ducts on imaging. Biopsy shows inflammation with
periductal fibrosis. Which mechanism best explains
the underlying disease process? | back 59 A. T cell–mediated immune injury to bile ducts This describes Primary sclerosing cholangitis. |
front 60 fulminant liver failure and encephalopathy in children with viral illness who take aspirin. related to mitochondrial damage of hepatocytes | back 60 Reye syndrome |
front 61 A 24-year-old woman using oral contraceptives is found to have a well-circumscribed benign liver mass. Which diagnosis is most likely? A. Hepatocellular adenoma | back 61 A. Hepatocellular adenoma |
front 62 Hepatocellular adenoma is most strongly associated with oral contraceptives and: A. Estrogen withdrawal | back 62 B. Anabolic steroids |
front 63 The most common liver tumor of early childhood is: A. Hepatocellular adenoma | back 63 B. Hepatoblastoma |
front 64 Widespread parenchymal injury causing zonal loss of contiguous hepatocytes is called: A. Interface hepatitis | back 64 B. Confluent necrosis |
front 65 The principal liver cell responsible for scar deposition is the: A. Kupffer cell | back 65 C. Hepatic stellate cell |
front 66 The most severe form of liver disease is: A. Steatosis | back 66 D. Liver failure |
front 67 Acute liver failure usually follows: A. Slow portal fibrosis | back 67 D. Sudden massive destruction |
front 68 Chronic liver failure more often follows: A. Insidious progressive injury | back 68 A. Insidious progressive injury |
front 69 Acute liver failure is defined by acute liver illness with encephalopathy and: A. Hyperbilirubinemia | back 69 B. Coagulopathy |
front 70 Acute liver failure must occur within what time from the initial injury? A. 12 weeks | back 70 C. 26 weeks |
front 71 Acute liver failure is usually associated with: A. Massive hepatic necrosis | back 71 A. Massive hepatic necrosis |
front 72 Chronic liver failure is most often associated with advanced fibrosis and: A. Steatohepatitis | back 72 C. Cirrhosis |
front 73 Cirrhosis features diffuse remodeling into parenchymal nodules surrounded by: A. Fat vacuoles | back 73 B. Fibrous bands |
front 74 Cirrhosis often includes a variable degree of: A. Bacterial translocation | back 74 D. Portosystemic shunting |
front 75 Grossly, cirrhosis converts the smooth liver capsule into a: A. Pale glassy sheet | back 75 C. Bumpy scarred surface |
front 76 The depressed scars and bulging nodules of cirrhosis reflect: A. Necrotizing vasculitis | back 76 B. Regeneration and fibrosis |
front 77 Portal hypertension results partly from increased resistance to portal flow at the level of the: A. Central veins | back 77 D. Sinusoids |
front 78 Portal hypertension also involves increased portal flow due to: A. Portal thrombosis | back 78 B. Hyperdynamic circulation |
front 79 Which is a major consequence of portal hypertension? A. Ascites | back 79 A. Ascites |
front 80 Another major consequence of portal hypertension is formation of: A. Regenerative nodules | back 80 B. Portosystemic shunts |
front 81 Portal hypertension commonly also causes congestive: A. Hepatomegaly | back 81 C. Splenomegaly |
front 82 Which listed consequence of portal hypertension is commonly discussed under liver failure? A. Ascites | back 82 B. Encephalopathy |
front 83 Hepatitis B can result in acute hepatitis followed by: A. Carrier conversion only | back 83 B. Recovery and clearance |
front 84 A severe possible consequence of hepatitis B is: A. Massive liver necrosis | back 84 A. Massive liver necrosis |
front 85 Hepatitis B may also produce chronic hepatitis with or without progression to: A. Steatosis | back 85 C. Cirrhosis |
front 86 Which hepatitis B outcome may be clinically silent? A. Healthy carrier state | back 86 A. Healthy carrier state |
front 87 Hepatitis C rarely causes: A. Chronic hepatitis | back 87 B. Symptomatic acute hepatitis |
front 88 Hepatitis C is the most common cause of: A. Acute liver failure | back 88 B. Chronic viral hepatitis |
front 89 Chronic hepatitis requires continuing or relapsing hepatic disease for more than: A. 3 months | back 89 C. 6 months |
front 90 Chronic hepatitis may also be defined morphologically by the presence of: A. Steatosis | back 90 B. Fibrosis |
front 91 The defining histologic feature of chronic viral hepatitis is portal inflammation with: A. Granulomas | back 91 D. Fibrosis |
front 92 The portal inflammatory infiltrate in chronic viral hepatitis is typically: A. Lymphocytic or lymphoplasmacytic | back 92 A. Lymphocytic or lymphoplasmacytic |
front 93 In chronic hepatitis B, hepatocytes may show a ground-glass appearance due to accumulation of: A. HCV core protein | back 93 B. HBsAg in ER |
front 94 Infectious agents that can involve the liver and biliary tree include bacteria, fungi, helminths, and: A. Prions | back 94 C. Protozoa/parasites |
front 95 Autoimmune hepatitis is a chronic progressive hepatitis associated with genetic predisposition, autoantibodies, and response to: A. Antibiotics | back 95 C. Immunosuppression |
front 96 Which finding supports the diagnosis of autoimmune hepatitis? A. Low serum IgG | back 96 B. Elevated serum IgG |
front 97 Diagnosis of autoimmune hepatitis requires exclusion of other etiologies such as: A. Viral hepatitis and drugs | back 97 A. Viral hepatitis and drugs |
front 98 A supportive study in autoimmune hepatitis is: A. Renal biopsy | back 98 C. Liver biopsy |
front 99 In the United States, a major cause of acute liver failure is: A. Drug- or toxin-induced injury | back 99 A. Drug- or toxin-induced injury |
front 100 The classic dose-dependent predictable hepatotoxin is: A. Isoniazid | back 100 C. Acetaminophen |
front 101 In the United States, the most common cause of acute liver failure requiring transplantation is: A. Hepatitis B | back 101 B. Acetaminophen toxicity |
front 102 Excessive alcohol intake causes steatosis and dysfunction of mitochondria, microtubules, cellular membranes, and: A. Cholangiolar transport | back 102 B. Oxidative stress pathways |
front 103 Alcohol-related liver injury ultimately leads to varying degrees of inflammation and: A. Portal granulomas | back 103 C. Hepatocyte death |
front 104 Which finding is characteristic of hemochromatosis? A. Hypopigmented skin | back 104 B. Pancreatic islet destruction |
front 105 A patient with iron overload has arrhythmias, diabetes, bronzed skin, and arthropathy. Which diagnosis is most likely? A. Wilson disease | back 105 C. Hemochromatosis |
front 106 α1-antitrypsin deficiency is characterized in hepatocytes by: A. Ground-glass cytoplasm | back 106 D. Cytoplasmic globular inclusions |
front 107 Obstruction of the major hepatic veins causing liver enlargement, pain, and ascites is called: A. Budd-Chiari syndrome | back 107 A. Budd-Chiari syndrome |
front 108 In preeclampsia, periportal sinusoids contain: A. Copper granules | back 108 B. Fibrin deposits |
front 109 In preeclampsia, hemorrhage into the space of Disse leads to periportal hepatocellular: A. Apoptosis | back 109 C. Coagulative necrosis |
front 110 Acute fatty liver of pregnancy can range from mild aminotransferase elevation to: A. Portal fibrosis only | back 110 B. Hepatic failure and coma |