



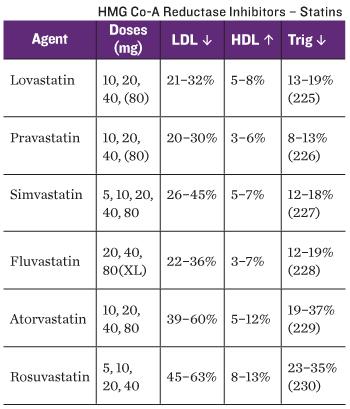
HMG-CoA REDUCTASE INHIBITORS
atorvastatin
(Lipitor)
fluvastatin (Lescol)
lovastatin (Mevacor)
pitavastatin
(Livalo)
pravastatin (Pravachol)
rosuvastatin
(Crestor)
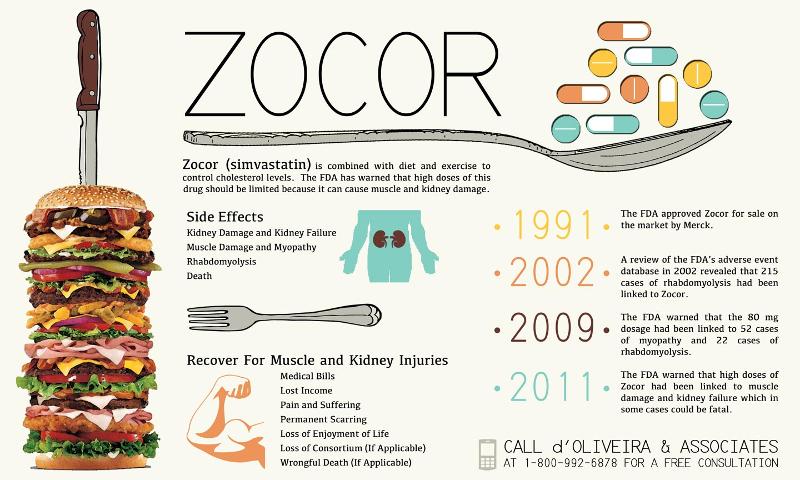
simvastatin (Zocor)
PO; 10–80 mg daily (max: 80 mg/day)
PO; 20 mg daily (max: 80 mg/day)
Headache, dyspepsia, abdominal cramping, myalgia, rash or pruritus
lovastatin (Mevacor)
PO; 10–20 mg
once daily (max: 80 mg/day immediate release; 60 mg/day extended
release)
Rhabdomyolysis, severe myositis, elevated hepatic enzymes
pitavastatin (Livalo)
pravastatin
(Pravachol)
rosuvastatin (Crestor)
simvastatin
(Zocor)
PO; 1–4 mg daily (max: 4 mg/day)
PO; 10–40 mg daily
(max: 80 mg/day)
PO; 5–40 mg daily (max: 80 mg/day)
PO;
5–40 mg daily (max: 80 mg/day)
BILE ACID SEQUESTRANTS
cholestyramine
(Questran)
colesevelam (Welchol)
colestipol (Colestid)
PO; 4–8 g bid–qid (max: 32 g/day)
PO; 1.9 g bid (max: 4.4
g/day)
PO; 5–20 g daily in divided doses
Constipation,
nausea, vomiting, abdominal pain, bloating, dyspepsia
Gastrointestinal (GI) tract obstruction, vitamin deficiencies
due to poor absorption
FIBRIC ACID AGENTS
fenofibrate (Antara, Tricor,
others)
fenofibric acid (Fibricor, Lofibra, Trilipix)
PO; 54
mg daily (max: 200 mg/day)
PO; (Fibricor: regular release):
35–105 mg once daily
PO; (Triplex: delayed release): 45–135 mg
once daily
Myalgia, flulike syndrome, nausea, vomiting, increased
serum transaminase and creatinine levels
Rhabdomyolysis,
cholelithiasis, pancreatitis
gemfibrozil (Lopid)
PO; 600 mg
bid (max: 1,500 mg/day)
PO; 54 mg daily (max: 200 mg/day)
PO; (Fibricor: regular
release): 35–105 mg once daily
PO; (Triplex: delayed release):
45–135 mg once daily
Myalgia, flulike syndrome, nausea, vomiting,
increased serum transaminase and creatinine levels
Rhabdomyolysis, cholelithiasis, pancreatitis
gemfibrozil
(Lopid)
PO; 600 mg bid (max: 1,500 mg/day)
PO; 4 g daily with food
Arthralgia
Hypersensitivity
niacin (Niaspan)
Hyperlipidemia: PO; 1.5–3 g daily in
divided doses (max: 6 g/day)
Niacin deficiency: PO; 10–20 mg
daily
Flushing, nausea, pruritus, headache, bloating, diarrhea
Dysrhythmias
omega-3-acid ethyl esters (Lovaza)
PO; 4
g daily with food
Eructation, dyspepsia, fishy taste
Hypersensitivity
Note: Italics indicate common adverse
effects; underlining indicates serious adverse effects
OTHER AGENTS
ezetimibe (Zetia)
Hyperlipidemia: PO; 10 mg
daily
Arthralgia, fatigue, upper respiratory tract infection,
diarrhea, elevation ofhepatic enzymes
Rhabdomyolysis
icosapent (Vascepa)
PO; 4 g daily with food
Arthralgia
Hypersensitivity
niacin (Niaspan)
Hyperlipidemia: PO;
1.5–3 g daily in divided doses (max: 6 g/day)
Niacin deficiency:
PO; 10–20 mg daily
Flushing, nausea, pruritus, headache,
bloating, diarrhea
Dysrhythmias
omega-3-acid ethyl esters
(Lovaza)
PO; 4 g daily with food
Eructation, dyspepsia,
fishy taste
Hypersensitivity
Note: Italics indicate common
adverse effects; underlining indicates serious adverse effects
INTERACTIONS
Drug–Drug:
Atorvastatin interacts with many other drugs. Azole antifungals, HIV protease inhibitors, and telaprevir are contraindicated due to an increased risk for myopathy and rhabdomyolysis.
Atorvastatin may increase levels of digoxin and oral contraceptives containing norethindrone and ethinyl estradiol.
Erythromycin may increase atorvastatin levels 40%. Risk of rhabdomyolysis increases with concurrent administration of atorvastatin with macrolide antibiotics, cyclosporine, and niacin.
Ethanol should be avoided during therapy because of its effects on hepatic function.
Lab Tests: May increase serum transaminase and creatine kinase levels.
Herbal/Food: Grapefruit juice inhibits the metabolism of statins, allowing them to reach toxic levels. Red yeast rice contains small amounts of natural statins and may increase the effects of atorvastatin. Because statins also decrease the synthesis of coenzyme Q10 (CoQ10), patients may benefit from CoQ10 supplements.
Manifestations of CoQ10 deficiency include high blood pressure, congestive heart failure, and low energy.
Treatment of Overdose: There is no specific treatment for overdose.
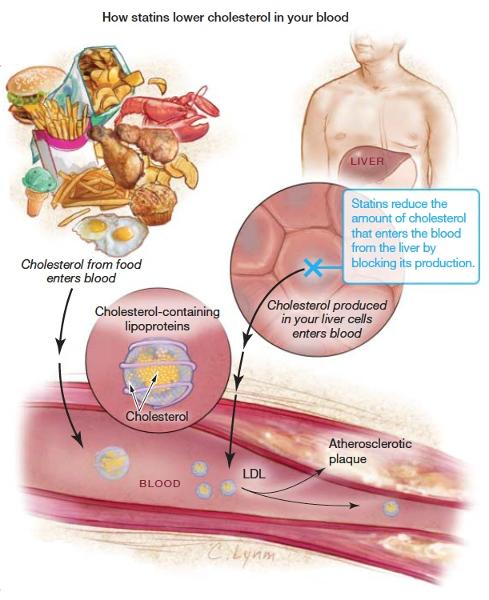
bile acid sequestrants or resins
bind bile acids, which contain a high concentration of cholesterol. Because of their large size, these drugs are not absorbed from the small intestine, and the bound bile acids and cholesterol are eliminated in the feces. The liver responds to the loss of cholesterol by making more LDL receptors, 292293which removes even more cholesterol from the blood in a mechanism similar to that of the statin drugs. The bile acid sequestrants are capable of producing a 20% drop in LDL cholesterol. They are no longer considered first-line drugs for dyslipidemias, although they are sometimes combined with statins for patients who are unable to achieve sufficient response from the statins alone. The three bile acid sequestrants have equivalent efficacy and similar safety profiles.
Cholestyramine (Questran)
Therapeutic Class: Antihyperlipidemic
Pharmacologic Class: Bile acid sequestrant
ACTIONS AND USES
Cholestyramine is a powder that is mixed with fluid before
being taken once or twice daily. It is not absorbed or metabolized
once it enters the intestine; thus, it does not produce any systemic
effects. It may take 30 days or longer to produce its maximum effect.
Questran binds with bile acids (containing cholesterol) in an
insoluble complex that is excreted in the feces. Cholesterol levels
decline due to fecal loss.
ADMINISTRATION ALERTS Mix thoroughly with 60 to 180 mL of water, noncarbonated beverages, highly liquid soups, or pulpy fruits (applesauce, crushed pineapple), and have the patient drink it immediately to avoid potential irritation or obstruction in the GI tract. Give other drugs more than 2 hours before or 4 hours after the patient takes cholestyramine. Pregnancy category C.
PHARMACOKINETICS
Onset
Peak
Duration
24–48h
1–3 wk
2–4 wk
ADVERSE EFFECTS
Although cholestyramine rarely produces serious
side effects, patients may experience constipation, bloating, gas, and
nausea that sometimes limit its use.
Contraindications: This drug
is contraindicated in patients with total biliary obstruction and in
those with prior hypersensitivity to the drug.
INTERACTIONS
Drug–Drug: Because cholestyramine can bind to other drugs, such
as digoxin, penicillins, thyroid hormone, and thiazide diuretics, and
interfere with their absorption, it should not be taken at the same
time as these other medications. Cholestyramine may increase the
effects of anticoagulants by decreasing the levels of vitamin K in the
body.
Lab Tests: Serum aspartate aminotransferase (AST),
phosphorus, chloride, and alkaline phosphatase (ALP) levels may
increase. Serum calcium, sodium, and potassium levels may
decrease.
Herbal/Food: Taking cholestyramine
with food may interfere with the absorption of the following
essential nutrients: beta-carotene, calcium, folic acid, iron,
magnesium, vitamin B12, vitamin D, vitamin E, vitamin K, and zinc.
Manifestations of nutrient depletion may include weakened immune
system, cardiovascular problems, and osteoporosis.
is a vitamin-like substance found in most animal cells. It is an essential component in the cell’s mitochondria for producing energy or ATP. Because the heart requires high levels of ATP, a sufficient level of CoQ10 is essential to that organ. Foods richest in this substance are pork, sardines, beef heart, salmon, broccoli, spinach, and nuts. Older adults appear to have an increased need for CoQ10
Coenzyme Q10 (CoQ10)
Gemfibrozil (Lopid)
Therapeutic Class: Antihyperlipidemic
Pharmacologic Class: Fibric acid agent (fibrate)
ACTIONS AND
USES
Effects of gemfibrozil include up to a 50% reduction in
VLDL with an increase in HDL. The mechanism of achieving this action
is unknown. It is less effective than the statins at lowering LDL;
thus, it is not a drug of first choice for reducing LDL levels.
Gemfibrozil is taken orally at 600 to 1,200
mg/day.
ADMINISTRATION ALERTS Administer with meals to decrease
GI distress. Pregnancy category B.
PHARMACOKINETICS
Onset
Peak
Duration
1–2 h
1–2 h
2–4 months
ADVERSE EFFECTS
Gemfibrozil produces few serious adverse
effects, but it may increase the likelihood of gallstones and may
occasionally affect liver function. The most common adverse effects
are GI related: dyspepsia, diarrhea, nausea, and
cramping.
Contraindications: Gemfibrozil is contraindicated in
patients with hepatic impairment, severe renal dysfunction, or
pre-existing gallbladder disease, or those with prior hypersensitivity
to the drug.
INTERACTIONS
Drug–Drug: Concurrent use of
gemfibrozil with oral anticoagulants may potentiate anticoagulant
effects. Concurrent use with statins should be avoided because this
increases the risk of myopathy and rhabdomyolysis. Gemfibrozil may
increase the effects of certain antidiabetic agents, statins,
sulfonylureas, and vitamin K antagonists.
Lab Tests: May increase
liver enzyme values, and CPK and serum glucose levels. May decrease
hemoglobin (Hgb), hematocrit (Hct), and WBC counts.
Herbal/Food:
Fatty foods may decrease the efficacy of gemfibrozil.
Treatment
of Overdose: There is no specific treatment for overdose
is absorbed from the intestinal lumen by cells in the jejunum of the small intestine
Cholesterol
Lipids can be classified into three types, based on their chemical structures
triglycerides, phospholipids, and sterols.Triglycerides and cholesterol are blood lipids that can lead to atherosclerotic plaque
______________are carried through the blood as lipoproteins; VLDL and LDL are associated with an increased incidence of cardiovascular disease, whereas HDL exerts a protective effect.
Lipids
1. The client is to begin taking atorvastatin (Lipitor) and the nurse is providing education about the drug. Which symptom related to this drug should be reported to the health care provider?
1. Constipation 2. Increasing muscle or joint pain 3. Hemorrhoids 4. Flushing or “hot flash”
1. Answer: 2
Rationale: “Statins”
(HMG-CoA reductase inhibitors) such as atorvastatin (Lipitor) may
cause rhabdomyolysis, a rare but serious adverse effect. Options 1,
3, and 4 are incorrect. Constipation and hemorrhoids may result from
bile acid sequestrants. A feeling of flushing or hot flash-type
effects may result from nicotinic acid. Cognitive Level: Analyzing.
Nursing Process: Implementation. Client Need: Physiological Integrity.
2. A client is receiving cholestyramine (Questran) for elevated low-density lipoprotein (LDL) levels. As the nurse completes the nursing care plan, which of the following adverse effects will be included for continued monitoring?
2. Answer: 1
Rationale: Obstruction of the GI tract is one of
the most serious complications of bile acid sequestrants. Abdominal
pain may signal the presence of obstruction. Options 2, 3, and 4 are
incorrect. Cholestyramine (Questran) does not cause orange-red urine
and saliva, sore throat, or fever, or affect capillary refill.
Cognitive Level: Applying. Nursing Process: Planning. Client Need:
Physiological Integrity.
3. The nurse is instructing a client on home use of niacin and will include important instructions on how to take the drug and about its possible adverse effects. Which of the following may be expected adverse effects of this drug? (Select all that apply.)
1. Fever and chills 2. Intense flushing and hot flashes 3. Tingling of the fingers and toes 4. Hypoglycemia 5. Dry mucous membranes
3. Answer: 2, 3
Rationale: Intense
flushing and hot flashes occur in almost every client who is taking
niacin. Tingling of the extremities may also occur. Options 1, 4, and
5 are incorrect. Fever, chills, or dry mucous membranes are not
adverse effects associated with niacin. Niacin may cause an increase
in blood glucose, especially in people with diabetes. Cognitive
Level: Analyzing. Nursing Process: Implementation. Client Need:
Physiological Integrity.
.
4. The community health nurse is working with a client taking simvastatin (Zocor). Which client statement may indicate the need for further teaching about this drug? 1. “I’m trying to reach my ideal body weight by increasing my exercise.” 2. “I didn’t have any symptoms even though I had high lipid levels. I hear that’s common.” 3. “I’ve been taking my pill before my dinner.” 4. “I take my pill with grapefruit juice. I’ve always taken my medications that way.” 297298
1. “I’m trying to reach my ideal body weight by increasing my exercise.” 2. “I didn’t have any symptoms even though I had high lipid levels. I hear that’s common.” 3. “I’ve been taking my pill before my dinner.” 4. “I take my pill with grapefruit juice. I’ve always taken my medications that way.” 297298
4. Answer: 4
Rationale: Grapefruit juice
inhibits the metabolism of statins such as simvastatin (Zocor),
allowing them to reach higher serum levels and increasing the risk of
adverse effects. Options 1, 2, and 3 are incorrect. Most clients with
lipid disorders are asymptomatic and maintaining ideal body weight
and increasing exercise are important components of a holistic plan
of care. Because cholesterol biosynthesis is higher at night, taking
the drug in the evening may ensure that peak levels are reached
during the night-time hours. Cognitive Level: Applying. Nursing
Process: Evaluation. Client Need: Health Promotion and Maintenance.
5. A client has been on long-term therapy with colestipol (Colestid). To prevent adverse effects related to the length of therapy and lack of nutrients, which of the following supplements may be required? (Select all that apply.)
1. Folic acid 2. Vitamins A, D, E, and K 3. Potassium, iodine, and chloride 4. Protein 5. B vitamins
5. Answer: 1, 2
Rationale: Long-term use
of bile acid sequestrants such as colestipol (Colestid) may cause
depletion or decreased absorption of folic acid and the fat-soluble
vitamins. Options 3, 4, and 5 are incorrect. Decreases in protein,
potassium, iodine, chloride, and the B vitamins are not a direct
effect of bile acid sequestrant therapy. Cognitive Level: Applying.
Nursing Process: Planning. Client Need: Physiological Integrity.
6. A client has been ordered gemfibrozil (Lopid) for hyperlipidemia. The nurse will first validate the order with the health care provider if the client reports a history of which disorder?
1. Hypertension 2. Angina 3. Gallbladder disease 4. Tuberculosis
6. Answer: 3
Rationale: Fibric acid agents
(fibrates) may cause or worsen gallbladder disease and the order
should be checked with the provider before giving. Options 1, 2, and
4 are incorrect. Hypertension and angina may indicate the existence
of atherosclerosis and arteriosclerosis; both are indications for
lipid-lowering therapy. A history of tuberculosis would not be a
rationale for withholding the drug. Cognitive Level: Applying.
Nursing Process: Implementation. Client Need: Physiological Integrity
1. The nurse is preparing a teaching plan for a 39-year-old female patient who has been prescribed atorvastatin (Lipitor). Identify key information
1. Atorvastatin (Lipitor) is used along with diet and exercise modifications to lower serum lipid levels. After assessing the patient’s current diet for possible modifications, the nurse may consider the need for consultation with a dietitian, or may include teaching about how to make small modifications over time (e.g., switching to a smaller plate size so that portions seem larger or using the “My Plate” visual guide to increase amounts of vegetables and fruits). Because atorvastatin is a category X drug and this patient is within child-bearing age, clear instruction on the need to avoid pregnancy during drug therapy is vital. Atorvastatin may be taken at any time of the day. Although headache and GI complaints may be common, any unusual soreness or muscle pain, especially if increasing, should be reported to the health care provider. Periodic laboratory testing will also be needed to ensure that the drug is having therapeutic effects and that no adverse effects such as hepatotoxicity are occurring. 2. Cholestyramine (Questran), like other bile acid sequestrants, has the possibility of causing esophageal irritation, so taking the proper fluids or food with this medication is important. Mixing the drug powder well with fruit juice or with pulpy fruit such as applesauce, followed by a glass of water, may decrease the occurrence of esophageal irritation, and it also may help prevent the constipation caused by the drug. Any other medications must be taken 2 hours before or 4 hours after the cholestyramine to prevent a potential delay in absorption or binding of the drug. 3. The nurse should assess the amount of niacin the patient is taking and advise him to seek medical advice before self-medicating, especially because this patient also has diabetes, and many drugs may affect blood glucose levels or interact with drugs used to treat diabetes. Niacin may cause a rise in fasting glucose levels and his serum glucose levels should be evaluated. The flushing and hot flashes are normal side effects of niacin; if his health care provider recommends that he continue taking it, the nurse may recommend taking the drug with cold water and, after confirming with his provider, with one 325 mg of aspirin.
2. A patient has been prescribed cholestyramine (Questran) for elevated lipids. What teaching is important for this patient?
2. Cholestyramine (Questran), like other bile acid sequestrants, has the possibility of causing esophageal irritation, so taking the proper fluids or food with this medication is important. Mixing the drug powder well with fruit juice or with pulpy fruit such as applesauce, followed by a glass of water, may decrease the occurrence of esophageal irritation, and it also may help prevent the constipation caused by the drug. Any other medications must be taken 2 hours before or 4 hours after the cholestyramine to prevent a potential delay in absorption or binding of the drug.
3. A male patient with diabetes presents to the emergency department with complaints of being flushed and having “hot flashes.” The patient admits to self-medicating with niacin for elevated lipids. What is the nurse’s best response?
3. The nurse should assess the amount of niacin the patient is taking and advise him to seek medical advice before self-medicating, especially because this patient also has diabetes, and many drugs may affect blood glucose levels or interact with drugs used to treat diabetes. Niacin may cause a rise in fasting glucose levels and his serum glucose levels should be evaluated. The flushing and hot flashes are normal side effects of niacin; if his health care provider recommends that he continue taking it, the nurse may recommend taking the drug with cold water and, after confirming with his provider, with one 325 mg of aspirin.
1. The client is prescribed digoxin (Lanoxin) for treatment of HF. Which of the following statements by the client indicates the need for further teaching? 1. “I may notice my heart rate decrease.” 2. “I may feel tired during early treatment.” 3. “This drug should cure my heart failure.” 4. “My energy level should gradually improve.”
1. Answer: 3
Rationale: Digoxin helps increase the contractility
of the heart, thus increasing cardiac output. But it is not a cure for
heart failure, only a treatment option. Options 1, 2, and 4 are
incorrect. The client is correct that the heart rate will decrease
with the use of digoxin, tiredness may be noted in early therapy until
the heart failure has improved, and energy levels will gradually
improve. Cognitive Level: Analyzing. Nursing Process: Evaluation.
Client Need: Physiological Integrity.
inhibitors because this can
increase the likelihood of dysrhythmias. Options 1, 2, and 4 are
incorrect. Weight, presence of edema, and dietary intake of sodium
will be monitored because of their relationship to HF and monitoring
for therapeutic improvement but they are not crucial to assess before
beginning therapy. The client’s sleep patterns or presence of sleep
apnea has no direct relationship with the drug but monitoring may be
ordered for other reasons. Cognitive Level: Analyzing. Nursing
Process: Assessment. Client Need: Physiological Integrity.
2. The nurse reviews laboratory studies of a client receiving digoxin (Lanoxin). Intervention by the nurse is required if the results include which of the following laboratory values? 1. Serum digoxin level of 1.2 ng/dL 2. Serum potassium level of 3 mEq/L 3. Hemoglobin of 14.4 g/dL 4. Serum sodium level of 140 mEq/L
2. Answer: 2
Rationale: Normal serum potassium level is 3.5 to 5
mEq/L. Hypokalemia may predispose the client to digitalis toxicity.
Options 1, 3, and 4 are incorrect. A digoxin level of 1.2 ng/dL is
within therapeutic range. A hemoglobin of 14.4 g/dL and a serum sodium
of 140 mEq/L are also within normal range. Cognitive Level: Analyzing.
Nursing Process: Evaluation. Client Need: Physiological Integrity.
3. A client with heart failure has an order for lisinopril (Prinivil, Zestril). Which of the following conditions in the client’s history would lead the nurse to confirm the order with the provider? 1. A history of hypertension previously treated with diuretic therapy 2. A history of seasonal allergies currently treated with antihistamines 3. A history of angioedema after taking enalapril (Vasotec) 4. A history of alcoholism, currently abstaining
3. Answer: 3
Rationale: Angioedema is a rare but potentially
serious adverse effect from ACE inhibitors; because this client has
had a previous reaction to another drug within the same group
(enalapril/Vasotec), the nurse should confirm the order with the
provider. Options 1, 2, and 4 are incorrect. The use of diuretics
along with ACE inhibitors must be closely monitored but this client
was previously on diuretic therapy and it may be assumed that the
client is no longer taking it. The use of antihistamines concurrently
with lisinopril may help to relieve any dry cough that occurs with the
lisinopril. While a history of alcoholism may suggest more frequent
hepatic monitoring, the client is currently abstaining. Cognitive
Level: Analyzing. Nursing Process: Assessment. Client Need:
Physiological Integrity.
4. The teaching plan for a client receiving hydralazine (Apresoline) should include which of the following points? 1. Returning for monthly urinalysis testing 2. Including citrus fruits, melons, and vegetables in the diet 3. Decreasing potassium-rich food in the diet 4. Rising slowly to standing from a lying or sitting position
4. Answer: 4
Rationale: Hydralazine (Apresoline) commonly causes
orthostatic hypotension and the client should be taught to rise slowly
from a lying or sitting position to standing. Options 1, 2, and 3 are
incorrect. Hydralazine does not require monthly urinalysis testing.
Potassium levels will be monitored along with other electrolytes, but
the client does not need to decrease the amount of potassium-rich
foods in the diet and a healthy balance of all foods is encouraged.
Cognitive Level: Applying. Nursing Process: Planning. Client Need:
Physiological Integrity.
5. Lisinopril (Prinivil) is part of the treatment regimen for a client with HF. The nurse monitors the client for the development of which of the following adverse effects of this drug? (Select all that apply.) 1. Hyperkalemia 2. Hypocalcemia 3. Cough 4. Dizziness 5. Heartburn
5. Answer: 1, 3, 4
Rationale: Common adverse effects of
lisinopril (Prinvil) and other ACE inhibitors include cough, headache,
dizziness, change in sensation of taste, vomiting and diarrhea, and
hypotension. Hyperkalemia may occur, especially when the drug is taken
concurrently with potassium-sparing diuretics. Options 2 and 5 are
incorrect. Hypercalcemia and heartburn are not adverse effects
associated with the ACE inhibitors. Cognitive Level: Analyzing.
Nursing Process: Evaluation. Client Need: Physiological Integrity.
6. The client who has not responded well to other therapies has been prescribed milrinone (Primacor) for treatment of his heart failure. What essential assessment must the nurse make before starting this drug? 1. Weight and presence of edema 2. Dietary intake of sodium 3. Electrolytes, especially potassium 4. History of sleep patterns and presence of sleep apnea
6. Answer: 3
Rationale: Electrolytes, especially potassium for
the presence of hypokalemia, should be assessed before beginning
milrinone (Primacor) or any phosphodiesterase inhibitory. Hypokalemia
should be corrected before administering phosphodiesterase
1. A patient is newly diagnosed with mild heart failure. The patient has been started on digoxin (Lanoxin). What objective evidence would indicate that this drug has been effective?
1. The nurse should note improved signs of perfusion including the patient’s skin color (e.g., warm, noncyanotic), blood pressure and heart rate within normal limits or to parameters set by the provider, and an increase in urine output. If lung congestion was present, adventitious lung sounds should be clearing or absent. The ECG may also show improvement if dysrhythmias were present before beginning drug therapy.
2. A 69-year-old patient has a sudden onset of acute pulmonary edema. The patient has no past cardiac history, is allergic to sulfa antibiotics, and routinely takes no medications. The health care provider orders furosemide (Lasix) to relieve the pulmonary congestion, along with digoxin (Lanoxin) to improve the patient’s hemodynamic status. What interventions are essential in the care of this patient?
2. There is a potential cross-sensitivity between sulfa and furosemide (Lasix) and the nurse should notify the health care provider of the patient’s allergy before beginning the medication. Because furosemide will cause loss of potassium, the nurse will frequently monitor the patient’s serum potassium levels while the patient is on digoxin (Lanoxin). Hypokalemia may increase the risk for dysrhythmias related to digoxin therapy.
3. A patient who has diabetes and hypertension is started on lisinopril (Prinivil) for mild heart failure. What teaching is important for this patient?
3. This patient with diabetes should have a baseline assessment of renal function to detect any decline in renal function and electrolyte levels. Hyperkalemia may occur during drug therapy with lisinopril (Prinvil) and patients 824825with renal insufficiency may be at greater risk. The patient should be taught to maintain normal amounts of potassium-containing foods in his diet; avoid the use of salt substitutes, which contain potassium; and return regularly for laboratory tests to monitor his kidney function and other values. The lisinopril will also treat the patient’s hypertension but the nurse should assess what other medications the patient is currently taking for the condition. Safety should be emphasized, especially regarding postural hypotension and the patient should be taught to rise slowly from a lying or sitting position to standing.
1. The client is being discharged with nitroglycerin (Nitrostat) for sublingual use. While planning client education, what instruction will the nurse include? 1. “Swallow three tablets immediately for pain and call 911.” 2. “Put one tablet under your tongue for chest pain. If pain does not subside, you may repeat in 5 minutes, taking no more than three tablets.” 3. “Call your health care provider when you have chest pain. He will tell you how many tablets to take.” 4. “Place three tablets under your tongue and call 911.”
1. Answer: 2
Rationale: At the initial onset of chest pain,
sublingual nitroglycerin is administered and three doses may be taken
5 minutes apart. Pain that persists 5 to 10 minutes after the initial
dose may indicate an MI, and the client should seek emergency medical
assistance for more definitive diagnosis and care. Options 1, 3, and 4
are incorrect. Nitroglycerin sublingual dosing should not be swallowed
and no more than one tablet is administered at a time. Trying to reach
the health care provider may cause unnecessary delays in treatment.
Cognitive Level: Applying. Nursing Process: Planning. Client Need:
Physiological Integrity.
2. Nitroglycerin patches have been ordered for a client with a
history of angina. What teaching will the nurse give to this client?
1. Keep the patches in the refrigerator. 2. Use the patches only if
the chest pain is severe. 3. Remove the old patch before applying a
new one. 4. Apply the patch only to the upper arm or thigh areas. in
prolonged and severe hypotension when combined with nitrates. 3. They
will adequately treat the patient’s angina as well as erectile
dysfunction. 4. They will increase the possibility of nitrate
tolerance developing and should be avoided unless other drugs can be
used.
CRITICAL THINKING QUESTIONS 1. A patient on the medical
unit is complaining of chest pain (4 on a scale of 10), has a history
of angina, and is requesting his PRN nitroglycerin spray. The
patient’s blood pressure is 96/60 mmHg at present. Identify what the
nurse should do. 2. A patient is recovering from an acute MI and has
been put on atenolol (Tenormin). What teaching should the patient
receive prior to discharge from the hospital? 3. A patient with chest
pain has been given the calcium channel blocker diltiazem (Cardizem)
IV for a heart rate of 118 beats per minute. Blood pressure at this
time is 100/60 mmHg. What precautions should the nurse take?
2. Answer: 3
Rationale: To prevent the development of nitrate
tolerance, nitroglycerin patches are often removed at night for 6 to
12 hours. Options 1, 2, and 4 are incorrect. The patches should not be
kept in the refrigerator unless excessive room temperatures are
anticipated and then only under the direction of the pharmacist or
health care provider. Nitroglycerin patches provide long-term control
of angina and should not be used only when the chest pain is severe.
They should be applied to hair-free areas of the torso and not on the
arms or legs. Muscle activity in these areas may increase drug
absorption. Cognitive Level: Applying. Nursing Process:
Implementation. Client Need: Physiological Integrity.
3. Which of the following assessment findings in a client who is receiving atenolol (Tenormin) for angina would be cause for the nurse to hold the drug and contact the provider? (Select all that apply.) 1. Heart rate of 50 beats/minute 2. Heart rate of 124 beats/minute 3. Blood pressure 86/56 4. Blood pressure 156/88 5. Tinnitus and vertigo
3. Answer: 1, 3
Rationale: Atenolol (Tenormin) decreases blood
pressure and heart rate. The administration of this drug may cause
significant hypotension and bradycardia in some clients. Options 2, 4,
and 5 are incorrect. Atenolol is given to treat tachycardia and
hypertension as well as angina. Tinnitus and vertigo are not adverse
effects associated with atenolol. Cognitive Level: Analyzing. Nursing
Process: Evaluation. Client Need: Physiological Integrity.
4. The nurse is caring for a client with chronic stable angina who is receiving isosorbide dinitrate (Isordil). Which of the following are common adverse effects of isosorbide? 1. Flushing and headache 2. Tremors and anxiety 3. Sleepiness and lethargy 4. Light-headedness and dizziness 375376
4. Answer: 4
Rationale: Lightheadedness and dizziness may occur
secondary to the hypotensive effects of the isosorbide (Isordil).
Options 1, 2, and 3 are incorrect. The oral form of isosorbide has a
slower onset than the sublingual form and flushing and headache are
not usually experienced. Tremors, anxiety, sleepiness, or lethargy are
not associated effects from the drug and if they occur, other causes
should be investigated. Cognitive Level: Analyzing. Nursing Process:
Evaluation. Client Need: Physiological Integrity.
5. Place the following nursing interventions in order for a client who is experiencing chest pain. 1. Administer nitroglycerin sublingually. 2. Assess heart rate and blood pressure. 3. Assess he location, quality, and intensity of pain. 4. Document interventions and outcomes. 5. Evaluate the location, quality, and intensity of pain.
5. Answer: 3, 2, 1, 5, (2), 4
Rationale: Prior to administering
nitrates for chest pain, the nurse must first assess the location,
quality, and intensity of pain. Blood pressure and heart rate should
be assessed and the health care provider contacted if the blood
pressure is below 90/60 (or below previously established parameters)
or if tachycardia is present before administering the dose. Once
nitrates are administered, the location, quality, and intensity of the
pain are evaluated after 5 minutes. If the pain is still present, the
blood pressure and pulse should be reassessed before giving another
dose (the second (2) above). Documentation of drug administration and
client outcomes is completed after administration and re-evaluation.
Cognitive Level: Applying. Nursing Process: Implementation. Client
Need: Physiological Integrity.
6. Erectile dysfunction drugs such as sildenafil (Viagra) are contraindicated in clients taking nitrates for angina. What is the primary concern with concurrent administration of these drugs?
6. Answer: 2
Rationale: Erectile dysfunction drugs such as
sildenafil (Viagra), vardenafil (Levitra), and tadalafil (Cialis)
decrease BP. When combined with nitrates, severe and prolonged
hypotension may result. Options 1, 3, and 4 are incorrect. Erectile
dysfunction drugs do not contain nitrates and do not lead to nitrate
tolerance. These drugs are not recognized as useful for the treatment
of anginal pain. Cognitive Level: Analyzing. Nursing Process:
Implementation. Client Need: Physiologic Integrity.
Normal Parameters of the following:
Heart rate (HR)
Cardiac output (CO) and cardiac index (CO/CI)
Stroke volume (SV)
Systemic vascular resistance (SVR)
Pulmonary artery
systolic and diastolic pressures (PAS/PAD)
Mean systemic
arterial (MAP)
pulmonary arterial pressures (MPAP)
Mixed
venous oxygen saturation (SvO2)
HR: 60-100
CO: 4-8 L/min
CO/CI: 2.5-4.0 L/min/m2
SV: 60-100 ml/beat
SVR: 800-1200 dynes/sec/cm2
PAS 20-30
mm Hg
PAD 6-12 mm Hg
MAP 70-105
MPAP 10-20 mm
Hg
SvO2 80-100%
What are the effects of each of the following types of drugs:
1. positive inotropy
2. positive chronotropy
3. positive dromotropy
inotropy = increased contraction
chromotropic = increased
HR
dromotropy = increased electrical conduction
What will be the CO, SV, SVR, SvO2, and urine output of the patient
receiving positive:
1. Inotropic
2. Chronotropic
3.
Dromotropic drugs?
1. Inotropic: Contraction
- increased CO
- increased SV
- increased SvO2
- not sure about
SVR
- increased urine output
2. Chronotropic: Heart Rate
- decreased
CO
- decreased SV
- decreased SVR
- decreased
SvO2
- decreased urine output
3. Dromotropic: Cardiac Conduction
I find the
answer to this dependent upon HOW much conduction is increased. An
increase in HR and conduction can really either increase CO, SV, SVR,
SvO2, and urine output, or decrease it. It depends on the baseline condition.
Lisinopril, captopril, enalapril, ramipril...etc. class
Ace inhibitors
Lisinopril, captopril, enalapril, ramipril....etc. indications
Heart failure
Hypertension
Ace inhibitor mechanism of action (ie. lisinopril, enalapril, captopril...etc.)
Inhibits aldosterone secretion (blocks sodium and water resorption) --> diuresis --> decreased preload --> decreased workload on the heart
Losartan, Irbesartan, Valsartan class
ARB (angiotensin receptor blockers)
Losartan, Irbesartan, Valsartan mechanism of action
blocks the angiotensin II receptors -->
vasodilation --> decreased afterload
***All ARBS are similar
in action except for losartan-hydrochlorothiazide
Metoprolol and carvedilol class
Beta Blockers
metoprolol and carvedilol mechanism of action
Reduce SNS stimulation = reduced HR and contractility = reduced hypertrophy
Spironolactone and Eplerenone Class
Aldosterone antagonist
*Spironolactone is
actually a potassium sparing diuretic
Spironolactone mechanism of action
Works at the distal convoluted tubule to prevent water resorption- also keeps in potassium
Eplerenone mechanism of action
selective aldosterone b
1. Inotropic: Contraction
- increased CO
- increased
SV
- increased SvO2
- not sure about SVR
- increased
urine output
2. Chronotropic: Heart Rate
- decreased
CO
- decreased SV
- decreased SVR
- decreased
SvO2
- decreased urine output
3. Dromotropic: Cardiac Conduction
I find the
answer to this dependent upon HOW much conduction is increased. An
increase in HR and conduction can really either increase CO, SV, SVR,
SvO2, and urine output, or decrease it. It depends on the baseline condition.
Lisinopril, captopril, enalapril, ramipril...etc. class
Ace inhibitors
Lisinopril, captopril, enalapril, ramipril....etc. indications
Heart failure
Hypertension
Ace inhibitor mechanism of action (ie. lisinopril, enalapril, captopril...etc.)
Inhibits aldosterone secretion (blocks sodium and water resorption) --> diuresis --> decreased preload --> decreased workload on the heart
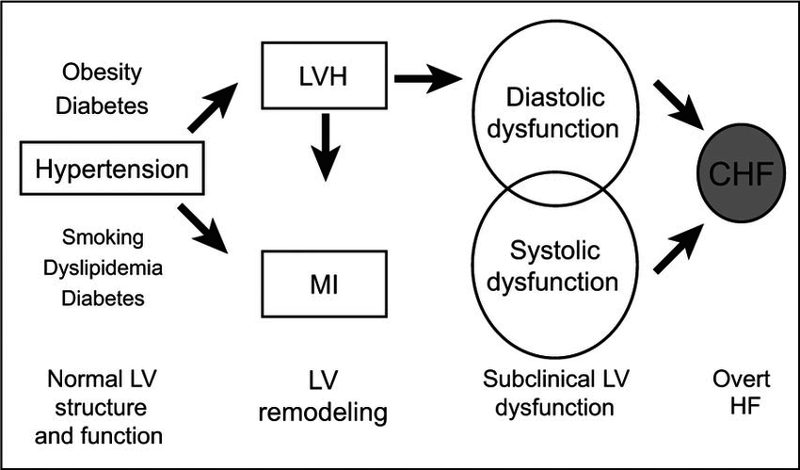




Coronary Atherosclerosis
¨Atherosclerosis is the abnormal accumulation of lipid deposits and fibrous tissue within arterial walls and lumen.
¨In coronary atherosclerosis, blockages and narrowing of the coronary vessels reduce blood flow to the myocardium.
¨Cardiovascular disease is the leading cause of death in the United States for men and women of all racial and ethnic groups.
¨CAD, coronary artery disease, is the most prevalent cardiovascular disease in adults.
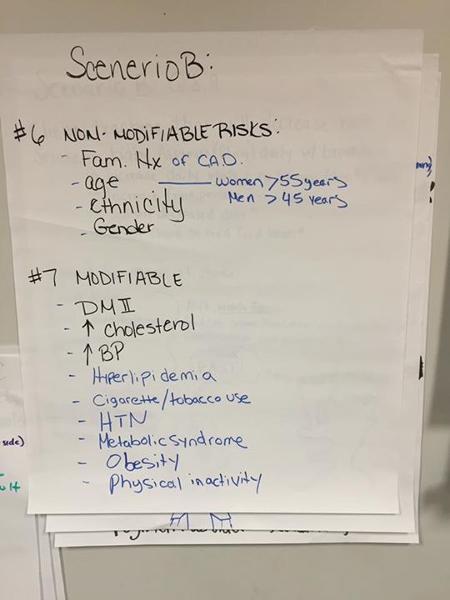
¨Nonmodifiable
¤Family history of CAD (first degree relative)
¤Increasing age (>45yrs for men; >55yrs for women)
¤Gender
¤Race (African American higher incidence)
¨Modifiable
¤Hyperlipidemia
¤Cigarette/tobacco use
¤HTN
¤DM
¤Metabolic Syndrome
¤Obesity
¤Physical inactivity
Risk factors for CAD and prevention
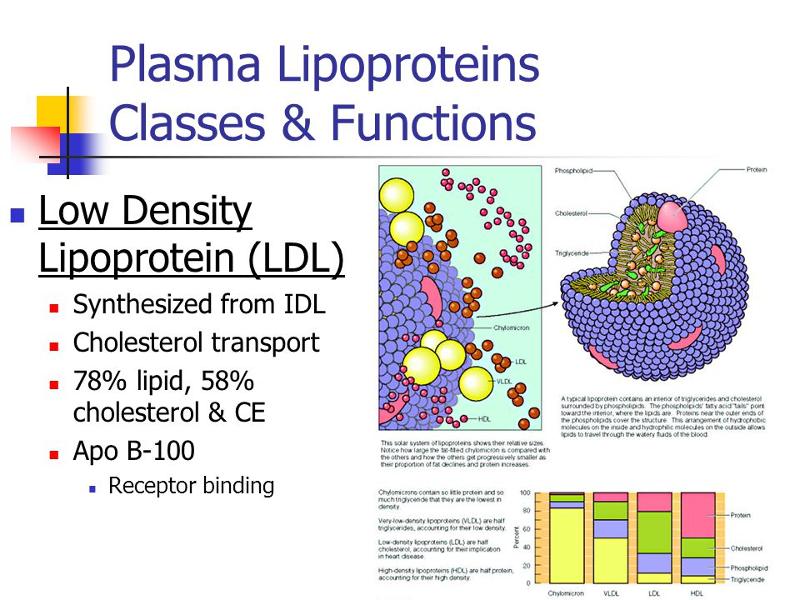
¨Water insoluble fats are encased in lipoproteins which permits transportation within the circulatory system
¤Lipoproteins are classified by density, which increases with the presence of protein
¤Four elements of fat metabolism
nTotal cholesterol
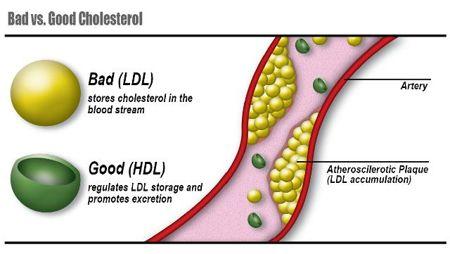
nLDL: “Bad” deposits on the artery walls
nHDL: “Good” carries cholesterol from artery wall to liver
nTriglycerides: fat made by the body; associated with diets high in carbs.
Cholesterol
¨Diet modification
¤Veggies, legumes, low fat, soluble fiber, decrease in red meat
¨Physical activity
¨Statins
¤Atorvastatin (Lipitor): blocks cholesterol synthesis, decrease LDL and TG, increase HDL
nMonitor LFTs, Rhabdomylsis
Management of Cholesterol
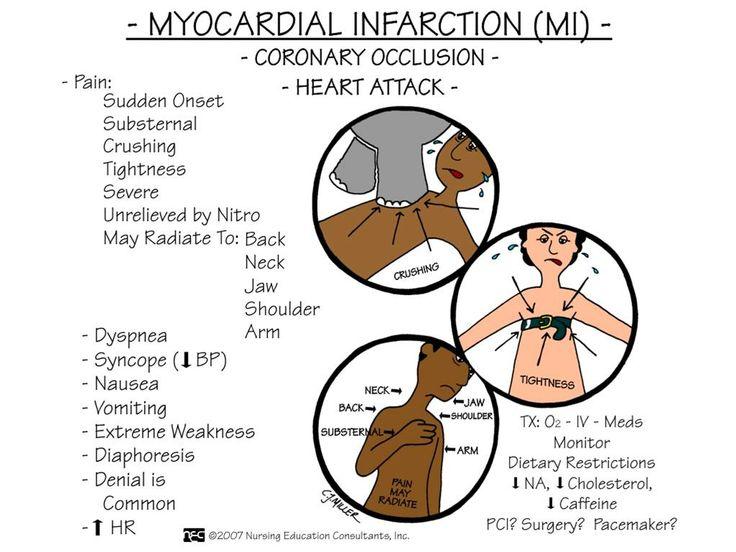
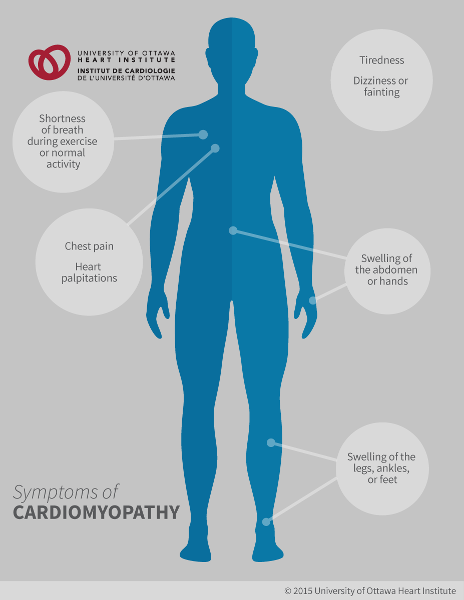
¨Symptoms of myocardial ischemia
¤Angina pectoris: chest pain from ischemia
¤Nausea, shortness of breath, weakness, referred pain
¤Dysrhythmias
¨Symptoms and complications are related to the location and degree of vessel obstruction
¤Myocardial infarction
¤Heart failure
¤Sudden cardiac death
Clinical Manifestations of CAD
¨A syndrome characterized by episodes or paroxysmal pain or pressure in the anterior chest caused by insufficient coronary blood flow; CAD is the primary cause
¤Myocardial oxygen demand increases
Physical exertion
Exposure to cold causes vasoconstriction
Heavy meal increases blood flow to mesenteric area
Stress, increase in HR
Angina Pectoris
¨Stable: predictable, consistent; pain with exertion relieved with rest and nitroglycerin
¨Unstable: symptoms increase with frequency, not relieved with rest and nitro
¨Refractory: severe incapacitating chest pain
¨Variant ( Prinzmetal’s ): pain at rest with reversible ST segment elevation; coronary artery spasms
¨Silent ischemia: objective findings of ischemia but patient denies pain.
Types of Angina and Presentation
¨Treatment seeks to decrease myocardial oxygen demand and increase oxygen supply
¨Medications
¨Oxygen
¨Reduce and control risk factors
¨Reperfusion therapy may also be done
TREATMENT OF ANGINA
¨Nitrates
vasodilatation, decreases left ventricular end diastolic pressure and left ventricular end diastolic volume (Preload), reduces myocardial oxygen consumption
¤Isosorbide (Imdur)
vasodilation decrease left ventricular end diastolic pressure and left ventricular diastolic volume (Preload), increases blood flow through coronary arteries, reduces myocardial consumption of oxygen
¨Aspirin: prevents platelet aggregation, decreases arterial wall inflammation
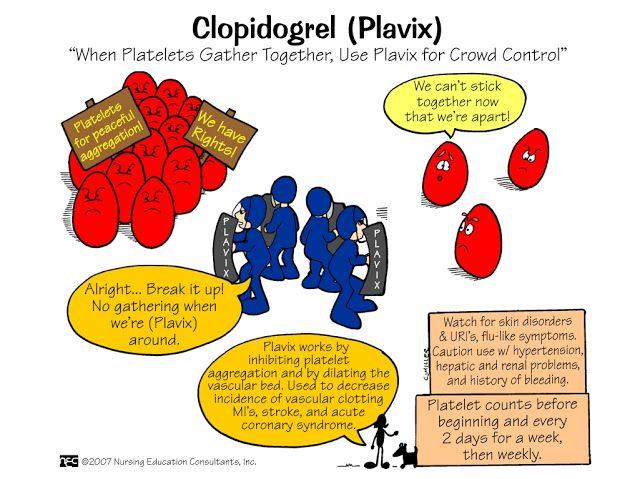
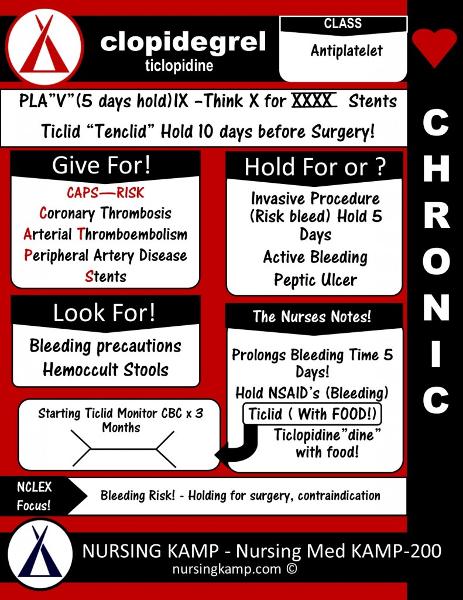
¨Clopidogrel (Plavix): inhibits platelet aggregation, by irreversibly inhibiting the binding of ATP to platelet receptors
¨Beta Blockers
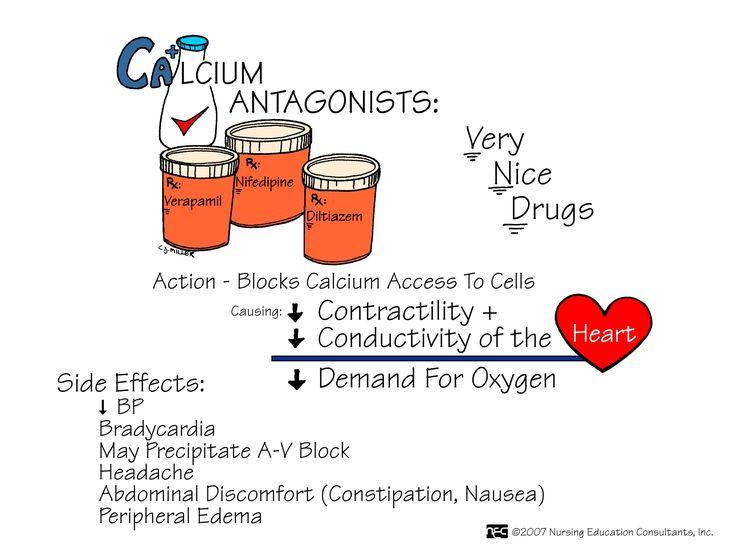
¨CCB
Pharmacotherapy Angina and CAD
¨Symptoms and activities, especially those that precede and precipitate attacks
¨Risk factors, lifestyle, and health promotion activities
¨Patient and family knowledge
¨Adherence to the plan of care
Nursing Management: CAD/Angina
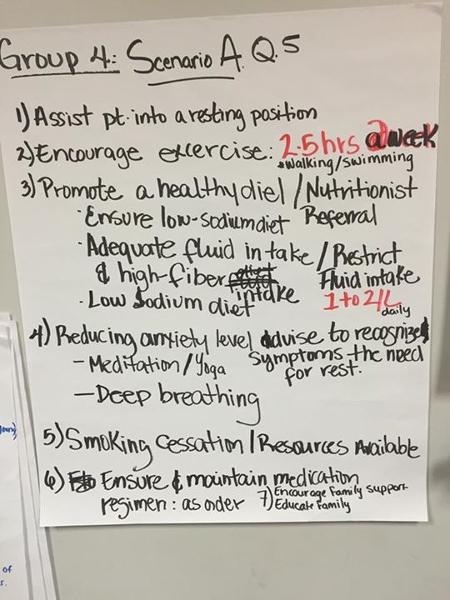
Goals include the immediate and appropriate treatment of angina, prevention of angina, reduction of anxiety, awareness of the disease process, understanding of prescribed care, adherence to the self-care program, and absence of complications
Nursing Process: The Care of the Patient with Angina Pectoris—Planning
¨Treatment of angina pain is a priority nursing concern.
¨Patient is to stop all activity and sit or rest in bed.
¨Assess the patient while performing other necessary interventions. Assessment includes VS, and observation for respiratory distress, and assessment of pain. In the hospital setting, the ECG is assessed or obtained.
¨Administer oxygen.
Administer medications as ordered or by protocol, usually NTG
Treatment of Angina Pain
¨Use a calm manner
¨Stress-reduction techniques
¨Patient teaching
¨Addressing patient spiritual needs may assist in allaying anxieties
¨Address both patient and family needs
NURSING CARE: ANXIETY
¨Lifestyle changes and reduction of risk factors
¨Explore, recognize, and adapt behaviors to avoid to reduce the incidence of episodes of ischemia
¨Teaching regarding disease process
¨Medications
¨Stress reduction
¨When to seek emergency care
PATIENT TEACHING : ANXIETY
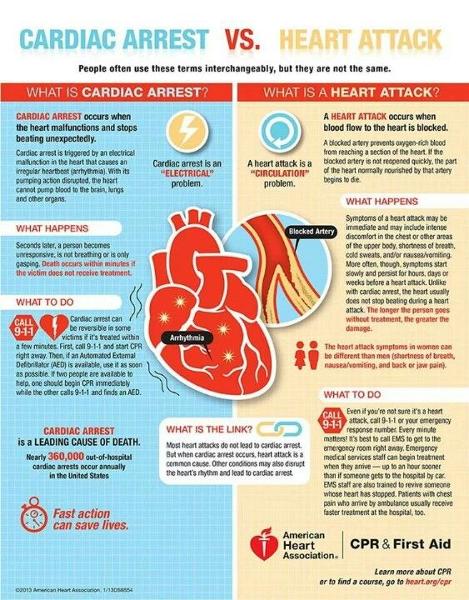
¨ACS: rupture of atherosclerotic plaque breaks off, but coronary artery is not completely occluded
¨MI: coronary artery is completely occluded, area of the myocardium is permanently destroyed.
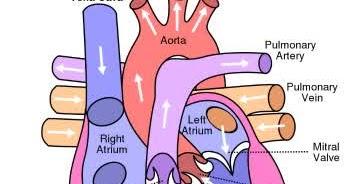
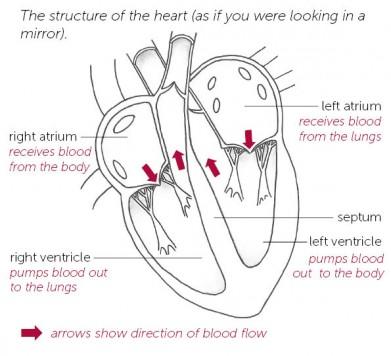
¤The right coronary artery supplies:
nright atrium, SA and AV node
nright ventricle
nbottom portion of both ventricles and back of the septum
¤The left coronary arteries supply:
nCircumflex artery - supplies blood to the left atrium, side and back of the left ventricle
nLeft Anterior Descending artery (LAD) - supplies the front and bottom of the left ventricle and the front of the septum
n
NURSING CARE:Acute Coronary Syndrome/ Myocardial Infarction
¨MI classified
¤Type: NSTEMI vs STEMI
¤Location of injury to the ventricular wall
Inferior
Anterior
Posterior
Lateral
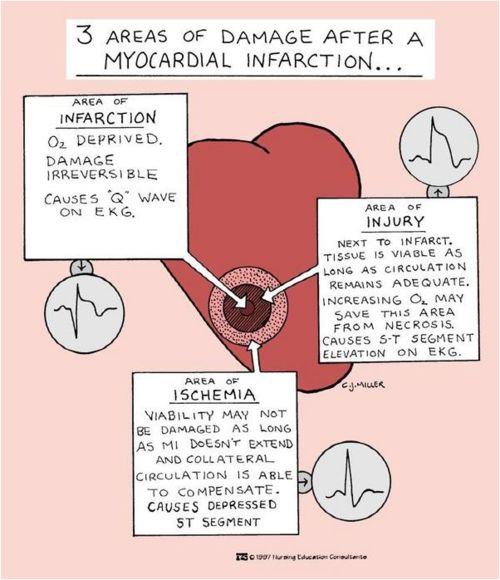
MI: Ischemia, Injury, Infarction
¨ECG (within 10 minutes of arrival)
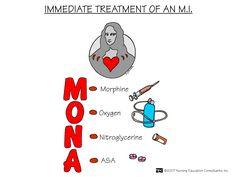
¨Oxygen
¨Aspirin, nitroglycerin, morphine, beta-blockers
¨Angiotensin-converting enzyme inhibitor within 24 hours
¨Evaluate for percutaneous coronary intervention or thrombolytic therapy
¨As indicated; IV heparin or LMWH, clopidogrel or ticlopidine, glycoprotein IIb/IIIa inhibitor
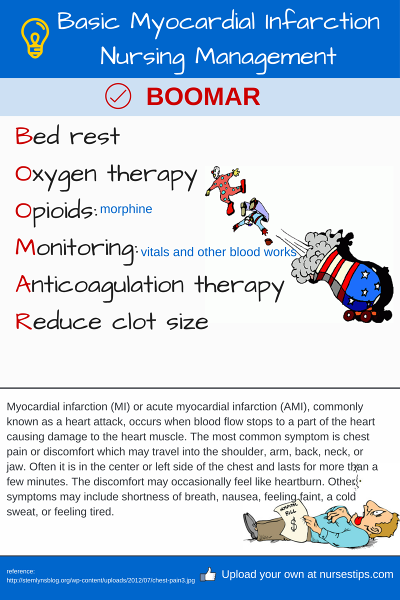
¨Bed rest
TREATMENT OF ACUTE MI
¨Laboratory tests—biomarkers
¤CK-MB: increases in a few hours, peaks within 24 hrs
¤Troponin T or I: increases in a few hours, remains elevated for a longer period, serial labs until peak then trend down
¤Myoglobin: increase within 1-3 hrs, peaks 12 hrs
¨Echo
¨Stress Test
DIAGNOSTIC TESTING: ACUTE MI
¨Relieving pain and other symptoms of ischemia
¤ balance oxygen supply and demand
¤Frequent vital signs
¨Respiratory function
¤Fluid volume status
¨Tissue Perfusion
¤Activity restrictions
¤Urine output
¤Cap refill/pulses
¨Reducing anxiety
Nursing Management: MI/ACS
¨Acute pulmonary edema
¨Heart failure
¨Cardiogenic shock
¨Dysrhythmias and cardiac arrest
¨Pericardial effusion and cardiac tamponade
COLLABORATE : MI/ACS
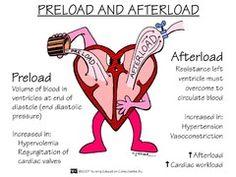
Cardiac Hemodynamics
¨CO = SV × HR
¨Preload
¨Afterload
¨Contractility
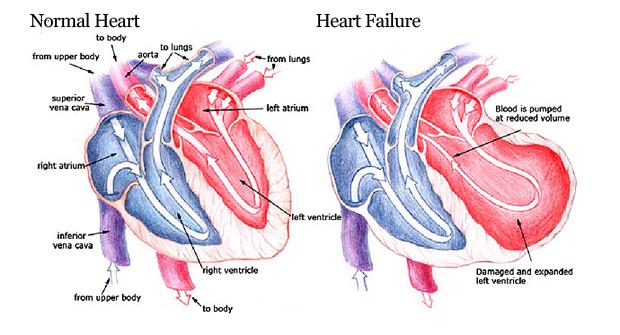
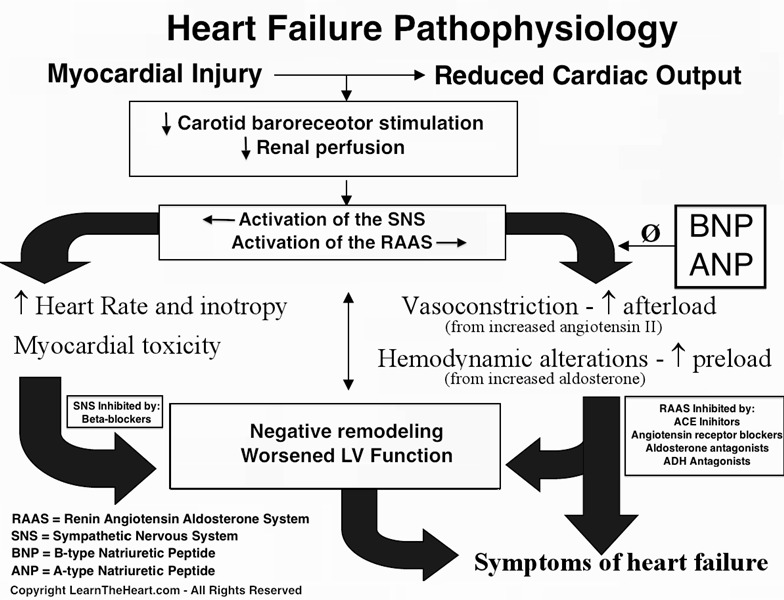
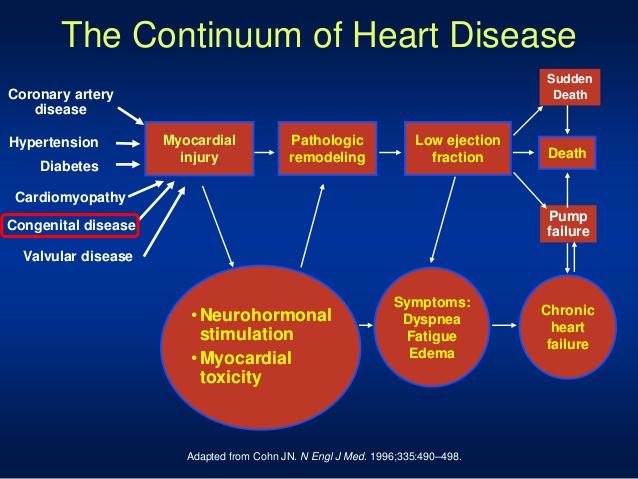
¨The inability of the heart to pump sufficient blood to meet the needs of the tissues for oxygen and nutrients.
¤A syndrome characterized by fluid overload or inadequate tissue perfusion.
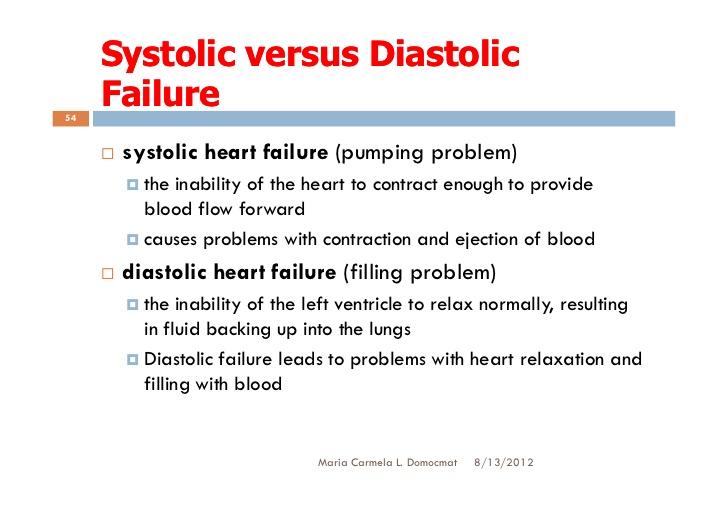
¤indicates myocardial disease, in which there is a problem with the contraction of the heart (systolic failure) or filling of the heart (diastolic failure).
¨Some cases are reversible, most heart failure is a progressive, lifelong disorder managed with lifestyle changes and medications.
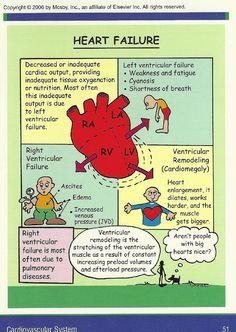
HEART FAILURE
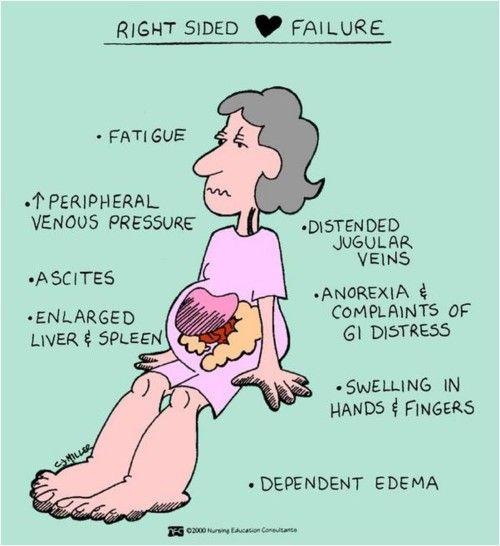
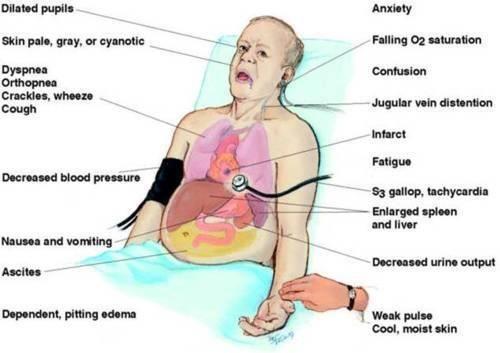
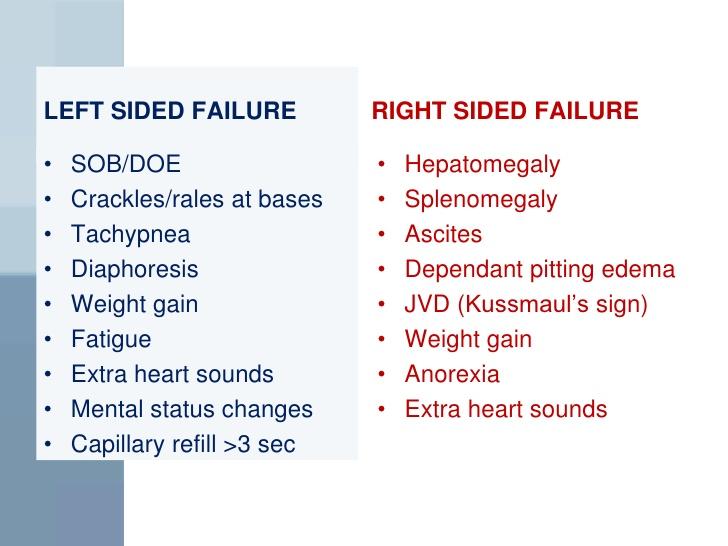
¨Right-sided failure
¤RV cannot eject sufficient amounts of blood and blood backs up in the venous system. This resuts in perpheral edema, hepatomegaly, ascites, anorexia, nausea, weakness, and weight gain.
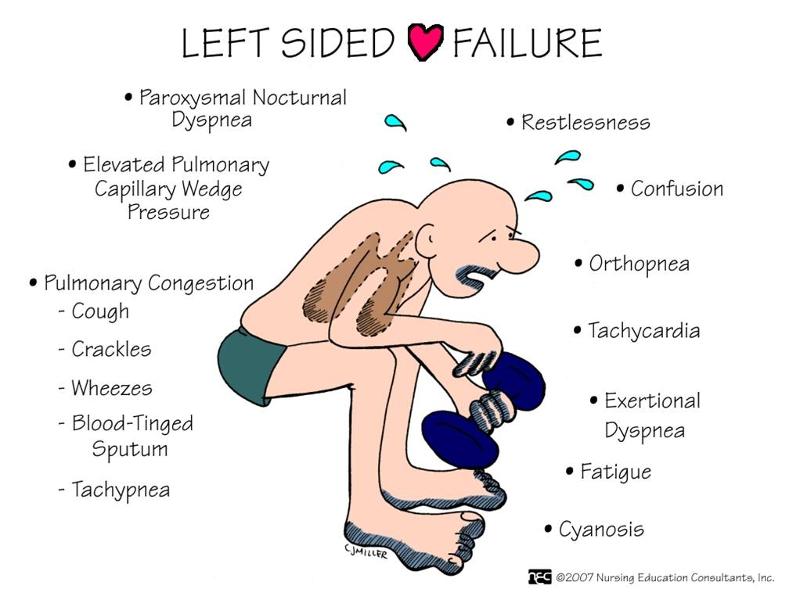
¨Left-sided failure
¤LV cannot pump blood effectively to the systemic circulation. Pulmonary venous pressures increase and result in pulmonary congestion with dyspnea, cough, crackles, and impaired oxygen exchange.
¨Chronic heart failure is frequently biventricular.
Clinical Manifestations
¨NYHA classification of heart failure
¤Classification I , II, III, IV
¨ACC/AHA classification of heart failure
¤Stages A, B, C, D
¨Treatment guidelines are in place for each stage
CLASSIFICATION OF HF
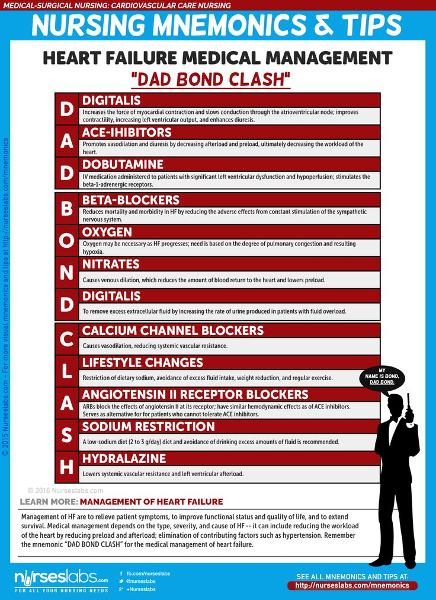
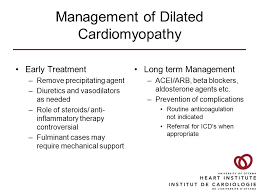
¨Eliminate or reduce etiologic or contributory factors.
¨Reduce the workload of the heart by reducing afterload and preload.
¨Optimize all therapeutic regimens.
¨Prevent exacerbations of heart failure.
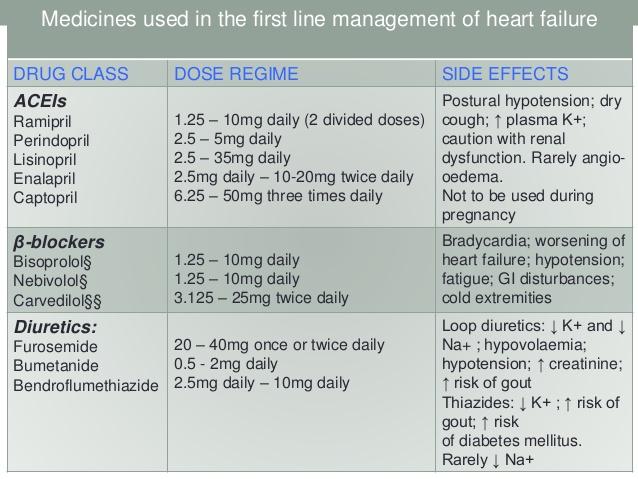
¨Medications are routinely prescribed for heart failure.
Medical Management of Heart Failure
¨Angiotensin: converting enzyme inhibitors
¨Angiotensin II receptor blockers
¨Beta-blockers
¨Diuretics
¨Digitalis (Digoxin): +inotropic: inhibiting NA K ATPase, accumulation of NA causes release of CA -chronotropic: suppress SA node and slow conduction through the AV node
¤Page 802 (Taylor) and Page 353 (Adams)
MEDICATIONS OF HF
¨Health history
¨Sleep and activity: paroxysmal nocturnal dysnpnea
¨Knowledge and coping
¨Physical exam
¤Mental status
¤Lung sounds: crackles and wheezes
¤Heart sounds: S3: volume entering the ventricles at the beginning of diastole
¤Fluid status/signs of fluid overload
nDaily weight and I&O
¨Assess responses to medications
¨
Nursing Process: The Care of the Patient with Heart Failure—Assessment
¨Activity intolerance and fatigue
¨Excess fluid volume
¨Anxiety
¨Powerlessness
¨Noncompliance
Nursing Process: The Care of the Patient with Heart Failure—Diagnoses
¨Cardiogenic shock
¨Dysrhythmias
¨Thromboembolism
¨Pericardial effusion and cardiac tamponade
¨
Collaborative Problems/Potential Complications
¨Goals may include promoting activity and reducing fatigue, relieving fluid overload symptoms, decreasing anxiety or increasing the patient’s ability to manage anxiety, encouraging the patient to make decisions and influence outcomes, teaching the patient about the self-care program.
Nursing Process: The Care of the Patient with Heart Failure—Planning
¨Bed rest for acute exacerbations
¨Encourage regular physical activity; 30–45 minutes daily
¨Exercise training
¨Pacing of activities
¨Wait 2 hours after eating for physical activity
¨Avoid activities in extreme hot, cold, or humid weather
¨Modify activities to conserve energy
¨Positioning; elevation of the HOB to facilitate breathing and rest, support of arms
ACTIVITY INTOLERANCE : HF
¨Assessment for symptoms of fluid overload
¨Daily weight
¨I&O
¨Diuretic therapy; timing of meds
¨Fluid intake; fluid restriction
¨Maintenance of sodium restriction
FLUID VOLUME EXCESS/ OVERLOAD
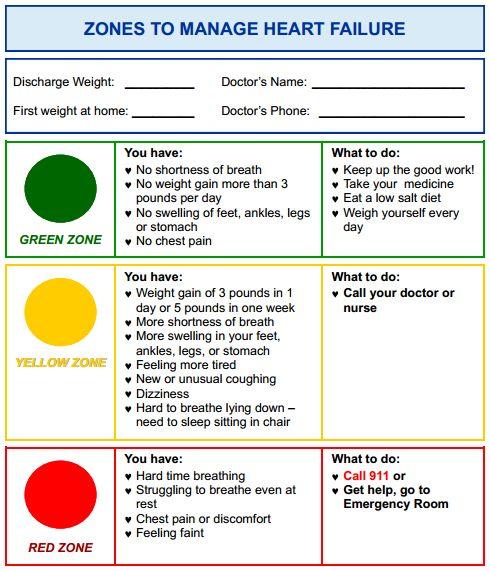
¨Medications
¨Diet: low-sodium diet and fluid restriction
¨Monitoring for signs of excess fluid, hypotension, and symptoms of disease exacerbation, including daily weight
¨Exercise and activity program
¨Stress management
¨Prevention of infection
¨Know how and when to contact health care provider
¨Include family in teaching
¨
PATIENT TEACHING : HF
¨Acute event in which the LV cannot handle an overload of blood volume. Pressure increases in the pulmonary vasculature, causing fluid movement out of the pulmonary capillaries and into the interstitial space of the lungs and alveoli.
¨Results in hypoxemia.
¨Clinical manifestations: restlessness, anxiety, dyspnea, cool and clammy skin, cyanosis, weak and rapid pulse, cough, lung congestion (moist, noisy respirations), increased sputum production (sputum may be frothy and blood-tinged), decreased level of consciousness.
PULMONARY EDEMA
¨Prevent
¨Early recognition: monitor lung sounds and for signs of decreased activity tolerance and increased fluid retention
¨Place patient upright and dangle legs
¨Minimize exertion and stress
¨Oxygen
¨Medications
¤Morphine
¤Diuretic: furosemide
MANAGEMENT OF PULMONARY EDEMA
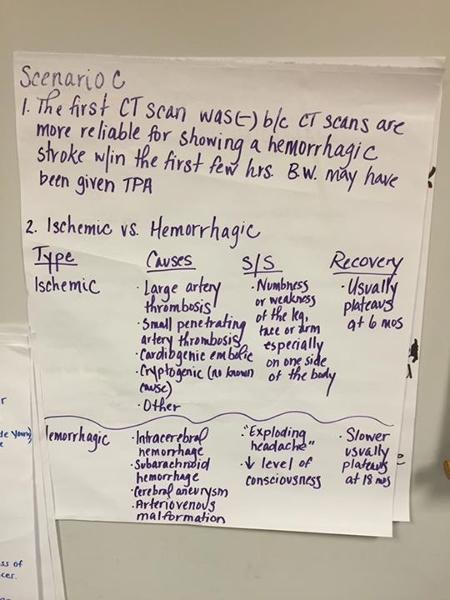
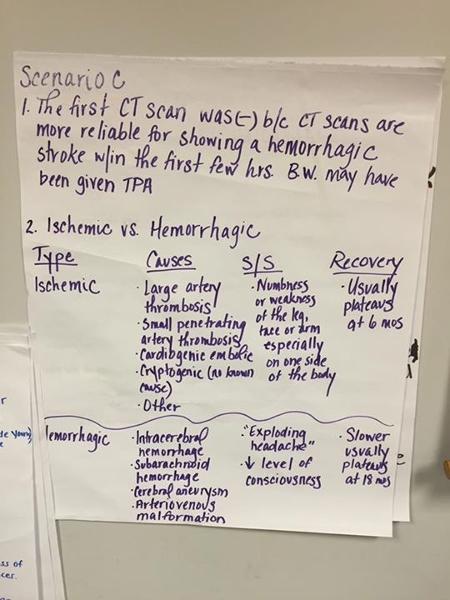
- Is the disruption of the supply of blood to a specific area in the brain.
- Secondary to ischemia, embolism or hemorrhage
- This may result in tissue necrosis and sudden loss of brain functions
- Atherosclerosis resulting in cerebrovascular disease
Cerebrovascular Accident
Anterior: Carotid Arteries – middle & anterior cerebral arteries
frontal, parietal, temporal lobes; basal ganglion; part of the diencephalon (thalamus & hypothalamus)
Posterior: Vertebral Arteries – basilar artery
Mid and lower temporary & occipital lobes, cerebellum, brainstem, & part of the diencephalon
Circle of Willis – connects the anterior & posterior cerebral circulation
Anatomy of Cerebral Circulation: Blood Supply
High blood pressure Diabetes Cigarette smoking TIA (Aspirin) High blood cholesterol Obesity Heart Disease Atrial fibrillation
Oral contraceptive use Physical inactivity
Sickle cell disease Asymptomatic carotid stenosis Hypercoagulability
Controllable Risks with Medical Treatment & Lifestyle Changes:
- Symptoms depend on the location and size of the affected area
- Numbness or weakness of face, arm, or leg, especially on one side
- Confusion or change in mental status
- Trouble speaking or understanding speech
- Difficulty in walking, dizziness, or loss of balance or coordination
- Sudden, severe headache
- Perceptual disturbances
Manifestations of Ischemic Stroke
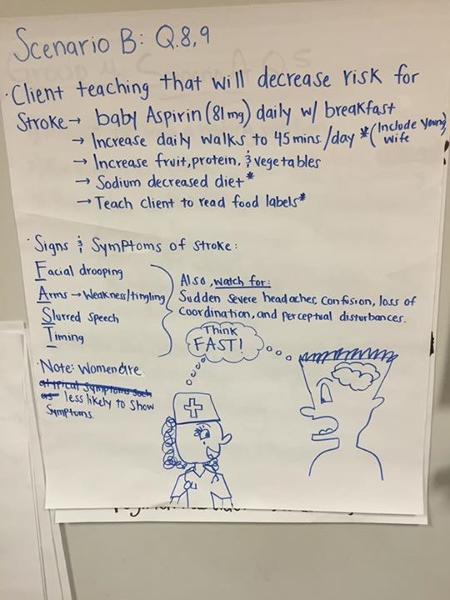
- F- Facial drooping
- A - Arms
- S- slurred speech
- T- timing
STROKE ALERT
- Done to confirm CVA and identify causes
- Neuro assessment, carotid bruit, carotid Doppler (PE)
- Ct scan
- CTA- CT with angiography
- Angiography –gold standard for imaging carotid arteries
- MRI
DIAGNOSTIC STUDIES - STROKE
- Health maintenance measures including a healthy diet, exercise, and the prevention and treatment of periodontal disease
- Carotid endarterectomy
- Anticoagulant therapy
- Antiplatelet therapy: aspirin, dipyridamole plus aspirin (Aggrenox), clopidogrel (Plavix)
- “Statins”
- Antihypertensive medications
Preventive Treatment and Secondary Prevention- STROKE
- Prompt diagnosis and treatment:
- Assessment of stroke: NIHSS assessment tool Table 67-1 pg. 1978
- Thrombolytic therapy
- Criteria for tPA: Brunner 1977 Chart 67-2
- IV dosage and administration
- Patient cardiac and neurological monitoring
- Side effects: potential bleeding
- Elevate head of bed (HOB) unless contraindicated
- Maintain airway and ventilation
Medical Management: Acute Phase of Stroke
- Acute phase
- Ongoing, frequent monitoring of all systems, including vital signs and neurologic assessment—LOC, motor symptoms, speech, eye symptoms
- Monitor for potential complications, including musculoskeletal problems, swallowing difficulties, respiratory problems, and signs and symptoms of increased ICP and meningeal irritation
- After the stroke is complete
- Focus on patient function; self-care ability, coping, and education regarding needs to facilitate rehabilitation
- Improved thought processes
- Achieving a form of communication
- Maintaining skin integrity
- Restored family functioning
- Improved sexual function
- Absence of complications
Nursing Process: The Patient Recovering From an Ischemic Stroke—Assessment
- Turn and position in correct alignment every 2 hours
- Use of splints
- Passive or active ROM four or five times day
- Positioning of hands and fingers
- Prevention of flexion contractures
- Prevention of shoulder abduction
- Do not lift by flaccid shoulder
- Measures to prevent and treat shoulder problems
Improving Mobility and Preventing Joint Deformities
- Encourage patient to exercise unaffected side
- Establish regular exercise routine
- Quadriceps setting and gluteal exercises
- Assist patient out of bed as soon as possible; assess and help patient achieve balance; move slowly
- Ambulation training
Improving Mobility and Preventing Joint Deformities
- Enhancing self-care
- Set realistic goals with the patient
- Encourage personal hygiene
- Ensure that patient does not neglect the affected side
- Use of assistive devices and modification of clothing
- Support and encouragement
- Strategies to enhance communication
- Encourage patient to turn head, look to side with visual field loss
- Nutrition
- Consult with speech therapy or nutritional services
- Have patient sit upright, preferably out of bed, to eat
- Chin tuck or swallowing method
- Use of thickened liquids or pureed diet
- Bowel and bladder control
- Assessment of voiding and scheduled voiding
- Measures to prevent constipation: fiber, fluid, toileting schedule
- Bowel and bladder retraining
NURSING INTERVENTIONS POSITIONING FROM STROKE
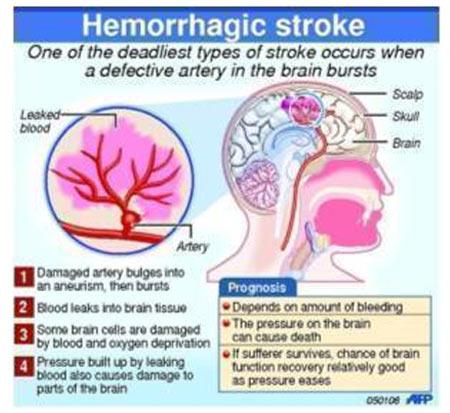
- Caused by bleeding into brain tissue, the ventricles, or subarachnoid space
- Brain metabolism is disrupted by exposure to blood.
- ICP increases caused by blood in the subarachnoid space.
- Compression or secondary ischemia from reduced perfusion and vasoconstriction causes injury to brain tissue
HEMMORAGIC STROKE
- Similar to ischemic stroke
- Severe headache
- Early and sudden changes in LOC
- Possible focal seizures
- Vomiting
- (due to brain stem involvement)
MANIFESTATIONS OF HEMMORGIC STROKE
- Prevention: control of Hypertension
- Diagnosis: CT scan, cerebral angiography, lumbar puncture if CT is negative and ICP is not elevated to confirm subarachnoid hemorrhage
- Care is primarily supportive
- Bed rest with sedation
- Oxygen
- Treatment of vasospasm, increased ICP, hypertension, potential seizures, and prevention of further bleeding
Medical Management HEMMORAGIC STROKE
- Complete and ongoing neurologic assessment; use neurologic flow chart
- Monitor respiratory status and oxygenation
- Monitoring of ICP
- Patients with intracerebral or subarachnoid hemorrhage should be monitored in the ICU
- Monitor for potential complications
- Monitor fluid balance and laboratory data
- All changes must be reported immediately
Nursing Process: The Patient With a Hemorrhagic Stroke—Assessment
- Vasospasm
- Seizures
- Hydrocephalus
- Rebleeding
- Hyponatremia
Collaborative Problems and Potential Complications- HEMORRHAGIC STROKE
- Goals may include:
- Improved cerebral tissue perfusion
- Relief of sensory and perceptual deprivation
- Relief of anxiety
- The absence of complications
Nursing Process: The Patient With a Hemorrhagic Stroke—Planning
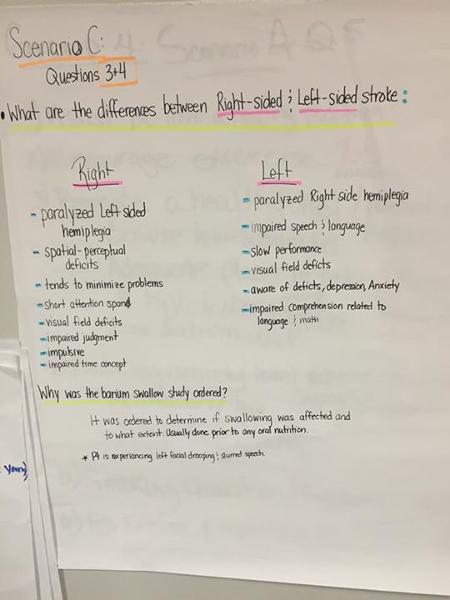
- Hemiplegia
- Hemiparesis
- Dysarthria
- Aphasia: expressive aphasia, receptive aphasia
- Hemianopsia
...
- Prevention of and signs and symptoms of complications
- Medication education
- Safety measures
- Adaptive strategies and use of assistive devices for ADLs
- Nutrition: diet, swallowing techniques, tube feeding administration
- Elimination: bowel and bladder programs, catheter use
- Exercise and activities, recreation and diversion
- Socialization, support groups, and community resources
Home Care and Education for the Patient Recovering from a Stroke
Cerebrovascular Accident Clinical Manifestations Right Brain – Left Brain Damage
...
What are expected patient outcomes for a patient recovering from a hemorrhagic stroke?
- Exhibits absence of vasospasm
- Residual aphasia
- One to four seizures
- Complains of visual changes
A.Exhibits absence of vasospasm
Expected patient outcomes for a patient recovering from a hemorrhagic stroke include absence of vasospasm, no seizures, normal speech patterns, and no visual changes.
What intervention would not be included in aspiration precautions for a patient in the acute phase of a stroke?
A.Referral to speech therapy
B.Have patient tuck their chin toward the chest when swallowing
C.Thickened fluids or pureed diet
D.Raise HOB to 30 degrees when feeding
D.Raise HOB to 30 degrees when feeding
Interventions to prevent aspiration include a referral to speech therapy for swallowing evaluation; having the patient tuck the chin toward the chest when swallowing to close off the trachea, preventing aspiration into the lungs; providing thickened fluids or a pureed diet; and sitting the patient at a full upright position (90 degrees) when feeding or providing fluids. The patient’s HOB should be elevated to 30 degrees at all times to prevent aspiration of secretions but would not prevent aspiration of food or fluids when feeding
A patient with right-sided paresthesias and hemiparesis is hospitalized and diagnosed with a thrombotic stroke. Over the next 72 hours, the nurse plans care with the knowledge that the patient:
- Is ready for aggressive rehabilitation.
- Will show gradual improvement of the initial neurologic deficits.
- May show signs of deteriorating neurologic function as cerebral edema increases.
- Should not be turned or exercised to prevent extension of the thrombus and increased neurologic deficits.
...
While performing health screening at a health fair, the nurse identifies which of the following individuals at greatest risk for experiencing a stroke?
- A 46-year-old white female with hypertension and oral contraceptive use for 10 years.
- A 58-year-old white male salesman who has a total cholesterol level of 285 mg/dL.
- A 42-year-old African American female with diabetes mellitus who has smoked for 30 years.
- A 62-year-old African American male with hypertension who is 35 pounds overweight.
...
What is agnosia?
- Failure to recognize familiar objects perceived by the senses
- Inability to express oneself or to understand language
- Inability to perform previously learned purposeful motor acts on a voluntary basis
- Impaired ability to coordinate movement, often seen as a staggering gait or postural imbalance
A.Failure to recognize familiar objects perceived by the senses
Agnosia is failure to recognize familiar objects perceived by the senses. Aphasia is an inability to express oneself or to understand language. Apraxia is an inability to perform previously learned purposeful motor acts on a voluntary basis. Ataxia is an impaired ability to coordinate movement, often seen as a staggering gait or postural imbalance.
1 Describe the pathophysiology, clinical manifestations, and treatment of coronary atherosclerosis
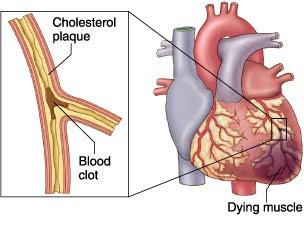
Pathophysiology: What is Atherosclerosis?
A disease in which plaque builds up inside your arteries
Pathophysiology: What is Plaque?
Plaque is a sticky substance made up of fat, cholesterol, calcium, and other substances found in the blood.
Pathophysiology: What happens when plaque hardens and narrows in your arteries?
It limits the flow of oxygen-rich blood to your body.
Pathophysiology: What can Atherosclerosis lead to?
It can lead to Coronary Artery Disease, Carotid Artery Disease, and Peripheral Arterial Disease.
Pathophysiology: Advanced with again, what can Atherosclerosis do?
It can cause critical narrowing of the arteries resulting in tissue ischemia (lack of blood and oxygen).
Epidemiology: When does Atherosclerosis begin?
Begins in childhood with the development of fatty streaks
Epidemiology: As these individuals age, there is an increased incidence of advanced complicated lesions which leads to...?
the organ-specific clinical manifestations of the disease.
Epidemiology: What are the primary risk fators of Atherosclerosis?
o Cigarette smoking o High blood pressure o Elevated serum cholesterol (total and LDL) o Advancing age o Diabetes mellitus
Epidemiology: What are the secondary risk factors of Atherosclerosis?
o Obesity o Psychosocial factors o Physical inactivity o Family history of early CAD o Ethnic characteristics
Symptoms: Many people don't have Atherosclerosis until they have these two medical emergencies...?
Heart attack or strokes
Symptoms: The type of symptoms depends on what?
Location of blocked artery
Symptoms: What are Atherosclerosis symptoms in Carotid Arteries?
o Sudden weakness o Confusion o Problems breathing o Dizziness o Sudden and severe headache
Symptoms: What are Atherosclerosis symptoms in Peripheral Arteries?
Numbness o Pain o Dangerous infection
Symptoms: What a
2 Describe the pathophysiology, clinical manifestations, and treatment of angina pectoris.
Pathophysiology
Angina is usually caused by atherosclerotic disease. Almost invariably, angina is associated with a significant obstruction of at least one major coronary artery. Normally, the myocardium extracts a large amount of oxygen from the coronary circulation to meet its continuous demands. When demand increases, flow through the coronary arteries needs to be increased. When there is blockage in a coronary artery, flow cannot be increased and ischemia results. The types of angina are listed in Several factors are associated with typical anginal pain:
- Physical exertion, which precipitates an attack by increasing myocardial oxygen demand
- Exposure to cold, which causes vasoconstriction and elevated blood pressure, with increased oxygen demand
- Eating a heavy meal, which increases the blood flow to the mesenteric area for digestion, thereby reducing the blood supply available to the heart muscle; in a severely compromised heart, shunting of blood for digestion can be sufficient to induce anginal pain
- Stress or any emotion-provoking situation, causing the release of catecholamines, which increases blood pressure, heart rate, and myocardial workload
Unstable angina is not closely associated with these listed factors. It may occur at rest. See the later discussion of unstable angina in Acute Coronary Syndrome and Myocardial Infarction section.
Clinical Manifestations
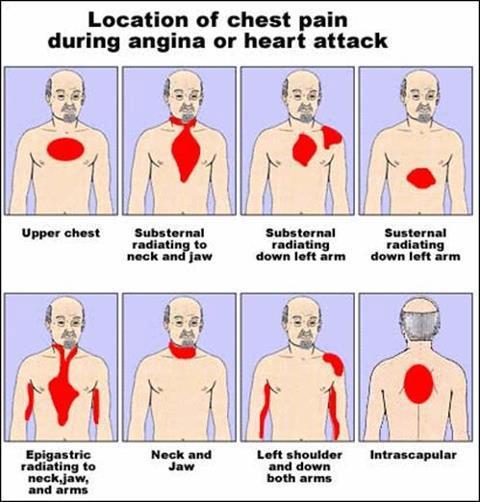
Ischemia of the heart muscle may produce pain or other symptoms, varying from mild indigestion to a choking or heavy sensation in the upper chest. The severity ranges from discomfort to agonizing pain. The pain may be accompanied by severe apprehension and a feeling of impending death. It is often felt deep in the chest behind the sternum (retrosternal area). Typically, the pain or discomfort is poorly localized and may radiate to the neck, jaw, shoulders, and inner aspects of the upper arms, usually the left arm. The patient often feels tightness or a heavy choking or strangling sensation that has a viselike, insistent quality.
The patient with diabetes may not have severe pain with angina because diabetic neuropathy can blunt nociceptor transmission, dulling the perception of pain. Women may have differe
3 Use the nursing process as a framework for care of clients with angina pectoris.
https://quizlet.com/25072853/nurs-432-ch-40-flash-cards/
Goal: pain is reduced / resolved. Outcomes: Patient states / shows the pain is relieved, Patient reported angina episodes decreased in frequency, duration and severity. Interventions: 1. Instruct the patient to notify nurse quickly in the event of chest pain. Rationale: Pain and decreased cardiac output can stimulate the sympathetic nervous system to release large amounts of nor epinephrine, which increases platelet aggregation and thromboxane A2 issued. Pain cannot be detained cause vasovagal response, reducing BP and heart rate. 2. Identification of the precipitating factors, if any: frequency, duration, intensity and location of pain. Rationale: Helps distinguish chest pain early and the possibility of progress evaluation tool becomes unstable angina (stable angina usually ends 3 to 5 minutes while unstable angina longer and can last more than 45 minutes. 3. Evaluation report pain in the jaw, neck, shoulder, hand or arm (especially on the left side). Rationale: cardiac pain may spread to the sample surface pain more often innervated by the same spinal level. 4. Instruct the patient on bed rest during episodes of angina. Rationale: Reduce myocardial oxygen demand to minimize the risk of tissue injury or necrosis. 5. Elevate the head of the bed when the patient is short of breath. Rationale: Facilitate the exchange of gases to reduce repetitive hypoxia and shortness of breath. 6. Monitor the speed or rhythm of the heart. Rationale: Patients with unstable angina have increased life-threatening dysrhythmias in acute, which occurs in response to ischemia and or stress. 7. Monitor vital signs every 5 minutes during an attack of angina. Rational: BP can rise early with respect to sympathetic stimulation, then dropped when the cardiac output is affected. 8. Maintain a calm, comfortable environment, limit the visitor when necessary. Rationale: mental or emotional stress increase myocardial work. 9. Give soft foods. Let the patient rest for 1 hour after eating. Rationale: Reduces myocardial work in connection with the work of digestion, manurunkan risk of angina attacks 10. Give antianginal as indicated. Rationale: For the treatment and prevent angina pain.
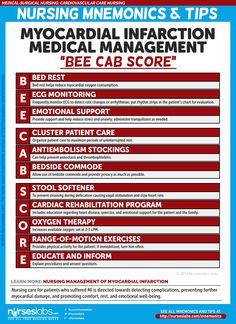
4 Describe the pathophysiology, clinical manifestations, and treatment of myocardial infarction.
What is myocardial infarction?
Treatment Guidelines for Acute Myocardial Infarction
- Use rapid transit to the hospital.
- Obtain 12-lead electrocardiogram to be read within 10 minutes.
- Obtain laboratory blood specimens of cardiac biomarkers, including troponin.
- Obtain other diagnostics to clarify the diagnosis.
- Begin routine medical interventions:
- Supplemental oxygen
- Nitroglycerin
- Morphine
- Aspirin 162–325 mg
- Beta-blocker
- Angiotensin-converting enzyme inhibitor within 24 hours
- Anticoagulation with heparin and platelet inhibitors
- Evaluate for indications for reperfusion therapy:
- Percutaneous coronary intervention
- Thrombolytic (fibrinolytic) therapy
- Continue therapy as indicated:
- IV heparin, low-molecular-weight heparin, bivalirudin, or fondaparinux
- Clopidogrel (Plavix)
- Glycoprotein IIb/IIIa inhibitor
- Bed rest for a minimum of 12–24 hours
Acute Myocardial Infarction Core Measure Set
- Aspirin administered upon arrival to the hospital
- Aspirin prescribed at discharge from the hospital
- ACE inhibitor or ARB prescribed for patients with concomitant left ventricular systolic dysfunction
- Adult smoking cessation advice/counseling as needed
- Beta-blocker prescribed at discharge from the hospital
- Thrombolytic (fibrinolytic) therapy received within 30 minutes of hospital arrival
- PCI received within 90 minutes of hospital arrival
- Statin prescribed at discharge
When coronary blood flow is interrupted for a period of time, death of the myocardium occurs.
What are the causes of M.I.?
Atherosclerosis, and coronary vasospasm
How does atherosclerosis cause M.I.?
Plaque is disrupted and thrombus formation leads to acute decrease in coronary blood flow.
What causes a plaque to rupture?
Shear forces, inflammation, apoptosis, macrophage-derived degradative enzymes.
What causes blood clot formation over lesion?
5 Use the nursing process as a framework for care of a clients with acute coronary syndrome.
https://quizlet.com/99890304/nursing-management-coronary-artery-disease-and-acute-coronary-syndrome-flash-cards/
http://www.coursewareobjects.com/objects/evolve/E2/book_pages/lewismedsurg/pdfs/nursing_care_plans.pdf
6 Use the nursing process as a framework for care of a clients who has undergone cardiac surgery.
Pathophysiology a. The disorder is characterized by a narrowing of coronary arteries due to atherosclerosis, spasm or, rarely, embolism. b. Atherosclerotic changes in coronary arteries results in damage to the inner layers of the coronary arteries with stiffening of vessels and diminished dilatory response. c. Accumulation of fatty deposits and lipids, along with development of fibrous plaques over the damaged areas in the vessels, causes narrowing of the arteries, thus reducing the size of the vessel’s lumen and impeding blood flow to the myocardial tissues. d. Decreased delivery of oxygen and nutrients to the tissues causes transient myocardial ischemia and pain. e. Hard plaque causes hardened arteries, whereas soft plaque can cause formation of blood clots. II. Types b. Unstable i. May be new onset of pain with exertion or at rest, or recent acceleration in severity of pain ii. Occurs in no regular pattern, usually lasts longer (30 minutes), not generally relieved with rest or medications iii. Sometimes grouped with myocardial infarction (MI) under the diagnosis of acute coronary syndrome (ACS)c. Variant (Prinzmetal’s) i. Rare, usually occurs at rest—midnight to early morning hours ii. Pain possibly severe iii. Electrocardiogram (ECG) changes due to coronary artery spasmIV. Etiology Discharge Goals 1. Desired activity level achieved, with return to activity baseline, and self-care needs met with minimal or no pain. 2. remains free of complications. 3. Disease process, prognosis, and therapeutic regimen understood. 4. Participates in treatment program and behavioral changes. 5. Plan in place to meet needs after discharge. NURSING DIAGNOSIS: acute Pain May be related to Increased cardiac workload and oxygen consumption Decreased myocardial blood flow, tissue ischemia Possibly evidenced by Reports of pain varying in frequency, duration, and intensity, especially as condition worsens Narrowed focus Distraction behaviors, such as moaning, crying, pacing, or restlessness Autonomic responses, such as diaphoresis, BP and pulse rate changes, pupillary dilation, increased or decreased respiratory rate Desired Outcomes/Evaluation Criteria—Client Will Pain Level Report anginal episodes decreased in frequency, duration, and severity. Demonstrate relief of pain as evid
7.Describe the management of patients with heart failure.
- Congestive Heart Failure or CHF is a severe circulatory congestion due to decreased myocardial contractility, which results in the heart’s inability to pump sufficient blood to meet the body’s needs.
- About 80% of CHF cases occur before 1 year of age
Etiology
- The primary cause of CHF in the first 3 years of life is CHD.
- Other causes in children include:
- Other myocardial disorders, such as cardiomyopathies, arrhythmias, and hypertension
- Pulmonary embolism or chronic lung disease
- Severe hemorrhage or anemia
- Adverse effects of anesthesia or surgery
- Adverse effects of transfusions or infusions
- Increased body demands resulting from conditions such as fever, infection and arteriovenous fistula
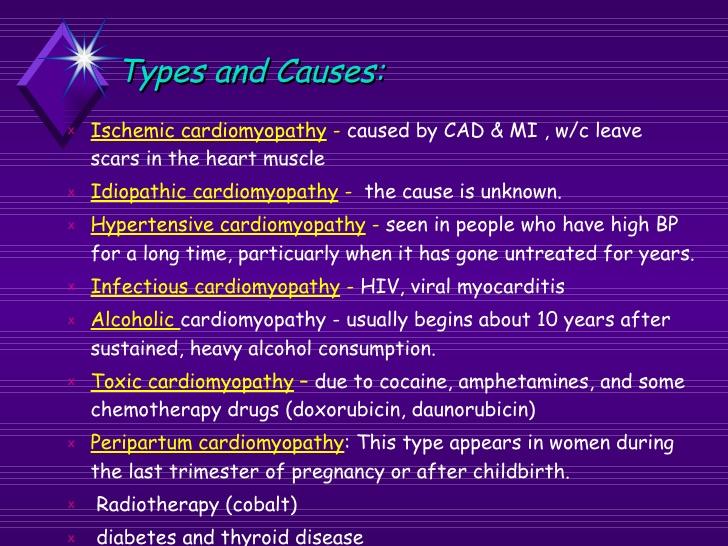
- Adverse effects of drugs, such as doxorubicin
- Severe physical or emotional stress
- Excessive sodium intake
- In general,
causes can be classified according to the following:
- Volume overload may cause the right ventricle to hypertrophy to compensate for added volume.
- Pressure overload usually results from an obstructive lesion, such as COA
- Decrease contractility can result from problems such as severe anemia, asphyxia, heart block and acidemia.
- High cardiac output demands occur when the body’s need for oxygen exceeds the heart’s output seen in sepsis and hyperthyroidism.
- Pathophysiology
- Right ventricular failure occurs when the right ventricle is unable to pump blood into the pulmonary circulation. Less blood is oxygenated and pressure increases in the right atrium and systemic venous circulation, which results in edema of the extremities.
- Left ventricular failure occurs when the left ventricle in unable to pump blood into systemic circulation. Pressure increases in the left atrium and pulmonary veins; then the lungs become congested with blood, causing elevated pulmonary pressure and pulmonary edema.
- To compensate, the cardiac muscle hypertrophies eventually resulting in decreased ventricular compliance. Decreased compliance requires higher filling pressure to produce the same stroke volume. Increased mu
8.Use the nursing process as a framework for care of patients with heart failure.
Nursing Intervention
- Monitor for signs of respiratory distress
- Provide pulmonary hygiene as needed
- Administer oxygen as prescribed
- Keep the head of the bed elevated
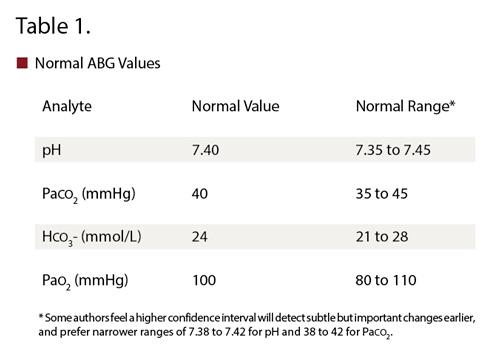
- Monitor ABG values.
- Monitor for signs of
altered cardiac output, including
- Pulmonary edema
- Arrhythmias, including extreme tachycardia and bradycardia
- Characteristic ECG and heart sound changes
- Evaluate fluid status
- Maintain strict fluid intake and output measurements
- Monitor daily weights
- Assess for edema and severe diaphoresis
- Monitor electrolyte values and hematocrit level
- Maintain strict fluid restrictions as prescribed
- Administer prescribed medications
which may include:
- Antiarrhythmias to increase cardiac performance
- Diuretics, to reduce venous and systemic congestion
- Iron and folic acid supplements to improve nutritional status.
- Prevent Infection
- Reduce cardiac demands
- Keep the child warm
- Schedule nursing interventions to allow for rest
- Do not allow an infant to feed for more than 45 minutes at a time
- Provide gavage feedings if the infant becomes fatigued before ingesting an adequate amount
- Promote adequate nutrition. Maintain a high-calorie, low-sodium as prescribed.
- Promote optimal growth and development
- As appropriate, refer the family to a community health nurse for follow up care after discharge.
- Documentation Guidelines
- Physical findings indicative of HF: Mental confusion ,pale, cyanotic ,clammy skin, presence of jugular vein distension and HJR, ascites, edema, pulmonary crackles or wheezes, adventitious heart sounds
- Fluid intake and output, daily weights
- Response to medications such as diuretics, nitrates ,dopamine, dobutamine, and oxygen
- Psychosocial response to illness
Discharge and Home Healthcare Guidelines
- PREVENTION. To prevent exacerbations, teach the patient and family to monitor for an increase in shortness of breath or edema. Tell
The Pathway of Blood to and from the Heart
- Blood that has circulated through the body, which has lost its oxygen and collected carbon dioxide, enters through the vena cava into the right atrium of the heart.
- The right atrium contracts and pumps the blood through the tricuspid valve and into the right ventricle.
- The right ventricle then pumps blood through the pulmonary artery into the lungs.
- In the lungs, tiny blood vessels called capillaries absorb carbon dioxide from the blood and replace it with oxygen.
- Oxygenated blood then flows through the pulmonary vein and into the left atrium.
- Oxygenated blood then pumps through the mitral valve and into the left ventricle.
- The left side of the heart contracts the strongest to send blood out the left ventricle and through the aortic arch on its way to all parts of the body. At this point, there are a few options for the blood flow: blood can be pumped • through the carotid artery and into the brain. • Through the auxiliary arteries and into the arms. • Through the aorta and into the torso and legs.
- Blood will then move through the arteries, then through capillaries, and then return through the veins.
- Deoxygenated blood (blood without oxygen) will then return to the heart.
- The cycle repeats.
HF TERMINOLOGY
acute coronary syndrome (ACS): signs and symptoms that indicate unstable angina or acute myocardial infarction
angina pectoris: chest pain brought about by myocardial ischemia
atheroma: fibrous cap composed of smooth muscle cells that forms over lipid deposits within arterial vessels and protrudes into the lumen of the vessel, narrowing the lumen and obstructing blood flow; also called plaque
Atherosclerosis: abnormal accumulation of lipid deposits and fibrous tissue within arterial walls and the lumen
Contractility: ability of the cardiac muscle to shorten in response to an electrical impulse
coronary artery bypass graft (CABG): a surgical procedure in which a blood vessel from another part of the body is grafted onto the occluded coronary artery below the occlusion in such a way that blood flow bypasses the blockage
high-density lipoprotein (HDL): a protein-bound lipid that transports cholesterol to the liver for excretion in the bile; composed of a higher proportion of protein to lipid than low-density lipoprotein; exerts a beneficial effect on the arterial wall
ischemia: insufficient tissue oxygenation
low-density lipoprotein (LDL): a protein-bound lipid that transports cholesterol to tissues in the body; composed of a lower proportion of protein to lipid than high-density lipoprotein; exerts a harmful effect on the arterial wall
metabolic syndrome: a cluster of metabolic abnormalities including insulin resistance, obesity, dyslipidemia, and hypertension that increase the risk of cardiovascular disease
myocardial infarction (MI): death of heart tissue caused by lack of oxygenated blood flow
percutaneous coronary intervention (PCI): a procedure in which a catheter is placed in a coronary artery, and one of several methods is employed to reduce blockage within the artery
percutaneous transluminal coronary angioplasty (PTCA): a type of percutaneous coronary intervention in which a balloon is inflated within a coronary artery to break an atheroma and open the vessel lumen, improving coronary artery blood flow
stent: a metal mesh that provides structural support to a coronary vessel, preventing its closure
sudden cardiac death: abrupt cessation of effective heart activity
thrombolytic: a pharmacologic agent that breaks dow
A client with known coronary artery disease reports intermittent chest pain, usually on exertion. The physician diagnoses angina pectoris and orders sublingual nitroglycerin to treat acute angina episodes. When teaching the client about nitroglycerin administration, which instruction should the nurse provide?
"Be sure to take safety precautions because nitroglycerin may cause dizziness when you stand up."
Nitroglycerin commonly causes orthostatic hypotension and dizziness. To minimize these problems, the nurse should teach the client to take safety precautions, such as changing to an upright position slowly, climbing up and down stairs carefully, and lying down at the first sign of dizziness. To ensure the freshness of sublingual nitroglycerin, the client should replace tablets every 6 months, not every 9 months, and store them in a tightly closed container in a cool, dark place. Many brands of sublingual nitroglycerin no longer produce a burning sensation. The client should take a sublingual nitroglycerin tablet at the first sign of angina. He may repeat the dose every 5 minutes for up to three doses; if this intervention doesn't bring relief, the client should seek immediate medical attention.
Hinkle, J.L., and Cheever, K.H. Brunner & Suddarth's Textbook of Medical-Surgical Nursing, 13th ed. Philadelphia: Lippincott Williams & Wilkins, 2014, Chapter 27: Management of Patients With Coronary Vascular Disorders, p. 738.
The nurse, caring for a patient after cardiac surgery, is aware that fluid and electrolyte imbalance is a concern. Select the most immediate result that needs to be reported.
Potassium level of 6 mEq/L
Changes in serum electrolytes should be immediately reported, especially a potassium level of 6 mEq/L. An elevated blood sugar is common postoperatively, and the weight gain isn't significant. The abnormal breath sounds are of concern, but the electrolyte imbalance is the most immediate condition that needs to be addressed.
Hinkle, J.L., and Cheever, K.H. Brunner & Suddarth's Textbook of Medical-Surgical Nursing, 13th ed. Philadelphia: Lippincott Williams & Wilkins, 2014, Chapter 27: Management of Patients With Coronary Vascular Disorders, pp. 761-2, Chart 27-13.
When the nurse notes that the post cardiac surgery patient demonstrates low urine output (< 25 mL/hr) with high specific gravity (> 1.025), the nurse suspects
Inadequate fluid volume
Urine output of less than 25 mL/hr may indicate a decrease in cardiac output. A high specific gravity indicates increased concentration of solutes in the urine, which occurs with inadequate fluid volume. Indices of normal glomerular filtration are output of 25 mL or greater per hour and specific gravity between 1.010 and 1.025. Overhydration is manifested by high urine output with low specific gravity. The anuric patient does not produce urine.
Hinkle, J.L., and Cheever, K.H. Brunner & Suddarth's Textbook of Medical-Surgical Nursing, 13th ed. Philadelphia: Lippincott Williams & Wilkins, 2014, Chapter 27: Management of Patients With Coronary Vascular Disorders, p. 764.
The nurse is educating a patient diagnosed with angina pectoris about the difference between the pain of angina and a myocardial infarction (MI). How should the nurse describe the pain experienced during an MI? (Select all that apply.)
• It is substernal in location. • It is sudden in onset and prolonged in duration. • It is viselike and radiates to the shoulders and arms.
Chest pain that occurs suddenly, continues despite rest and medication, is substernal, and is sometimes viselike and radiating to the shoulders and arms is associated with an MI. Angina pectoris pain is generally relieved by rest and nitroglycerin.
Hinkle, J.L., and Cheever, K.H. Brunner & Suddarth's Textbook of Medical-Surgical Nursing, 13th ed. Philadelphia: Lippincott Williams & Wilkins, 2014, Chapter 27: Management of Patients With Coronary Vascular Disorders, p. 742.
Chapter 27: Management of Patients With Coronary Vascular Disorders - Page 742
A client has a blockage in the proximal portion of a coronary artery. After learning about treatment options, the client decides to undergo percutaneous transluminal coronary angioplasty (PTCA). During this procedure, the nurse expects to administer an:
anticoagulant.
...