Adverse Effect:
- Any undesirable, unfavorable, unintended, or dangerous reaction.
- Tylenol (Acetaminophen)
- Dark Urine
- Yellowing of the skin or eyes
- Allergic Reaction
- Difficulty breathing
- Swelling (Face, Lips, Tongue or Throat)
- Call 911
Side Effect:
- An effect that is secondary, or additional, to the on intended.
- Tylenol (Acetaminophen)
- Upset stomach
- Nausea
- Loss of appetite
- Itching
- Call HCP
Adverse Effects vs Side Effects
- Substance P
- Prostaglandis
- Bradykinis
- Histamine
Pain-mediating chemicals
- The pain impulse travels along the sensory nerve from the origin of pain in the periphery, to the dorsal horn of the spinal cord.
- IF the dorsal horn conducts the pain sensation up the spinal cord to the cerebral cortex and thalamus, it's then interpreted in relation to the location and type of pain.
- Once the brain interprets the pain, the body releases body's natural pain killers; serotonin, enkephalins, and endorphins in response to pain pain.
Sensory: Pain
There are gates in the spinal cord that open or close in relation to the conduction of pain up the spinal cord to the brain.
According to "Gate Theory"
Transcutaneous Electrical Nerve Stimulation Unit
TENS Unit stands for...
S.E.E.
- Serotinon
- Enkephalins
- Endorphins
These bind with opioid receptors and inhibit the conduction of pain impulses.
Releif of a decrease of pain is the outcome.
Body's natural pain killers

- MU
- KAPPA
- DELTA
Three types of Opioid Receptors
- Analgesia, euphoria, sedation
- Respiratory depression
- Physical dependence
> Stimulated by opioid drugs.
> They cause analgesia or relief of pain whenever receptors are stimulated.
> Stimulation causes respiratory depression, euphoria, sedation, and physical dependence.
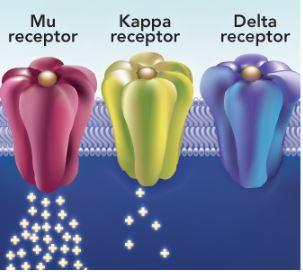
MU opioid receptor
- Analgesia, sedation
- Psychic Effects
> Stimulated by opioid drugs.
> They cause analgesia, sedation, and psychotomimetic effects whenever receptors are stimulated
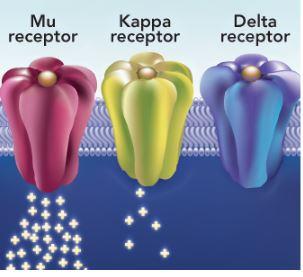
KAPPA opioid receptor
No pharmacology-related effects
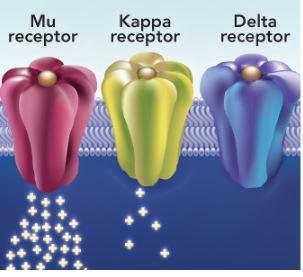
DELTA opioid receptor
- respiratory depression
- euphoria
- sedation
- physical dependence.
What are the effects that are primary concerns when administering opiod analgesics?
Effects that mimic psychosis such as hallucinations and delusion.
What is psychotomimetic effects?
> Occurs secondary to injury
- Pain
- Inflammation
- Fever
- Edema
> Chemical mediators
- Bradykinins
- Histamine
- Prostaglandins
Inflammatory Response
- Bradykinins
- Histamine
- Prostaglandins
What are the mediating chemicals released in response to cellular damage?
- Pain
- Inflammation
- Fever
- Edema
What are the local reaction to mediating chemicals?
- Substance P
- Prostaglandins
- Bradykinins
- Histamine
Substances that increase pain transmission and cause an inflammatory response.
- Serotonin
- Endorphins
- Enkephalins
Substances that decrease paint transmission and produce analgesia
- The adrenal glands produce a chemical called cortisol
- The hypothalamus stimulates the pituitary gland to release the Adreno-Cortico-Tropic Hormone (ACTH)
- ACTH then stimulates the adrenal glands to produce cortisol and the release of Aldosterone (which affetcs fluid balance in the body)
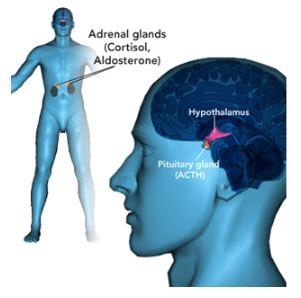
Suppression of Inflammation
> Corticosteroid
- Glucodorticoids: cortisol
- Mineralocorticoids: aldosterone
> Suppresses inflammation and immune response
ACTH stimulates adrenal glands to produce
- NSAIDs
- Opioids
Types of Analgesics
Interfere with production of prostaglandins, which in turn inhibits mild pain and suppresses inflammation.
NSAIDs
Act by stimulating opioid receptors
Opioids
- Gluccocorticoids
- Uricosurics
Type of Anti-Inflammatories
Produce a very strong anti-inflammatory effects, especially in high doses.
Glucocorticoids
Decreases the serum levels of uric acid, a chemical in the body that can cause gout.
Uricosurics
- Nonopioid analgesics
- Opioid analgesics
- Opioid antagonists
Three categories of drugs that support the treatment of pain.
- endorphin
growing or originating from within\
- morphine
substance used to treat pain
Edorphin
1 - First-generation nonsteroidal anti-inflammatory drugs (NSAIDs)
- COX-1
- COX-2 inhibitors
2 - Second-generation nonsteroidal anti-inflammatory drugs (NSAIDs)
- COX-2 inhibitors
3 - Acetaminophen (Tylenol)
4 - Centrally-acting nonopioids
Four types of Nonopiod Analgesics
- Suppress inflammation
- Treat mild to moderate pain
- Reduce fever
- Relieve dysmenorrhea
- Aspirins also inhibits platelet aggregation
1 - First-generation nonsteroidal anti-inflammatory drugs (NSAIDs)
- COX-1
- CPX-2 inhibotors
- Prototype drug:
aspirin (Advil)
ibuprofen (Mortin)
- Other drugs:
naproxen (Naprosyn, Aleve),
indomenthacin (Indocin)
Ketrolac
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Drugs
Inhibit cyclooxygenase (COX)
Cyclooxygenase converse arachidonic acid into prostaglandins
COX-1 enzyme stimulates release o protective prostaglandins (homeostasis)
- Gastric mucosal protectant
- Enhances platelet aggregation
- Promotes kidney function
COX-2 stimulates release of prosglandins secondary to injury
- inflammation
- pain
- fever
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Expected Pharmacologic Action
an enzyme that converts arachidonic acid into prostaglandis when tissue injury occurs.
Cyclooxygenase
- COX-1
- COX-2
Two forms of Cyclooxygenase
- stimulates the release of prostaglandins that work to maintain homeostatis in the body.
- they act to protect the gastric mucosa, enhance platelet aggregation, and promote renal function.
COX-1 enzyme
- stimulates the release of prostaglandins in response to injury, which results in inflammation, pain, and fever.
COX-2 enzyme
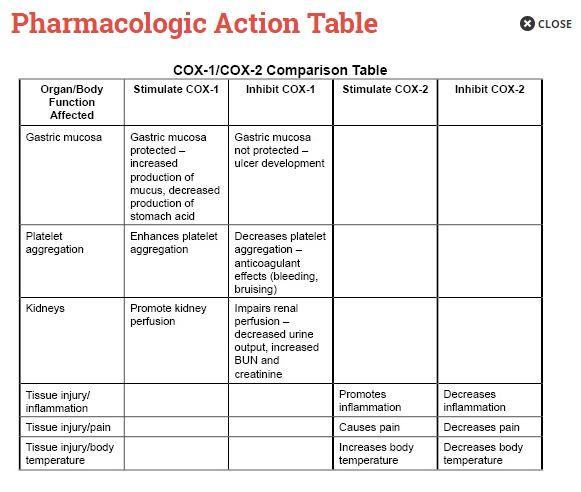
Pharmacology Action Table
- Gastric upset, heartburn, nausea, gastric ulceration
- can occur secondary to blocking the gastric mucosal protective effects of COX-1
- Bleeding (less with non-aspirin NSAIDs)
- occur for the same reason, however this occurs less with non-aspirin NSAIDs
- Kidney dysfunction
- due to NSAIDs block the protective effects of COX-1 on the kidneys
- Salicylism (aspirin)
- a buildup of aspirin in the body to toxic level, can occur if patients ingest more aspirin than they excrete.
- Reye's Syndrome (aspirin)
- a rare disorder that can occur secondary to giving aspirin to a child who has a viral infection
- Thromboembolic events (non-aspirin NSAIDs)
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Side/Adverse Effects
- Monitor signs of bleeding (black or dark-colored stools, abdominal pain, nausea, hematemesis)
- Test for and treat Helicobater pylori infection
- Recommend a proton pump inhibitor during NSAID therapy (patients who are high risk for gastric bleeding)
- Monitor for signs of easy bruising, petechiae, which are pinpoint hemorrhages just below the skin, and excessive bleeding from minor injuries such as a facisal nick wile shaving.
- Monitor I&O, BUN and creatinine (reflects a decrease in kidney function)
- Monitor for salicysism (tinnitus, dizziness, and/or headache, as well as diaphoresis (or excessive sweating) and tachypnea, which can result in respiratory alkalosis) STOP aspiring therapy immediately if these signs or symptoms arises so tha serum level of aspirin does not continue to rise.
- Recommend acetaminophen (Tylenol) for children with viral infection
- Non-aspirin NSAIDs (for short periods and in low doses to help minimize the side effects): Monitor for signs of embolic events
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Interventions
- Make sure patients swallow enteric-coated or sustained-release forms whole, and do not crush or chew them.
- Discontinue aspirin 1 week before schedule surgery
- Monitor for initial and continues therapeutic effects
- Prophylactic use of aspirin to inhibit platelet aggregation is usually 81 mg/day
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Administering
- Take with food, milk, or 8 oz of water ; avoid alcohol
- to minimize gastrointestinal effects.
- Report persistent gastric irritation, unusual or prolonged bleeding
- examples bruising, petechiae, and excessive bleeding from minor injuries.
- Report changes in urine output, weight gain, or fluid retention
- including weight gain, or signs of fluid retention such as edema or bloating.
- Do not give children or adolescents under age 19 who have viral infections.
- Let them know that they can use acetaminophen instead.
- Due to the risk of development of thrombi when taking a non-aspirin NSAID, tell patients to immediately report to the provider chest pain or heaviness, shortness of breath, sudden and sever headache, one-sided numbness, weakness, visual disturbances, or confusion.
- Non-aspirin NSAIDS: Report symptoms of embolic event; low-dose aspirin
- Reinforce the use of low-dose aspiring once daily to reduce the risk of myocardial infarction and cerebrovascular accident if the provider recommends it.
- Report tinnitus, sweating, headache, and dizziness; stop aspirin
- Also instruct the patient to report ringing or buzzing in the ears immediately, as this is the first sign of salicylism.
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Patient Instructions
ringing or buzzing in the ears, tinnitus, sweating, headache, and dizziness
What is the first sign of salicylism?
- Pregnancy risk category D, lactation
- Hypersensitivity to aspirin; NSAIDs
- Peptic ulcer disease; bleeding disorders
- Children or adolescents with a virus
- Prior to surgery
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Contraindications
- Older adults
- Cigarette smoking, alcohol use disorder
- Helibacter pylori infection
- Heart failure, advanced kidney dysfunction
- Hypertension (non-aspirin NSAIDs)
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Precautions
- Anticoagulants, glucocorticoids, and alcohol increase the risk of bleeding
- Ibuprofen decreases the antiplatelet effects of low-dose aspirin
- ACE inhibitors and angiotensin receptor blockers increase the risk of kidney failure
- Antihypertensice effects of ACE inhibitors decrease
- The risk of lithium carbonate (Lithobid) and methotrexate toxicity increases.
1) NSAIDs (COX-1 and COX-2 Inhibitors) - Interactions
- Analgesia for mild to moderate pain
- Inflammation suppression
- Fever reduction
- Dysmenorrhea
2) NSAIDs (COX-2 Inhibitor)
Celecoxib (Celebrex)
- the only true COX-2 inhibitor still on the market
Taken off the market due to increase of myocardial infarctions, heart attacks and cerebrovascular accidents, or strokes.
Rofecoxib (Vioxx)
Valdecoxib (Bextra)
2) NSAIDs (COX-2 Inhibitor) - Prototype/other Drugs
- Developed in the hopes that COX-1 inhibition related side effects would be minimized
- Some COX-1 related side effects were decreased while other were increased
- Gastric related side effects are less
- Kidney impairment side effects are similar
- Vasoconstriction combines with platelet aggregation increases risk of cardiovascular events
- COX-2 effects
- suppress pain
- suppress inflammation
2) NSAIDs (COX-2 Inhibitor) - Expected Pharmacologic Action
- Gastric upset, diarrhea, heartburn, nausea, gastric ulceration (less than with COX-1 inhibitor)
- Renal dysfunction
- Cardiovascular and cerebrovascular events
2) NSAIDs (COX-2 Inhibitor) - Side/Adverse Effects
- Monitor for an report gastric upset, heartburn, nausea, diarrhea, and GI bleeding
- Test for an treat Helicobacter pylori infection prior to long-term therapy
- For patients with high risk for gastric bleeding, recommend a proton pump inhibitor
- Monitor intake and output; watch for low urine output and fluid retention
- Monitor for rapid rises in BUN and creatinine
- Recommend the drug for short periods and in low doses only
- Recommend low-dose aspirin to prevent these events
- Monitor for signs of myocardial infarction and cerebrovascular accident
2) NSAIDs (COX-2 Inhibitor) - Interventions
When administering celecoxib (celebrex)
- Give 2 hour or after magnesium- or aluminum-based antacids
- Monitor for initial and continued therapeutic effects
2) NSAIDs (COX-2 Inhibitor) - Administration
Long-term NSAID therapy with a COX-2 inhibitor drug.
- Take low-dose aspiring once daily to reduce the risk of heart attach and stroke
- Take with food, milk, or 8 oz to minimize gastrointestinal effects
- Avoid alcohol
- Report persistent gastric irritation and signs of bleeding
- Report changes in urine output, weight gain, or signs of fluid retention such as edema or bloating
- Report chest pain or heaviness, shortness of breath, sudden and severe headache, numbness, weakness, visual disturbances, or confusion
2) NSAIDs (COX-2 Inhibitor) - Patien Instructions
- Pregnancy risk category D (third trimester; C in first and second trimesters
- Severe hepatic or kidney impairment
- Children younger than 18 yr
- Gastrointestinal bleeding, anemia
- Pain from coronary artery bypass gradting
- Allergy to sulfa, sulfonamides or celecoxib
2) NSAIDs (COX-2 Inhibitor) - Contraindication
- Alcohol use disorder
- Heart failure, cardiovascular disease, hypertension
- diabetes mellitus
- Asthma
- History of GI bleeding or peptic ulcer disease
- Mild or moderate live/kidney impairment
- Cerebrovascular accident
2) NSAIDs (COX-2 Inhibitor) - Precautions
- Diuretic effects of furosemide (Lasix) decrease
- Flucconazole (Diflucan) increases celecoxib levels
- Anticoagulant effects of warfarin (Coumadin) increase
- Glucocorticoids and alcohol increase the risk of bleeding
- Antihypertensive effects of ACE inhibitors decrease
- Risk of lithium carbonate (Lithobid) toxicity increases.
2) NSAIDs (COX-2 Inhibitor) - Interactions
- Non-opioid
- treats mild to moderate pain
- reduces fever
3) Acetaminophen
Acetaminophen (Tylenol)
- it is its own prototype drug
- provides many of the same benefits as COX-1 and COX-2 inhibitors, but without serious side effects when you give it in therapeutic doses.
3) Acetaminophen - Prototype/other Drugs
- COX inhibitor in the CNS (Central Nervous System)
- relieves pain
- reduces fever
- No peripheral inhibition
3) Acetaminophen - Expected Pharmacologic Action
Liver damage (overdose)
Hypertension (with daily use, particularly women)
3) Acetaminophen - Side/Adverse Effects
- Monitor for early symptoms of overdose or poisoning.
- abdominal discomfort, nausea, vomiting, sweating, and diarrhea.
- when giving in toxic dosages, liver damage can occur in only 48 to 72 hours
- IF overdose does occur, prepare to administer acytylcysteine (Mucomysts, Acetadote) orally of IV to counteract overdose and reduce liver injury
- Always monitor the blood pressure of patients taking acetaminophen on regular basis, especially women taking drug.
3) Acetaminophen - Intervensions
- Administer orally or rectally
- Do not administer more than 3 g per day (adults and children over 12 years of age)
- Infants and children should be given the manufacturer's recommended dose based on their age
- typical dose is less than 1 mL.
- Parents must be careful to give the dose prescribed to their infant because the risk for accidental overdose is high if infants don't get the appropriate dose.
- Caution patients that the drug is available in many combination products as well as many formulations; they must read labels carefully to avoid overdose.
3) Acetaminophen - Administration
- Do not exceed 3 g per day for adults and children over 12
- Infants and children under 12 should take the manufacturer's recommended dose based on their age.
- Report any abdominal discomfort, nausea, vomiting, sweating, or diarrhea immediately as this could indicate a possible overdose
- Have blood pressure checked regularly (especially women)
3) Acetaminophen - Patient Instructions
- Alcohol use disorder
- due to the potential for each to have an adverse effect on the liver.
3) Acetaminophen - Contraindications
- Anemia
- Immunosuppression
- Hepatic or kidney disease
3) Acetaminophen - Precautions
Alcohol increases the risk of liver injury (with high doses of acetaminophen)
Warfarin (Coumadin) increases the risk of bleeding
Cholestyramin (Questran reduces absoroption
3) Acetaminophen - Interactions
Treats moderate to moderately severe pain.
4) Centrally Acting Nonopioids
Tramadol (Ultram)
* there are other types of drugs that treat pain by acting on the CNS, but this module focuses only on tramadol.
4) Centrally Acting Nonopioids - Prototype/Other Drugs
- They bind to selected opioid receptors
- They block re-uptake or norepinephrine and serotonin in the CNS
4) Centrally Acting Nonopioids - Expected Pharmacologic Action
Side effects of tramadol are rare
- Sedation, dizziness
- Headache, nausea, vomiting, constipation
- Respiratory depression (rare)
- Seizures (rare)
- Urinary retention
4) Centrally Acting Nonopioids - Side/Adverse Effects
- Monitor patients when ambulating
- Recommend the lowest possible effective dose and short-term only
- to minimize the side effects of headache, nausea, vomiting, and constipation.
- Give with food
- Recommend an antiemetic if nausea or vomiting occurs frequently
- Measure baseline vital signs; monitor respirations
- For respiratory rates below 12 per minute, stimulate breathing
- Administer an opioid antagonist such as naloxone to restore respiratory rate
- Nalaxone might only be moderately effective in reversing respiratory depression cause by Tramadol, so the best intervention is prevention.
- Monitor for signs of seizure activity; institute precautions if indicates
- airway and suction equipment readily available as well as padding for the side rails and headboard.
- Monitor for urinary retention
4) Centrally Acting Nonopioids - Interventions
- Be aware that it take 1 hours for the analgesic effect to begin
- anticipate when patients will need their next dose in order to facilitate timely dosing that prevents recurrence of pain.
- Make sure patients swallow the extended-release form whole and do not crush or chew them.
4) Centrally Acting Nonopioids - Administration
- Do not take prior to driving or activities requiring mental alertness
- Stir or lie down if feeling lightheaded
- Change positions gradually
- Increase fluid and fiber exercise (in case of constipation)
- Take the drug only when needed and short-term
- to minimize the risk of side effects such as respiratory depression.
- Report urinary retention to provider
4) Centrally Acting Nonopioids - Patient Instructions
- Acute intoxication with alcohol, opioid, psychotropic drugs
- Seizure disorders
- Respiratory depression
- Children younger than 16 yr
4) Centrally Acting Nonopioids - Contraindications
- Substance abuse history
- Liver or kidney disease
- Increased intracranial pressure
- Older adults
4) Centrally Acting Nonopioids - Precautions
- Monoamine Oxidase Inhibitors (MAOIs) pose a risk for hypertensive crisis
- Selective serotonin-norepinephrine reuptake inhibitors, tricyclic antidepressants, MAOIs, and triptans pose a risk for serotonin syndrome
- Responses to CNS depressants increase
- Carbamazepine (Tegretol) decrease levels
- St. John's wort increases sedative effects
4) Centrally Acting Nonopioids - Intereactions
- Opioid agonists
- Opioid agonist-antagonists
Two type of opioid analgesics that support the treatment of pain.
- Bind to MU and KAPPA receptors, simultaneously stimulating and blocking their analgesic effects.
- Not as effective at reducing pain as opioid agonists, but they do serve as an alternative to opioids for patients addicted to opioids or women in labor.
Opioid agonist-antagonists
- Serves as an analgesic for moderate to severe pain.
- may also cause sedation and reduce anxiety in preoperative patients.
- Binds primarily to MU-type opioid receptors to produce their analgesic effects
- Opioid agonists
- Morphine
- Other drugs:
- Fentanyl (Sublimaze)
- Meperidine (Demerol) - synthetic opioid once given to a regular basis for postoperative pain. It reacts with many other drugs. Not well tolerated by older adults. Usually only an option for patients who can't tolerate other opioids.
- Methadone (Dolophine) - synthetic opioid that's chemically similar to morphine, but it's only used primarily as a substitute for opioids in drug abuse programs. Blocks the euphoric effects of opioids and reduces craving in people addicted to a drug in this group.
- Codeine, Oxycodone (OxyCotin, Percodan)
- Hydrocodone (Vicodin, Lortab)
- Opioid agonists - Prototype/Other Drugs
- Mimics actions of naturally occurring opioids (endrophons, enkephalins)
- Binds with MU receptors
- Stimulation of these receptors causes:
- Analgesia
- Sedation
- Euphoria
- Respiratory depression
- Opioid agonists - Prototype/Other Drugs
- Respiratory depression
- Sedation, dizziness, lightheadedness, drowsiness
- Constipation
- because they decrease intestinal motility
- Nausea, vomiting
- Orthostatic hypotension
- due to dilating effects on peripheral vasculature.
- Urinary retention
- due to decreasing the patient's perception that the bladder is full
- Cough suppression
- unless given a suppress coughing as part of a treatment regimen for an upper respiratory infection.
- Potential for abuse
- due to the euphoria that occurs secondary to stimulation of the MU receptors.
- Tolerance with continued use and cross tolerance with other opioids
- requiring larger doses to achieve the usual effect.
- Opioid agonists - Side/Adverse Effects
- Monitor vital signs and auscultate lungs for congestion
- Fro respiratory rates below 12 per minute, withhold the drug, stimulate breathing, and administer an opioid antagonist if indicated; Naloxone to restore respiratory rate.
- Monitor patients when ambulating to prevent injury
- Encourage fiber supplements, stool softeners
- Monitor intake and output, watching for signs of urinary retention (bladder distention)
- Encourage patients to urinate every 4 hours
- Prepare to insert a urinary catheter to drain the bladder.
- Opioid agonists - Interventions
- Measure baseline vital signs before administration and monitor throughout therapy.
- Administer orally, IM (intramuscularly), IV (Iintravenously), SC (subcutaneously), rectally, or epidurally
- Make sure patients swallow sustained-release forms whole and do not crush or chew them.
- Administer IV opioids by diluting as recommended and administering slowly over 4 to 5 minutes; have Naloxone and resusciation equipment available.
- Monitor PCA (patient-controlled analgesia) use and pump settings carefully.
- Administer to patients with cancer on a fixed, around-the-clock dosing schedule, not PRN.
- Opioid agonists - Administration
- Take the drug only when needed and short-term
- Do not take prior to driving or activities requiring mental alertness
- Sit or lie down if feeling lightheaded
- Change positions gradually
- due to the risk of dizziness and orthostatic hypotension, encourage patients to rise slowly from a reclining or sitting position to prevent falls.
- Increase fluid and fiber intake; activity and exercise
- Take the drug with food or milk (oral forms)
- Rose slowly from a reclining or sitting position
- Report any inability to urinate or difficulty irinating
- Cough regularly to clear secretions from the throat and chest to prevent pneumonia.
- Opioid agonists - Patient Instructions
- Pregnancy risk category D (long-term use, high doses, near term; otherwise C)
- Kidney failure
- Increased intracranial pressure
- Biliary colic, biliary tract surgery
- Preterm labor
- Opioid agonists - Contrindication
- II controlled substance
- Older adults, infants
- Reduced respiratory reserve
- Head injury
- Inflammatory bowel disease
- Prostatic enlargement
- Hypotension
- Hepatic or kidney disease
- Opioid agonists - Precautions
- CNS depressants (barbiturates, phenobarbital, benzodiazepines, alcohol) increase CNS depression.
- Anticholinergic agents, such as antihistamines, and tricyclic antidepressants increase interscholastic effects (constipation, urinary retention)
- MAOIs can cause hyperpyrexic coma (excitation, seizures, respiratory depression( with meperdine (Demerol)
- Antihypertensive increase hypotensive effects
- St. John's wort can increase sedation.
- Opioid agonists - Interactions
is an extreme elevation of body temperature which, depending upon the source, is classified as a core body temperature greater than or equal to 40.0 or 41.5 °C (104.0 or 106.7 °F).
Hyperpyrexia
- Analgesia for moderate to severe pain
- Anesthesia adjunct
II. Opioid agonist-antagonists
- Prototype drug:
- Butorphanol - only available as an injectable or nasal spray
- Pentazocine (Talwin) - available in oral form
- Other drugs:
- Buprenorphine (Buprenex) -
II. Opioid agonist-antagonists - Prototype/Other Drugs
- MU antagonists
- KAPPA agonists
- Fewer MU related side effects (respiratory depression, euphoria, dependence)
- Milder analgesic effects
- Can precipitate withdrawal in patients addicted to opioids
II. Opioid agonist-antagonists - Expected Pharmacologic Action
- Respiratory depression (limited)
- Sedation, dizziness, ligthheadedness, drowsiness
- Headache
- Nausea
- Increased cardiac workload (butorphanol and pentazocine)
- avoid using in patients who have a disorder that affects cardiac output.
- Abstinence syndrome
- may occur in patients who become depended on one of these drugs.
- withdrawal is less severe than that experienced by opioid-dependent patients
II. Opioid agonist-antagonists - Side/Adverse Effects
- Measure baseline vital signs
- Monitor respirations
- For respiratory rates below 12 per minute, withhold the drug and stimulate breathing
- Monitor patients when ambulating
- Consider recommending an alternative drug if nausea does not resolve
- Do not administer to patients with myocardial infarction or cardiac insufficiency
- Ask patients about opioid use before administration.
II. Opioid agonist-antagonists - Interventions
- Administer IM, IV, or intranasally
- Pentazoncine (Talwin)
- given orally
- often used when an invasive route is not warranted
- also often used when patients take the drug as part of home pain management.
- Measure baseline vital signs before administration and monitor throughout therapy.
- Do not give the drug if respirations are slower than 12 per minute
- Have Naloxone (Narcan) and resuscitation equipment available
- For intranasal administration on Butorphanol, give one spray and repeat every 60 to 90 minutes as needed
- For preoperative IM administration, give 60 to 90 minutes before surgery
- Monitor therapeutic effects
- Do not discontinue the drug abruptly if a patient is on it for an extended period of time.
II. Opioid agonist-antagonists - Administration
- Use the drug only when needed and short-term
- Do not take prior to driving or activities requiring mental alertness
- Sit or lie down if feeling lightheaded
- Change positions gradually
- Report worsening headache
- Lie down when feeling nauseated
- Do not use for anginal pain
- Do not take opioid while taking Butorphanol
II. Opioid agonist-antagonists - Patient Instructions
- Myocardial infarction
- Opioid dependence
patients should not take Nutorphanol or Pentazocine if they have either of the above contraindications.
II. Opioid agonist-antagonists - Contraindications
- Schedule IC controlled substance
- Hsstory of substance abuse
- Head injury, increased intracranial pressure
- Reduced respiratory reserve
- Hepatic or kidney disease
- Cardiac insufficiency
- Herpertension
II. Opioid agonist-antagonists - Precautions
- Don't give opioid agonist-antagonists with other CNS depressants as it can increase the risk of respiratory depression.
- barbiturates
- Phenobarbital
- Benzodiazepines
- Alcohol
- Opioid effects decrease
II. Opioid agonist-antagonists - Interactions
Various effects of Opioid that can be reversed or counteracted
- Reverse most effects:
- Respiratory depression
- Overdose
- Counteract selected effects:
- Constipation
- Euphoria
- Reversal or neonatal respiratory depression (from maternal analgesia)
Opioid Antagonists
- Prototype drug:
- Nalaxone - relieves opioid related constipation.
- Other drugs:
- Methylnaltrexone (Rlistor)
- Naltrexone (ReVia, Vivitrol) - prevents the euphoric effects of oipiods for patients addicted to opioid agonists
Opioid Antagonists - Prototype/Other Drugs
- Blocks opioid receptors
- effectively reversing or antagonizing the effects of opioids
Opioid Antagonists - Expected Pharmacologic Action
- Increase respiratory rate, blood pressure, heart rate
- Abstinence syndrome (hypertension, vomiting, tremors in opioid-dependent patients)
Opioid Antagonists - Side/Adverse Effects
- Monitor vital signs, in particular blood pressure
- Monitor heart rhythm for signs of ventricular tachycardia
- Have oxygen and resuscitation equipment ready
- Expects these symptoms in opioid- dependent patients
Opioid Antagonists - Side/Adverse Effects
- Administer IM, IC, SC
- Titrate doses carefully when giving the drug intravenously
- Monitor vital signs every 5 to 15 minutes
- Be aware that the drug might increase pain by reducing opioid effects and precipitate acute withdrawal for patients who are opioid-dependent
- Prepare to administer every 2 to 3 minutes until reversal of undesirable effects
- Prepare to begin administration again as the effects of opioids might persist beyond the effects of the reversal agent
- Observe for nausea, vomiting, tachycardia and diaphoresis (indications of opioid reversal)
Opioid Antagonists - Administration
- If awake, inform patient of need for drug
- Warn patient of possible side effects and return of pain
Opioid Antagonists - Patient Instructions
- Opioid dependence
- Respiratory depression due to nonopiod drugs
- patient should not take Naloxone
- Naloxone has no effect on drugs that are not opioids
Opioid Antagonists - Contraindications
- Cardiac irritability
- Head injury, increased intracranial pressure
- Brain tumor
- Seizure disorders
Opioid Antagonists - Precautions
- Opioid effects decrease
Opioid Antagonists - Interactions
- Uricosurics
- Glucocortocoids
Two Categories of Drugs that support the treatment of inflammation
- Treats the hyperuricemia that causes gout.
- Treats the hyperuricemia occurs secondary to cancer chemotherapy and blood dyscrasias
Uricosurics
- is an inflammatory disorder that occurs secondary to high levels of uric acid in the blood
- Urate acid crystals develop secondary to the hyperuricemia, and are deposited in joints,
- The joints primarily affected are the small joints in the body, the ones in the big toe in particular
- IF left untreated over a period of years, the urate crystals also deposit in the skin and various organs in the body.
Gout
- is an excess of uric acid in the blood. Uric acid passes through the liver, and enters your bloodstream. Most of it is excreted (removed from your body) in your urine, or passes through your intestines to regulate "normal" levels. (Chemocare.com)
Hyperuricemia
- Prototype drug:
- Allopurinol (Zyloprim)
- Other Drugs:
- Febuxostat (Uloric)
- Probenecid
Colchicine used to treat hyperuricemia for many years, but newer drugs with fewer side effects eventually replaced the use of this drug.
Opioid Antagonists - Prototype/Other Drugs
- Allopurinol , Febuxostat
- Xanthin Oxidase (XO) inhibited (from converting hypocanthine and xanthine into uric acid)
- Block formation of uric acid
- Probenecid
- Inhibits tubular reabsorption of uric acid in the kidney
- Promotes excretion of uric acid
Opioid Antagonists - Expected Pharmacologic Action
- Hypersensitivity syndrome
- fever, rash, eosinophilia (increase in the eosinophils, a white blood cell) , liver and kidney dysfunction
- Gastrointestinal disturbance
- nausea, vomiting, diarrhea
- Drowsiness, headache, vertigo (CNS effects)
- Agranulocytosis (decrease in certain type of white blood cells), aplastic anemia (decrease in several types of blood cells), bone marrow depression
- Metallic state in the mouth
- Cataracts
- with drug therapy longer than 3 yrs
Opioid Antagonists - Side/Adverse Effects
- Monitor for symptoms of hypersensitivity syndrome
- patients who just starting to take Uricosuric
- patients who've been taking one for 2 to 4 weeks
- IF fever or rash develops, stop the drug immediately, check liver and kidney function test, and notify the provider.
- Stop drug therapy immediately for signs of hypersensitivity syndrome
- Monitor for worsening GI effects
- For vomiting, ensure adequate hydration
- give the drug after meal
- Give drug after meals
- Monitor patients for drowsiness or vertigo when ambulating
- Monitor CBC, liver, kidney function tests and uric acid level
- Monitor for unusual taste sensations
- Recommend regular ophthalmologic examinations
Opioid Antagonists - Interventions
- Give Allopurinol orally or IV
- Monitor uric acid level
- initially every 1 to 2 weeks to establish the appropriate dosage
- Obtain baseline CBC, liver, and kidney function tests before therapy and monitor periodically thereafter
- Allow crushing tablets and mixing them with food or fluid
- Administer IV using recommended dilution and infuse over 30 to 60 minutes
- Make sure patients drink at least 3 L/day of fluid
Opioid Antagonists - Administration
- Report fever, rash, abdominal pain, swelling, or low urine output immediately
- Drink 3 L/day of fluids
- Report bleeding, easy bruising, or sore throat
- in relation to the potential for bone marrow suppression
- Warn patients that they may develop a metallic taste in their mouth
- Report blurred vision and/or loss of color acuity
- teach patients the early signs of cataract development
- Minimize exposure of eyes to sunlight
- wear sunglasses with ultraviolet (UV) protection
- Obtain periodic eye examinations
- Let them know that they can take the drug with food or right after a meal if it causes nausea
Opioid Antagonists - Patient Instructions
- Hypersensitivity to Allopurinol
Opioid Antagonists - Contraindications
- Bone marrow depression
- Liver or kidney dysfunction
- Peptic ulcer disease
- Lower gastrointestinal tract disease
Opioid Antagonists - Precautions
- Warfarin (Coumadin) requires lower dosage and closely monitor clotting time.
- due to Allopurinol increases the anticoagulant effect of Warfarin
- Concurrent administration of Allopurinol with the following, increases their potential for toxicity
- mercaptopurine (Purinethol)
- Theorphylline (Theolair)
- Azathioprine (Imuran)
- Ampicillin (Principen) increases the risk for rash when used with Allopurinol
Opioid Antagonists - Interactions
- Symptomatic relief of pain and inflammation for a wide variety of disorders
- Inflammatory disorders
- Autoimmune disorders
- Management of many skin disorders; allergic reactions
- Delay of progression of some disorders, such as rheumatoid arthritis
- Prevention of organ rejection
- Adjunctive therapy for some cancer
Glucocorticoids
- Prototype drug:
- Prednisone (Deltasone)
- Other drugs:
- Hydrocortisone Sodium Succinate (Solu-Cortef)
- Methylprednisolone (Solu-Medrol)
Glucocorticoids - Prototype/Other Drugs
- Corticosteroids: Hormonal Steroids
- Glucocorticoid: cortisol
- Mineralcoticoids: Aldosterone
- Suppresses inflammation and immune response
- Glucocorticoids mimic cortisol by suppressing inflammation and the immune response. They do this by inhibiting the synthesis of prostaglandins.
- Inhibits synthesis of prostaglandins (decreases pain)
- Decreased permeability of capillaries (decrease swelling)
- Inhibits lysosomal activity (decreases inflammation)
- Decreases production of lymphocytes (decreases immune response)
NSAIDs were considered "non-steroidal" anti-inflammatory drugs because corticosteroids are the "steroidal" anti-inflammatory drugs to which the "non" in the NSAIDs acronym refers.
Glucocorticoids - Expected Pharmacologic Action
are hormonal steroids produced by the adrenal cortex, the outside covering of the adrenal glands that sit on top of the kidneys
Corticosteroids
- a hormone that help regulate carbohydrate, fat, and protein metabolism.
- produced in response to stress, in an effort to restore emotional stability.
- the most important effect of cortisol, which forms the basis for its use as a pharmaco-therapeutic agent, is its ability to produce anti-inflammatory effects in the body as well as suppress the immune system.
Cortisol (glucocorticoinds)
- promote the retention of sodium by the kidneys and secondarily, fluid and electrolyte levels in the body.
Aldosterone (mineralocorticoids)
- Suppression of adrenal function
- because the adrenal gland no longer has produce its own cortisol.
- Hyperglycemia
- due to effect on carbohydrate metabolism
- Myopathy (weakness of the muscles)
- due to the effect on protein metabolism
- Peptic ulcer disease, gastrointestinal discomfort
- due to glucocorticoids' ability to inhibit prostaglandin synthesis
- Infection
- due to suppressed immune system
- Fluid and electrolyte imbalances
- due to mineralocorticoid effects
- Fat redistribution (long-term therapy)
- due to the effect on fat metabolism.
- increasing fat deposition in the face, torso, and upper back, and decreasing fat in the extremities. This combination results in truncal obesity with a moon face and buffalo hump.
- Bone loss
- due to glucocorticoids ability to draw calcium out of the bones
- can cause osteoporosis
- Cataracts (long-term therapy)
Glucocorticoids - Side/Adverse Effects
- Patients experiencing physical or emotional stress, monitor them for signs of adrenal insufficiency such as hypotension and fatigue.
- Larger dosage during times of illness and stress
- Monitor blood glucose levels, especially for patients who have diabetes mellitus
- Adjust dosages of insulin/hypoglycemic drugs accordingly
- Observe for gastrointestinal bleeding
- bloody vomitus, black or tarry stools.
- Implement gastric protective measures
- Give drug with food or meals
- Recommend analgesic substitute if NSAID is prescribed
- Observe for signs of infection that may not include fever or inflammation
- sore throat, fatigue, tachycardia, and discharge from a wound.
- Recommended initiation of appropriate antimicrobial therapy
- Monitor intake and output; water for edema, crackles in the lungs, and unexplained weight gain. (hypernatremia).
- Monitor also for generalized weakness (hypokalemia) and Cushing-like effects: abdominal fat, buffalo hump, moon face.
- Recommend the lowest possible effective dose and alternate-date dosing.
- Regular ophthalmologic examinations
Glucocorticoids - Interventions
- Give orally, IV, IM, SC, topically, intranasally, or by inhalation, depending on the indication
- For short-term oral use the largest dose is given on the 1st day with progressive smaller doses for each of the next 8 days
- For long-term use (10 days +), take in the morning using alternate-day dosing
- Taper the dose slowly when symptoms are controlled to establish the lowest possible oral dose
- Give supplemental doses as needed in times of stress
Glucocorticoids - Administration
- Make sure that patient understand the effects that these drugs have on the body, and the implications of adrenal suppression.
- For short-term dosing, follow the instructions carefully for each day's dose
- For long-term dosing, take drug on alternate days
- Report increased stress, contact provider because higher dosages may be required at such times
- Taper the dose before discontinuing it
- Report polyphagia, polydipsia , and polyuria; muscle pain or weakness
- Avoid taking NSAIDs; take with food or meals
- Report indigestion, bloody vomitus, black, tarry stools
- Report signs of infection, weight gain or edema (hypernatremia). Also report weakness (hypokalemia)
- Understand that long-term therapy may cause some changes in fat distribution throughout the body
- Perform weight-bearing exercise daily; consume adequate calcium and vitamin D
- Report blurred vision and loss of color acuity (cataract)
- Minimize exposure of eyes to sunlight
- Obtain periodic eye examinations.
Glucocorticoids - Patient Instructions
- Systemic fungal infection
- Cataracts
Glucocorticoids - Contraindications
- Heart failure
- Peptic ulcer ulcer disease
- Diabetes mellitus
- Peptic ulcer disease
- Hypertension
- Kidney dysfunction
- Myasthenia gravis
- Osteoporosis
Glucocorticoids - Precautions
- Glucocorticoids prevent the body from responding to vaccines
- Live vaccine administration increases risk for developing that viral disease
- Potassium-depleting diuretics, such as Furosemide (Lasix) increase risk of hypokalemia
- Risk of digoxin-induced dysrhythmias increases with digoxin
- NSAIDs increase risk of gastrointestinal bleeding and ulceration
- Effects of insulin and oral hypoglycemics decrease in patients who have diabetes
Glucocorticoids - Interactions
Analgesics
- Nonopioid analgesics
- NSAIDs (COX-1 and COX-2 inhibitors)
- NSAIDs (COX-2 inhibitors)
- Acetaminophen
- Centrally acting analgesics
- Opioid analgesics
- Opioid aganists
- Opioid agonist-antagonists
- Opioid antagonist (reverse the effects of opioid agonist & opioid agonist-antagonist)
Anti-inflammatories
- Uricosurics (given to patients with gout)
- Glucocorticoids (given to patients with inflammatory or autoimmune disorder)
Summary: Pain and Inflammation Medication
D. Petechiae
Aspirin inhibits platelet aggregation and can cause bleeding. Instruct the patient to watch for and report any signs of bleeding, such as bruising, petechiae, and coffee-ground emesis. Monitor coagulation studies as well. Aspirin helps prevent blood clots. A swollen, reddened, painful calf and shortness of breath are unlikely. Aspirin is more likely to nausea, vomiting, and diarrhea than constipation.
Drill 1:
A patient is about to start taking aspirin to prevent cardiovascular events. You should instruct the patient to watch for and report which of the following adverse effects of aspirin?
- Dyspnea
- Constipation
- Calf pain
- Petechiae
Ibuprofren (Advil) - B Nonsteroidal anti-inflammatory drug
Morphine - D - Opioid analgesic
Prednisone - A - Glucocorticoid
Naloxone - C - Opioid antagonist
Drill 2:
Match the drug in the left column with its classification in the right column by typing the appropriate letter in the center column.
- Glucocorticoid
- Nonsteroidal anti-inflammatory drug
- Opioid antagonist
- Opioid analgesic
- Ibuprofren (Advil)
- Morphine
- Prednisone
- Naloxone
- Take it with food
- Rise slowly from sitting or reclining
- Take it on a fixed schedule
- Increase fluid and fiber intake
- Do not take it before driving
Drill 3:
A patient is about to start taking oral morphine to treat acute pain from an injury. Which of the following instructions should you include when talking with the patient about taking morphine? (Select all that apply)
- Take it with food
- Rise slowly from sitting or reclining
- Take it on a fixed schedule
- Increase fluid and fiber intake
- Do not take it before driving
D. Increase serum glucose monitoring
Because prednisone can cause hyperglycemia, the primary provider should monitor the patient's serum glucose levels more frequently. The patient might need a higher insulin dose and might have to reduce his carbohydrate intake. The patient should watch for signs of hyperglycemia, such as polyuria, polyphagia, and polydipsia. Reducing the prednisone does may not reduce the risk for hyperglycemia.
Drill 4:
A provider prescribes prednisone for a patient who has type 1 diabetes mellitus. Recognizing the risk for an adverse reaction to the prednisone, which of the following precautions should the provider take for this patient?
- Reduce the insulin dose
- Increase carbohydrate intake
- Reduce the prednisone dose
- Increase serum glucose monitoring
A. Allow 1 hr for it to take effect
Drill 5:
A patient is about to start Tramadol (Ultram) to treat moderate pain. Which of the following instructions should you include when talking with the patients about taking this drug?
- Allow 1 hr for it to take effect
- Take it on an empty stomach
- Check the extended-release tablets
- Do not take it with grapefruit juice.
B. Hyperuricemia
Drill 6:
A patient who is receiving chemotherapy take Allopurinol (Zyloprim) prior to the chemotherapy to reduce the risk for which of the following?
- Agranulocytosis
- Hyperuricemia
- Aplastic anemia
- Thrombocytopenia
Butorphanol - C - Anesthesia adjunct
Acetaminophen (Tylenol) - D - Fever reduction
Prednisone - B - Prevention of organ rejection
Morphine - A - Sedation
Drill 7:
Match the drug in the left column with its classification in the right column by typing the appropriate letter in the center column.
- Sedation
- Prevention of organ rejection
- Anesthesia adjunct
- Fever reduction
- Butorphanol
- Acetaminophen (Tylenol)
- Prednisone
- Morphine
C. Acetylcysteine (Acetadote)
Drill 8:
A patient arrives at the emergency room immediately following an acetaminophen (Tylenol) overdose. Which of the following drugs should you prepare to administer?
- Atropine
- Naloxone
- Acetylcysteine (Acetadote)
- Flumazenil
B. use a Fentanyl (Submilaze) patch for chronic pain
Drill 9:
Butorphamol is an unsafe analgesic choice for patients who
- take glucocorticoids for rheumatoid arthritis
- use a Fentanyl (Submilaze) patch for chronic pain
- have type 1 diabetes mellitus and use an insulin pump
- take Warfarin (Coumadin) for thrombophlebitis.
A. Black, tarry stools
Drill 10:
A patient is about to begin Celecoxib (Celebrex) theraphy for osteoarthritis. You should instruct the patient to watch and report which of the following possible indications of a serious reaction to this drug?
- Black, tarry stools
- Polyuria
- Bone pain
- Dry mouth
C) Morphine
Naloxone, an opioid antagonist, reverses the effects of morphine, an opioid analgesic. Health care professionals should monitor respirations and reassess patients after the effects of naloxone have diminished (20 to 40 min) for recurrence of the adverse effects of morphine
A health care professional should understand that naloxone can reverse the effects of an excessive dosage of which of the following drugs?
A) Aspirin
B) Acetaminophen (Tylenol)
C)
Morphine
D) Prednisone
D) Hypokalemia
Prednisone, a glucocorticoid, can cause hypokalemia. The risk for this electrolyte imbalance increases with potassium-depleting diuretics, such as furosemide. Health care professionals should monitor potassium levels of patients who are taking both drugs or recommend the primary care provider prescribe a safer combination.
A health care professional is caring for a patient who takes furosemide (Lasix)
and is about to begin taking prednisone to treat
inflammatory bowel disease. The health care professional should
monitor the patient for which of the following results of concurrent
use of the two drugs?
A) Hypercalcemia
B)
Hypoglycemia
C) Hypothermia
D) Hypokalemia
A) Chest pain
Celecoxib, a COX-2 inhibitor, can cause cardiovascular or cerebrovascular events. Patients should report chest pain, shortness of breath, headache, numbness, weakness, or confusion. Primary care providers should prescribe the lowest effective dosage for the shortest time period possible.
A health care professional is caring for a patient who is about to begin taking celecoxib (Celebrex) to treat rheumatoid arthritis. The health care professional should tell the patient to report which of the following adverse reactions?
A) Chest pain
B) Tinnitus
C) Constipation
D) Diaphoresis
B) "Ibuprofen will reduce the antiplatelet effects of low-dose aspirin."
Ibuprofen, an NSAID, reduces the antiplatelet effects of low-dose aspirin. Patients taking low-dose aspirin for its antiplatelet effects should not take ibuprofen.
A patient who takes low-dose aspirin to prevent cardiovascular events asks a health care professional about taking ibuprofen (Advil) to treat rheumatoid arthritis. The health care professional should respond with which of the following statements?
A) "Ibuprofen will increase the risk for
salicylism."
B) "Ibuprofen will reduce the
antiplatelet effects of low-dose aspirin."
C)
"Low-dose aspirin will reduce the anti-inflammatory effects of
ibuprofen."
D) "Low-dose aspirin will reduce the
analgesic effects of ibuprofen."
B) Sore throat
C) Vertigo
D) Bruising
E) Vision changes
- Sore throat is correct. Allopurinol, an antigout drug, can cause agranulocytosis. Health care professionals should monitor WBC counts, and tell patients to report fever or sore throat and avoid crowds or exposure to people who might have communicable diseases.
- Vertigo is correct. Allopurinol, an antigout drug, can cause drowsiness and vertigo. Patients should avoid activities that require mental alertness until they know how the drug will affect them. They should also report vertigo.
- Bruising is correct. Allopurinol, an antigout drug, can cause thrombocytopenia. Health care professionals should monitor platelets and have patients report any bleeding or bruising.
- Vision changes is correct. Allopurinol, an antigout drug, can cause cataracts with extended use. Patients should report vision changes, such as cloudiness or halos around lights, and have eye examinations at recommended intervals.
A health care professional is caring for a patient who is about to begin taking allopurinol (Zyloprim) to prevent hyperuricemia. The health care professional should advise the patient to report which of the following adverse effects? (Select all that apply.)
A) Palpitations
B) Sore throat
C) Vertigo
D)
Bruising
E) Vision changes
B) Vomiting
D) Abdominal
cramps
E) Hypertension
- Vomiting is correct. Abstinence syndrome can cause nausea, vomiting, and anorexia.
- Abdominal cramps is correct. Abstinence syndrome can cause abdominal cramps and anorexia.
- Hypertension is correct. Abstinence syndrome can cause hypertension, tremors, and fever.
A health care professional is caring for a patient who is opioid-dependent and is about to begin taking butorphanol (Stadol). The health care professional should recognize the patient is at risk for developing a syndrome that causes which of the following? (Select all that apply.)
A) Bronchospasm
B) Vomiting
C) Peripheral edema
D) Abdominal cramps
E) Hypertension
C) Bone loss
Prednisone, a glucocorticoid, can cause osteoporosis, especially with long-term use. Patients taking the drug should increase weight-bearing activity and report back pain. Health care professionals should monitor bone density.
A health care professional is caring for an older adult patient who is about to begin taking prednisone for long-term treatment of rheumatoid arthritis. The health care professional should monitor the patient for which of the following adverse effects?
A) Pulmonary embolism
B) Hepatitis
C) Bone loss
D) Breast cancer
A) Tachypnea
B) Increased
pain
D) Tachycardia
E)
Hypertension
- Tachypnea is correct. Naloxone treats respiratory depression, but it can cause hyperventilation. It is essential for the health care professional to monitor respiration and oxygenation for patients receiving the drug.
-
Increased pain is correct. Naloxone reverses
the analgesic effects of opioids and can cause increased pain and
discomfort. It is essential for the health care professional to
assess pain frequently for patients receiving the drug.
- Tachycardia is correct. Naloxone can increase heart rate. It is essential for the health care professional to monitor patients receiving the drug for tachycardia and ventricular dysrhythmias.
- Hypertension is correct. Naloxone can cause hypertension. It is essential for the health care professional to monitor blood pressure for patients receiving the drug.
A health care professional is caring for a patient who is taking naloxone to treat a morphine overdose. The health care professional should monitor for which of the following adverse effects? (Select all that apply.)
A) Tachypnea
B) Increased pain
C)
Thrombophlebitis
D) Tachycardia
E) Hypertension
A) Diaphoresis
D) Nausea
E) Diarrhea
- Diaphoresis is correct. Acetaminophen toxicity can cause diaphoresis, anorexia, and, eventually, liver damage. Patients should following the dosage guidelines on the labels of over-the-counter drugs carefully to avoid overdose.
- Nausea is correct. Acetaminophen toxicity can cause nausea, vomiting, and anorexia and can lead to liver damage.
- Diarrhea is correct. Acetaminophen toxicity can cause diarrhea, lethargy, and, eventually, liver damage.
A patient recovering from a total knee arthroplasty has been prescribed acetaminophen (Tylenol) for mild discomfort that does not require an opioid. The health care professional should tell the patient to report which of the following early indications of acetaminophen overdose? (Select all that apply.)
A) Diaphoresis
B) Palpitations
C) Shortness of
breath
D) Nausea
E) Diarrhea
C) Weight gain
Aspirin use can cause renal dysfunction, especially in older adults and patients who have pre-existing renal or liver dysfunction and heart failure. Patients should report reduced urine output, weight gain, edema, or bloating. Health care professionals should monitor BUN and creatinine values, and stop aspirin therapy for patients who develop signs of renal dysfunction.
A health care professional is caring for an older adult patient who is about to begin taking aspirin to treat an ankle sprain. The health care professional should tell the patient to report which of the following adverse reactions?
A) Polyuria
B) Bone pain
C) Weight gain
D) Infection
A) Fever
Allopurinol, an antigout drug, can cause hypersensitivity syndrome. Patients should report rash, itching, or fever, as hypersensitivity reactions can lead to renal or liver dysfunction. Patients who develop this type of reaction should stop taking the drug.
A health care professional is caring for a patient who is about to begin taking allopurinol (Zyloprim) to treat gout. The health care professional should monitor the patient for hypersensitivity syndrome, which causes which of the following clinical manifestations?
A) Fever
B) Muscle pain
C) Anxiety
D) Tremors
B) Nausea
D) Dizziness
E) Headache
Nausea is correct. Butorphanol, an opioid agonist-antagonist, can cause nausea. Patients taking the drug should lie down when feeling nauseated.
Dizziness is correct. Butorphanol, an opioid agonist-antagonist, can cause dizziness and drowsiness. Patients taking the drug should avoid activities that require alertness.
Headache is correct. Butorphanol, an opioid agonist-antagonist, can cause headaches and increased intracranial pressure. Patients taking the drug should report severe headaches.
A health care professional is caring for a patient who is about to begin taking butorphanol for pain control. The health care professional should monitor the patient for which of the following adverse effects? (Select all that apply.)
A) Infection
B) Nausea
C) Tachycardia
D)
Dizziness
E) Headache
B) Discontinue the drug gradually.
C)
Report illness or infection.
D)
Increase intake of calcium and vitamin D.
E) Monitor for signs of gastric bleeding
- Discontinue the drug gradually the drug gradually is correct. Prednisone, a glucocorticoid, suppresses adrenal function. Patients taking the drug should taper the dosage before discontinuing it to allow for resumption of adrenal activity.
- Report illness or infection is correct. Patients can need higher doses of prednisone during illness or infection. Health care professionals should tell patients taking the drug to report signs of infection.
- Increase intake of calcium and vitamin D is correct. Prednisone, a glucocorticoid, can cause bone loss and reduced calcium absorption. Patients should increase their intake of calcium and vitamin D.
- Monitor for signs of gastric bleeding Prednisone, a glucocorticoid, can cause peptic ulcer disease. Patients should report signs of gastric bleeding, such as hematemesis or black tarry stools.
A health care professional is caring for a patient who is about to begin taking prednisone to treat systemic lupus erythematosus. When talking with the patient about the drug, the health care professional should include which of the following instructions? (Select all that apply.)
A) Reduce the dose during periods of stress.
B) Discontinue
the drug gradually.
C) Report illness or infection.
D)
Increase intake of calcium and vitamin D.
E) Monitor for signs
of gastric bleeding
D) Cholecystectomy
Morphine can cause biliary colic. It is inappropriate for patients who have just had biliary tract surgery, such as a cholecystectomy.
A health care professional should question the use of morphine for a patient who is recovering from which of the following procedures?
A) Mastectomy
B) Knee arthroplasty
C) Cystoscopy
D) Cholecystectomy
A) To reduce fever
C) To relieve
mild pain
- To reduce fever is correct. Acetaminophen reduces fever. It is important, however, to monitor patients taking the drug for signs of hepatotoxicity.
- To relieve mild pain is correct. Acetaminophen relieves mild to moderate pain. It is important, however, to monitor patients who might take high doses for early signs of toxicity, including sweating, nausea, diarrhea, and abdominal discomfort.
A health care professional should advise patients to take acetaminophen (Tylenol) for which of the following? (Select all that apply.)
A) To reduce fever
B) To decrease inflammation
C) To
relieve mild pain
D) To promote sedation
E) To alleviate anxiety
B) Peptic ulcer disease
Ibuprofen, an NSAID, is inappropriate for patients who have peptic ulcer disease. Health care professionals should monitor patients who are taking over-the-counter analgesics for gastric bleeding, and test or treat patients who have Helicobacter pylori prior to long-term or repeated treatment with these drugs.
A health care professional should advise a patient who has which of the following to stop taking ibuprofen (Advil) to treat an occasional headache or muscle strain?
A) Penicillin allergy
B) Peptic ulcer disease
C)
Dysmenorrhea
D) Hyperthyroidism
D) Alcohol use disorder
Acetaminophen can cause liver toxicity. Patients who have a history of alcohol use disorder should not take the drug.
A health care professional should question the use of acetaminophen (Tylenol) for patients who have which of the following?
A) Asthma
B) Diabetes mellitus
C) Heart failure
D) Alcohol use disorder
A) Phenobarbital (Luminal) for a seizure disorder
Taking morphine and phenobarbital together can cause increased CNS depression. Lower morphine doses are essential for patients who are taking phenobarbital. Health care professionals should monitor patients who are taking both drugs for decreased respirations and blood pressure and increased sedation.
A health care professional should question the use of morphine for a patient who is taking which of the following drugs?
A) Phenobarbital (Luminal) for a seizure disorder
B)
Warfarin (Coumadin) for anticoagulation
C) Glipizide
(Glucotrol) for diabetes mellitus
D) Alendronate (Fosamax) for osteoporosis
A) Seizure disorder
Tramadol, a nonopioid analgesic, can cause seizure activity. Patients who have seizure disorders, head injuries, or increased intracranial pressure should not take the drug.
A health care professional should question the use of tramadol (Ultram) for patients who have which of the following?
A) Seizure disorder
B) Hyperthyroidism
C) Rheumatoid
arthritis
D) Urinary incontinence
A) Fever
B) Tinnitus
C) Diaphoresis
E) Dizziness
- Fever is correct. Late symptoms seen in acute poisoning include fever. Prednisone, a glucocorticoid, is a drug that suppresses the immune response and increases patients' susceptibility to infection and fever.
- Tinnitus is correct. Ringing or buzzing in the ears can indicate salicylism. Patients should report this reaction, and stop taking aspirin at least until tinnitus resolves.
- Diaphoresis is correct. Sweating and headache can indicate salicylism. Patients should report these effects, and stop taking aspirin at least until the effects resolve.
- Dizziness is correct. Dizziness can indicate salicylism. Patients should report this effect, and stop taking aspirin at least until it resolves.
A health care professional is caring for a patient who has osteoarthritis and is about to begin taking aspirin. The health care professional should tell the patient to report which of the following possible indications of salicylism? (Select all that apply.)
A) Fever
B) Tinnitus
C) Diaphoresis
D)
Thrombophlebitis
E) Dizziness
B) Withhold the drug for respiratory rates below 12/min.
Butorphanol, an opioid agonist-antagonist, can cause respiratory depression. It is essential to monitor respiratory rate prior to administration and withhold the drug for rates below 12/min.
A health care professional is preparing for administer butorphanol (Stadol) to a patient for pain control. During administration, the health care professional should take which of the following actions?
A) Caution the patient about the drug's potential for abuse.
B) Withhold the drug for respiratory rates below 12/min.
C)
Administer one nasal spray into each nostril.
D) Give the drug
with an opioid agonist for maximal effects.
C) An allergy to sulfonamides
Patients who are allergic to sulfonamides can have severe allergic reactions to celecoxib, a COX-2 inhibitor. Patients who are allergic to salicylates can also react adversely to the drug
A health care professional should question the use of celecoxib (Celebrex) for a patient who has which of the following?
A) Rheumatoid arthritis
B) Ankylosing spondylitis
C)
An allergy to sulfonamides
D) Adrenocortical insufficiency
A) Increase fiber and fluid intake.
B)
Take the drug with food.
C) Avoid
driving after taking the drug.
D) Change
positions gradually.
- Increase fiber and fluid intake is correct. Tramadol can cause constipation and dry mouth. Patients taking the drug should increase fluid and fiber intake to minimize constipation, and sip water, suck on hard candy, or chew gum to relieve dry mouth.
- Take the drug with food is correct. Tramadol can cause nausea and vomiting. Patients should take the drug with food or milk and lie down if feeling nauseated.
- Avoid driving after taking the drug is correct. Tramadol can cause sedation and drowsiness. Patients taking the drug should avoid driving or other activities that require alertness.
- Change positions gradually is correct. Tramadol can cause sedation and dizziness. Patients taking the drug should use caution when changing positions and ambulating.
A health care professional is caring for a patient who is about to begin taking tramadol (Ultram) to treat moderate acute pain from a shoulder injury. When talking with the patient about the drug, the health care professional should include which of the following instructions? (Select all that apply.)
A) Increase fiber and fluid intake.
B) Take the drug with
food.
C) Avoid driving after taking the drug.
D) Change
positions gradually.
E) Reduce exercise level temporarily.
B) Urinary retention
C) Respiratory
depression
D) Sedation
E)
Orthostatic hypotension
- Urinary retention is correct. Morphine can cause urinary retention. Health care professionals should monitor fluid intake and output and assess for bladder distention.
- Respiratory depression is correct. Morphine can cause severe respiratory depression. Health care professionals should withhold the drug for respiratory rates below 12/min.
- Sedation is correct. Morphine can cause sedation, dizziness, and lightheadedness. Patients taking the drug should avoid activities that require alertness.
- Orthostatic hypotension is correct. Morphine can cause hypotension and postural hypotension. Patients taking the drug should change positions gradually.
A health care professional is caring for a patient who is receiving morphine to relieve severe pain. The health care professional should monitor the patient for which of the following adverse effects? (Select all that apply.)
A) Diarrhea
B) Urinary retention
C) Respiratory
depression
D) Sedation
E) Orthostatic hypotension
D) Aspirin
NSAIDs, especially aspirin, can increase the risk for Reye’s syndrome in children who have a viral infection, particularly chickenpox or influenza. Manifestations of Reye's syndrome include lethargy and persistent vomiting.
Which of the following drugs can increase the risk of Reye's syndrome in children who have viral infections?
A) Butorphanol (Stadol)
B) Acetaminophen (Tylenol)
C)
Tramadol (Ultram)
D) Aspirin
B. Identify and avoid trigger factors.
C. Lie down in a dark quiet room at the onset of a migraine.
D. Avoid foods that contain tyramine.
A nurse is providing teaching to a client who is experiencing
migraine
headaches. Which of the following instructions should
the nurse provide? (Select all that apply.)
A. Take ergotamine as a prophylaxis to prevent a migraine
headache.
B. Identify and avoid trigger factors.
C. Lie down
in a dark quiet room at the onset of a migraine.
D. Avoid foods
that contain tyramine.
E. Avoid exercise that can increase heart rate.
A. Keep the client NPO until pharyngeal response returns.
A nurse is planning care for a client who is to receive tetracaine
prior
to a bronchoscopy. Which of the following actions should
the nurse
include in the plan of care?
A. Keep the client NPO until pharyngeal response returns.
B.
Monitor the insertion site for a hematoma.
C. Palpate the bladder
to detect urinary retention.
D. Maintain the client on bed rest
for 12 hr fol
A. Seizures
A nurse is caring for a client who receives a local anesthetic
of
lidocaine during the repair of a skin laceration. For which of
the following adverse reactions should the nurse monitor the client?
A. Seizures
B. Tachycardia
C. Hypertension
D. Fever
D. An ECG indicates a first‑degree heart block.
A nurse is reviewing the health history of a client who has migraine
headaches and is to begin prophylaxis therapy with propranolol. Which of
the following
findings in the client history should the nurse
report to the provider?
A. The client had a prior myocardial infarction.
B. The client
takes warfarin for atrial fibrillation.
C. The client takes an
SSRI for depression.
D. An ECG indicates a first‑degree heart block.
C. Positive home pregnancy test
D. Numbness and tingling in fingers
E. Muscle pain
A nurse is providing teaching to a client who has
migraine
headaches and a new prescription for ergotamine. For which
of the
following adverse effects should the nurse instruct the
client to stop
taking the medication and notify the provider?
(Select all that apply.)
A. Nausea
B. Visual disturbances
C. Positive home
pregnancy test
D. Numbness and tingling in fingers
E. Muscle pain
A. Dizziness
D. Tinnitus
E. Headache
A nurse is assessing a client who has salicylism. Which of the following findings should the nurse expect? (Select all that apply.)
A. Dizziness
B. Diarrhea
C. Jaundice
D.
Tinnitus
E. Headache
A. Acetylcysteine
A nurse is admitting a toddler to the hospital after an acetaminophen overdose. Which of the following medications should the nurse anticipate administering to this client?
A. Acetylcysteine
B. Pegfilgrastim
C. Misoprostol
D. Naltrexone
A. Increases the risk for a myocardial infarction
A nurse is teaching a client about the a new prescription
for
celecoxib.
Which of the following information should the nurse include in the teaching?
A. Increases the risk for a myocardial infarction
B. Decreases
the risk of stroke
C. Inhibits COX‑1
D. Increases platelet aggregation
C. Warfarin
A nurse is taking a history for a client who reports that he is
taking
aspirin about four times daily for a sprained wrist. Which
of the following
prescribed medications taken by the client is
contraindicated with aspirin?
A. Digoxin
B. Metformin
C. Warfarin
D. Nitroglycerin
D. Respiratory depression
A nurse in an emergency department is performing an admission
assessment for a client who has severe aspirin toxicity. Which of the
following findings
should the nurse expect?
A. Body temperature 35° C (95° F)
B. Lung crackles
C.
Cool, dry skin
D. Respiratory depression