carotid sheath and contents
fascia in the neck (either side of the trachea and esophagus) that contains:
- common carotid artery
- internal carotid artery
- internal jugular vein
- vagus nerve
carotid sinus
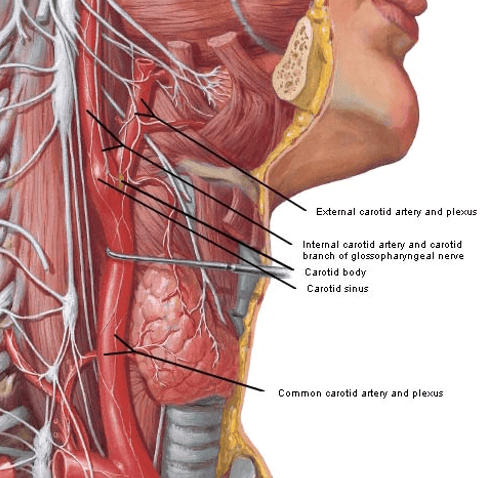
- located in the proximal part of the bifurcation of the common carotid
- collection of nerve endings from the glossopharyngeal nerve (IX)
-
functions as a
baroreceptor mechanism
- controls blood flow to brain thereby regulating intracranial pressure
carotid body
- located in the wall of the common carotid just before it divides into the internal and external carotid
-
functions as a
chemoreceptor through cranial nerves IX and X
- senses O2 and CO2 levels in the blood and regulates respirations accordingly
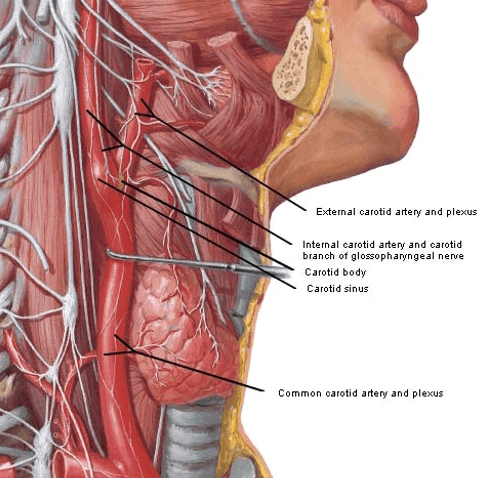
anterior triangle and its subdivisions
Anterior triangle Borders:
- superior: inferior border of the mandible
- laterally: medial border of the sternocleidomastoid
- medial: imaginary sagittal line down midline of neck
Carotid triangle
- Superior: Posterior belly of the digastric muscle
- Lateral: Medial border of the sternocleidomastoid muscle
- Inferior: Superior belly of the omohyoid muscle
- Contents:
- common carotid artery (which splits in the triangle into the external and internal carotid arteries)
- internal jugular vein
- hypoglossal and vagus nerves
Muscular Triangle
- Superiorly: The hyoid bone.
- Medially: Imaginary midline of the neck.
- Supero-laterally: Superior belly of the omohyoid muscle.
- Infero-laterally: Inferior portion of the sternocleidomastoid muscle
-
contents: no vessels
- infrahyoid muscles
- pharynx
- thyroid and parathyroid glands
Submental Triangle
- Inferiorly – Hyoid bone.
- Medially – Imaginary sagittal midline of the neck.
- Laterally – Anterior belly of the digastric
- contents: submental lymph nodes
- formed by mylohyoid muscle
Submandibular Triangle
- Superiorly: Body of the mandible.
- Anteriorly: Anterior belly of the digastric muscle.
- Posteriorly: Posterior belly of the digastric muscle.
-
contents:
- mandibular gland and lymph nodes
cervical plexus
- ventral primary rami of C1-C4 spinal nerves and their branches
- all these VPR receive gray rami communicans from the
superior cervical ganglion
- distribute sympathetic innervation through their branches
- located in the neck
- superficial (cutaneous) and deep (medial and lateral branches= muscular) branches
superficial nerves of cervical plexus
all cutaneous nerves
- lesser occipital nerve
- great auricular nerve
- transverse cervical nerve
- supraclavicular nerves
deep branches of cervical plexus
- Medial series
- Communicating branches to X and XII
- Muscular branches to rectus capitis lateralis, rectus capitis anterior, longus capitis and longus colli
- Inferior root of ansa cervicalis
- Phrenic nerve
- Lateral series
- communicating branches to XI
cervical dorsal primary rami
supply deep posterior and cervical muscles and skin on posterior head and neck
-
DPR of C1= suboccipital nerve
- enters suboccipital triangle
- carries motor fibers to supply the 4 suboccipital muscles and part of the semi-spinalis capitis
-
DPR of C2
- medial branch:
forms greater occipital nerve
- supplies muscular branches to semispinalis capitis, and skin of the posterior scalp
- lateral branch: muscular to splenius capitis, longissimus capitis, and semispinalis capitis
- medial branch:
forms greater occipital nerve
-
C3-C8 DPR
- medial and lateral branches supply the skin of posterior neck and deep muscles of the neck and upper back
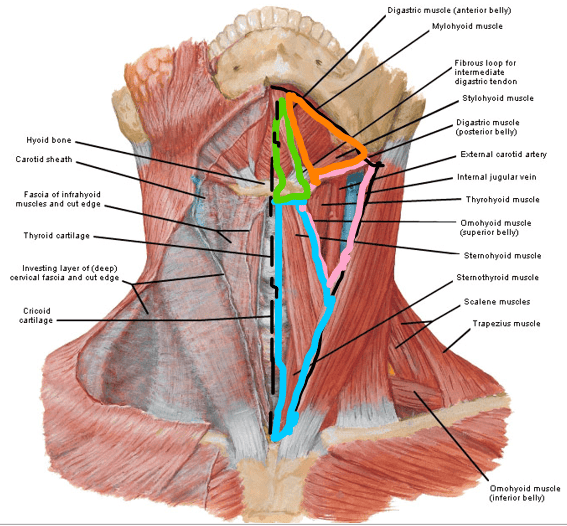
suboccipital triangle
- located in upper cervical region, deep to semispinalis capitis
-
borders:
- medial: rectus capitis posterior major
- inferior: obliquus capitis inferior
- lateral: obliquus capitis superior
-
contents:
- suboccipital nerve (C1 DPR)
- vertebral artery
- no bony protection here, so its vulnerable to injury
- posterior arch of the atlas (C1)
muscles of mastication
all innervated by the mandibular division of the trigeminal nerve
temporalis
lateral pterygoid
medial pterygoid
masseter
TMJ capsule and lateral ligaments
thin, synovial capsule
ligaments reinforce capsule and have sensory role in position and movement (proprioreception)
-
lateral temporo-mandibular
ligament: prevents excessive A-P and lateral
movements
- main suspension ligament during moderate opening
- Sphenomandibular ligament: suspends mandible during wide opening (medial lig)
- Stylomandibular ligament: acts as a stop to extreme opening (medial lig)
TMJ Articular Disc (Meniscus)
- fibrocartilaginous, avascular, aneural
- shock absorber,
improves congruency of joint surfaces, improves stability
- controls posterior movements during mouth closing
- attached to capsule anteriorly and through bilaminar
zone posteriorly
- attaches anteriorly to the superior belly of the lateral pterygoid
- inserts medially and laterally into poles of the condyle via medial and lateral collateral ligaments
bilaminar zone (retro-discal tissue) in TMJ
attaches to posterior capsule and the anterior tympanic plate (anterior part of external acoustic meatus)
keeps articular disc from moving too far anteriorly
upper and lower compartments of TMJ
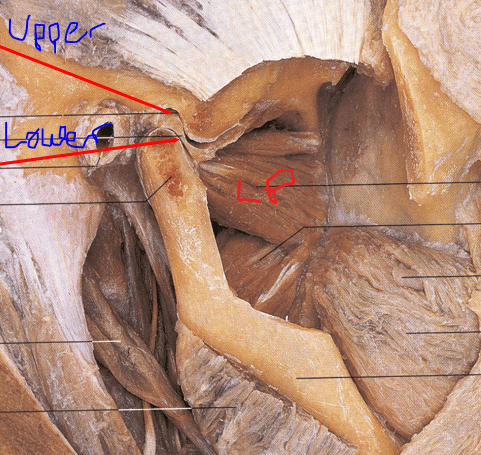
- Upper compartment: between disc and mandibular fossa & articular eminence
- Lower compartment: between disc and mandibular condyle
- Compartments play different kinematic roles during opening and closing of mouth
mouth opening and closing (depression and elevation)
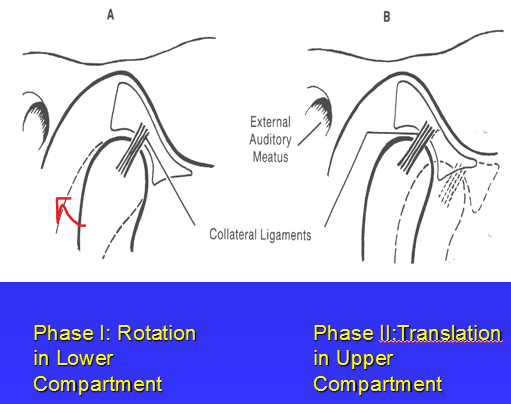
- coronal axis: passes through the condyles
-
Phase I: rotation of condyle on disk in lower
compartment
- First 11 – 25 mm.
- Phase II: translation of disc/condyle together in upper compartment
- Total excursion = 40 to 50 mm
- Closing or elevation occurs in reverse pattern as opening
TMJ dysfunction
Internal Derangement
- Meniscus is anteriorly displaced in front of condyle
Anterior Displacement with Reduction
- During opening, meniscus translates anteriorly & bilaminar zone is stretched
- At a certain point, meniscus will return to its normal position
- Pop or click may occur with reduction
Anterior Displacement without Reduction
- Meniscus remains anteriorly displaced with full opening
- Typically results in limited opening
mandibular protrusion and retrusion
Both are translational movements that occur in the upper compartment
Protrusion: mandible juts forward, range is about 6-9 mm
Retrusion: mandible pulls back, range is about 3 mm (past normal position)
Mandibular Lateral Deviation
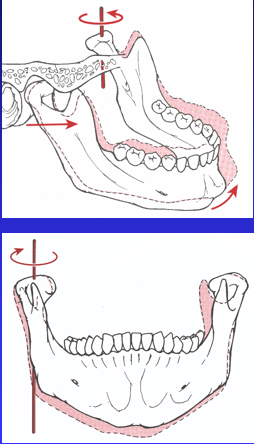
- Vertical Axis
- ipsilateral condyle
- Translation of contralateral condyle
- Normal excursion is about 8 mm
- Anterior-Posterior Axis
- Swing in frontal plane of ipsilateral condyle
- Depression (distraction) of contralateral condyle
mandibular depressors (opening)
- gravity
- inferior lateral pterygoid
- anterior digastric
mandibular elevators (closing)
- Temporalis
- Masseter
- Medial Pterygoid
- Superior lateral pterygoid plays role by keeping disc slightly forward during closing
right and left lateral deviators
right: left medial and lateral pterygoids and right posterior temporalis muscle
l eft: Right Medial and Lateral Pterygoids and the Left Posterior Temporalis Muscle
protrude/retruder muscles
Protruders:
- Bilateral Lateral Pterygoids
- Assist by Medial Pterygoids
Retruders:
- Posterior Temporalis Muscle
- Posterior Digastric
- Deep Masseter
general characteristics of facial muscles
- limited peripheral proprioceptive feedback
- small motor units
- attached mostly directly under the skin and to the superficial fascia and to bone
- generally surround facial orifices
- Functions:
- protective- sphincters and dilators for facial orifices
- facial expressions- convey mood during communication
information provided by facial expressions
- Basic emotions (e.g. anger, surprise, sadness, happiness), and more enduring moods such as euphoria, dysphoria, or annoyance, irritability;
- Cognitive activity, such as perplexity, concentration, or boredom;
- Temperament and personality traits such as hostility, sociability or shyness;
- Truthfulness, leakage of concealed emotions, and clues whether the information provided is false;
- Psychopathology, diagnostic information relevant to depression, mania, schizophrenia etc, and also information related to response to treatment.
Recognizing Anger and Associated muscles

- Eyebrows are lowered and pulled together to form wrinkles in
the skin of the forehead (glabella)
- procerus and currugator
- Tensed and straightened lower
eyelids, with tension in lips and mouth.
- orbicularis oris
- Raised upper eyelids causing a glaring look.
- Pressed lips with a slight pushing up of the chin boss
- mentalis, orbicularis oculi
recognizing happy and associated muscles

- Narrowing of the eyelids
- Crow’s feet wrinkling at the corners of the eyes,
- Raised outer and upper area of the
cheeks
- Zygomaticus major and minor and risorius, levator anguli oris
- Lips parted in a smile with teeth showing
recognizing sadness and associated muscles
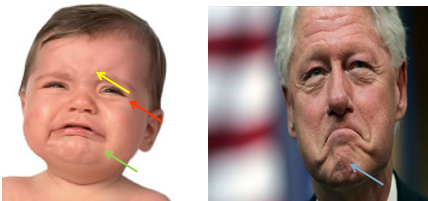
- Eyebrows are lowered and pulled together to form wrinkles in
the skin of the forehead (glabella)
- procerus and corrugator
- Tensed lower eyelids, with
tension in lips and mouth.
- orbicularis oculi
- Widened, and depressed lips, with
a slight push up of the chin boss.
- depressor anguli oris and depressor labii inferioris and mentalis
recognizing disgust and associated muscles
- wrinkled nose with the eyebrows pulled down the upper lip drawn
up
- Nasalis and levator labii superioris alaeque nasi, Levator labii superioris and levator anguli oris
- the lower eyelid is tensed and the eye opening narrowed
- the mouth is open and the upper eyelids relaxed
- orbicularis oris
- turn of the head to the side like you are avoiding something
recognizing fear and surprise and associated muscles
Fear
- raised upper lips and tensed lower lips
- levator palpabrae superioris
- The eyebrows are pulled
up and pulled together
- frontalis
- The mouth is stretched laterally
- depressor anguli oris and depressor labii inferioris
- the
neck muscles pulled
- platysma
Surprise
- eyebrows raised straight up, upper eyelids raised up, jaw
dropped and mouth open.
- similar muscles to fear
Blends of a fear expression and a surprise expression are common.
recognizing pain and associated muscles
- cheek-raising,upper lip raising, nose scrunching
- levator labii superioris aleque nasi, levator labii angularis nasalis
- brow lowering
- corrugator
- horizontally stretches mouth
- mouth open for fake pain, closed (teeth gritted) for real pain (unless vocalizing pain)
- zygomaticus major and minor, risorius
- eye closure (skin
drawn tight around eyes)
- orbicularis oculi
Bell's Palsy
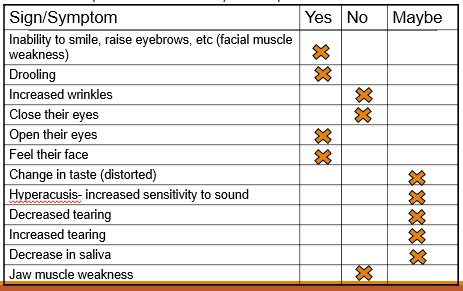
- common cause of unilateral facial paralysis
-
mostly caused by viral sources (Herpes simplex,
flu)
- can be caused by vascular sources such as edema and ischemia (high risk in pregnancy) or the cause may not be known
- causes a compression of the facial nerve in the most narrow part of the canal (labyrinthine portion right before the bend) due to inflammation
- sudden onset (peak within 48 hrs)
- recovery for most within 1-3 months, some have relapses, late
recovery, or incomplete recovery
- risk factors for incomplete recovery: older age, DM, BP, respiratory infections, pregnancy, genetic predisposition, no sign of recovery in first month
- incomplete recovery may result in: muscle tightness, contracture, twitching and/or synkinesis (voluntary muscle action followed by an involuntary action)
- functional difficulties: eating, drinking, speaking, dry eye and mouth, decreased eye protection (cannot close eyes or produce tears), oral hygiene, depression
- treatments: corticosteroids (most effective), Anti-viral therapy, Facial retraining with/or without EMG feedback, Adequate eye care (eye lubrication or ointment) to prevent corneal abrasions and dryness, Surgical decompression very rarely performed
functions of the vertebral column
- Provides a rigid but flexible axis for movement
- Provides a firm base for suspending structures which allow body to maintain cavities with relative constant shape and size
- Provides protection for spinal cord
3 pillars of support of the vertebral column
- 1 major pillar located anteriorly
- Stacking of vertebral bodies joined together by intervertebral discs forming a continuous flexible pillar
- Central axis of body
- 2 minor pillars
located posteriorly
- Stacking of articular processes joined together at synovial joints
cervical spine
- axial skeleton of neck, 7 vertebrae
- support and moves the head
- sensory platform- support and allow movement of the head
- Upper segments
- A/O & A/A joints
- C1 & C2 vertebrae
- Connecting ligaments
- primary concern: stability
- no translatory motion between dens and axis (transverse plane)
- instability can be caused by fracture or ligamentous disturbances, and can be masked by muscular spasms
-
Lower segment
- C3-C7 vertebrae
- C2/3-C7/T1 joints
- Connecting ligaments
Atlas
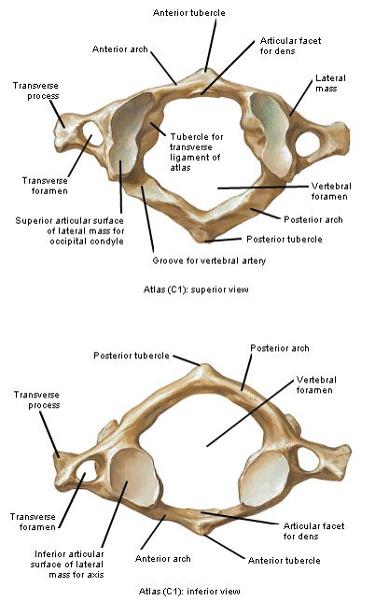
C1 vertebrae
- no vertebral body or true spinous process
-
2 lateral masses-
- Superior facets: concave and elongated, face up and medially
- Inferior facets: flat, circular, face down and medially
- tubercle for attachment of transverse ligament- medial side of lateral masses
-
anterior arch- connects front of lateral masses
- anterior tubercle on anterior surface and facet for dens on posterior surface
-
posterior arch- connects back of lateral masses
- posterior tubercle on post surface represents spinous process
- superior surface has groove for vertebral artery
-
Transverse Processes- long and broad
- levers for muscles that rotate head
- transverse foramen for vertebral artery
Axis
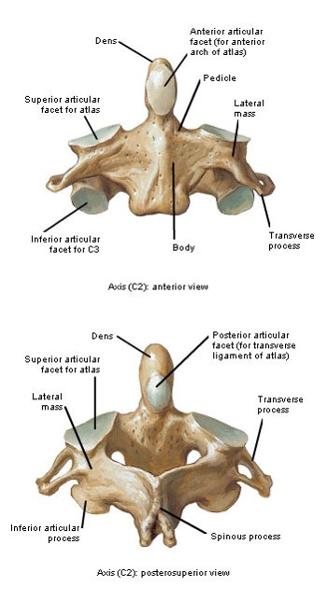
C2 vertebra- pivot on which atlas rotates
- Dens- apex is attachment for apical ligament and sides attach to alar ligaments
- has 5 primary ossification centers- 2 for
dens, 3 for rest of axis
- typical vertebrae has 3 ossification centers- 1 for body, 1 for each root of TP
- pedicles- deep inferior and shallow superior vertebral notches
- laminae- relatively broad
- SP- bifid and large
- TP- relatively small, single tubercle at apex, transverse foramen for vertebral artery
-
Superior articular process- large, oval, faces up
and slightly laterally
- don't form articular pillar
uncovertebral joints (joints of VonLuschka)
- Synovial jts
- only in cervical region
- between uncinate processes of vertebra below and body of vertebra above
-
Bounded:
- anteromedially: IV disc
- posterolaterally: intervertebral foramen (IVF)
- Subject to arthritic changes
- Uncovertebral cleft- fissures that
develop and may completely transect posterior 2/3 of disc
- allows upper vertebra to rotate in relation to lower vertebra
thoracic spine and notable surfaces
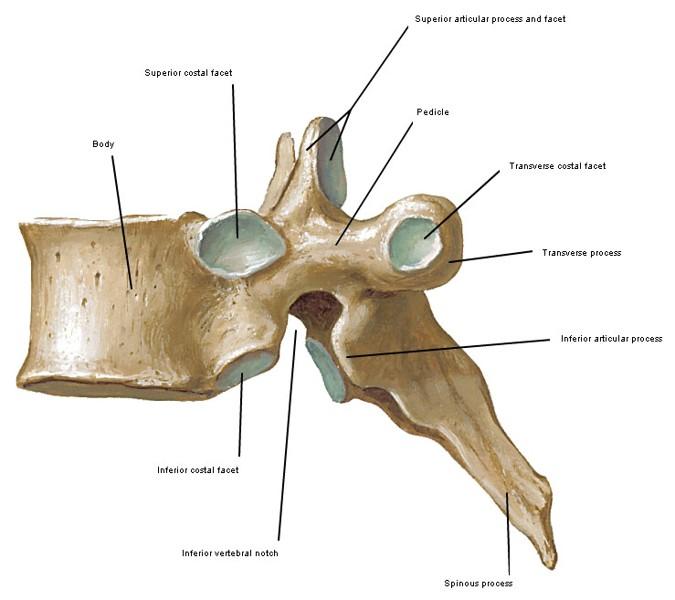
- suspends the ribs and supports respiratory cavity
- 12 thoracic vertebrae that get progressively larger to accommodate increasing loads
- "typical vertebrae"= T2-T8
- 2 pairs of costal facets (demifacets) for
articulation with heads of ribs
- superior pair for numerically same rib
- inferior pair for rib below
- vertebral foramen: relatively small and circular
- laminae: short and broad that overlap the vertebrae below
- Spinous processes: project inferiorly and posteriorly
- apex of kyphosis around T7-T8
- rule of 3's
-
Articular Processes: almost planar surface (just
gliding motion) in frontal plane
- Superior pair face dorsally, slightly laterally and superiorly
- Inferior pair face ventrally, slightly medially and inferiorly
-
Transverse process: thick, oriented laterally and
slightly posteriorly
- Oval facets located anteriorly at tip for articulation with tubercles of numerically corresponding ribs
rule of threes
compares level of spinous processes to level of corresponding transverse processes
- T1-T3: SPs same level as TPs of same vert.
- T4-T6: SPs midway bet. TPs of same vertebra and vertebra below
- T7-T9: SPs same level as TPs of vertebra below
- T10: same as T7-T9
- T11: same as T4-T6
- T12: same as T1-T3
not "typical" thoracic vertebra

1st thoracic vertebra
- Vertebral body has 2 pairs of facets:
- Circular facets located superiorly for 1st rib
- Demifacets located inferiorly for 2nd rib
-
Spinous process is
thick, long and horizontal
- may be as prominent as C7 SP
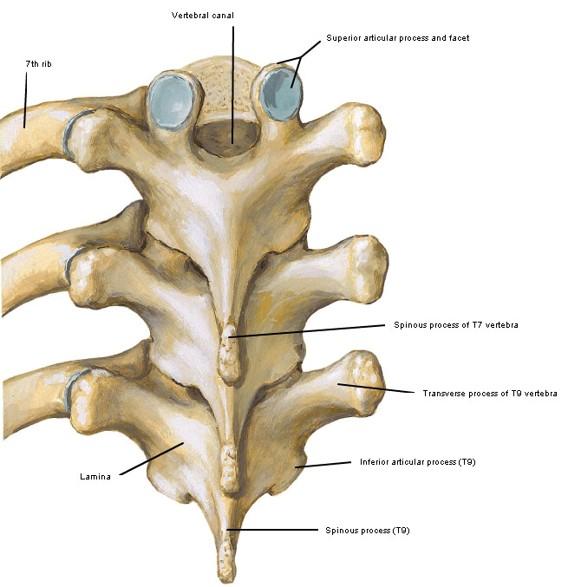
9th thoracic Vertebra
- Vertebral body may or may not form joints with 10th ribs, so may not have pair of demifacets located inferiorly
10th thoracic vertebra
- Vertebral body has only one pair of facets superiorly for articulation with 10th rib
- Transverse process may or may not form joint with 10th rib
11th thoracic vertebra
- only one pair of circular costal facets located superiorly for articulation with head of 11th rib (not 12th)
- TP are small and do not articulate with 11th rib
12th thoracic vertebra
- 1 pair of circular facets: articulates only with heads of 12th ribs
- small TPs with no costal facets
- large vertebral body (more like lumbar)
- superior
articular facets oriented in frontal plane (thoracic), inferior
articular facets oriented in sagittal plane (lumbar)
- change in facet orientation could happen anywhere from T9-L1
lumbar spine
lies opposite the abdominal cavity, 5 lumbar vertebrae
allows mobility between the thorax and pelvis
triangular vertebral canal
lumbar pedicles are often the site of metastasis due to ample vascularity
have mammillary processes on the posterior borders of superior articular processes
sacrum
lies opposite the pelvic cavity, 5 fused vertebrae
unites vertebral column with pelvic girdle
coccyx
rudimentary structure in humans
lends support to pelvic floor
fused bodies of 4 coccygeal vertebrae
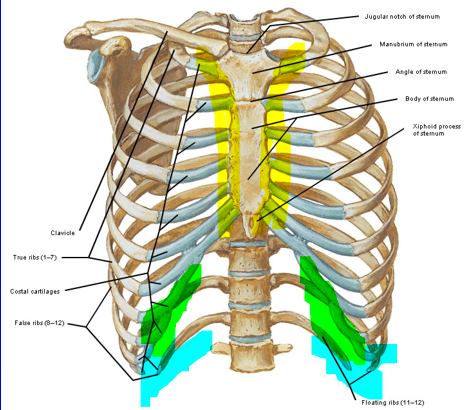
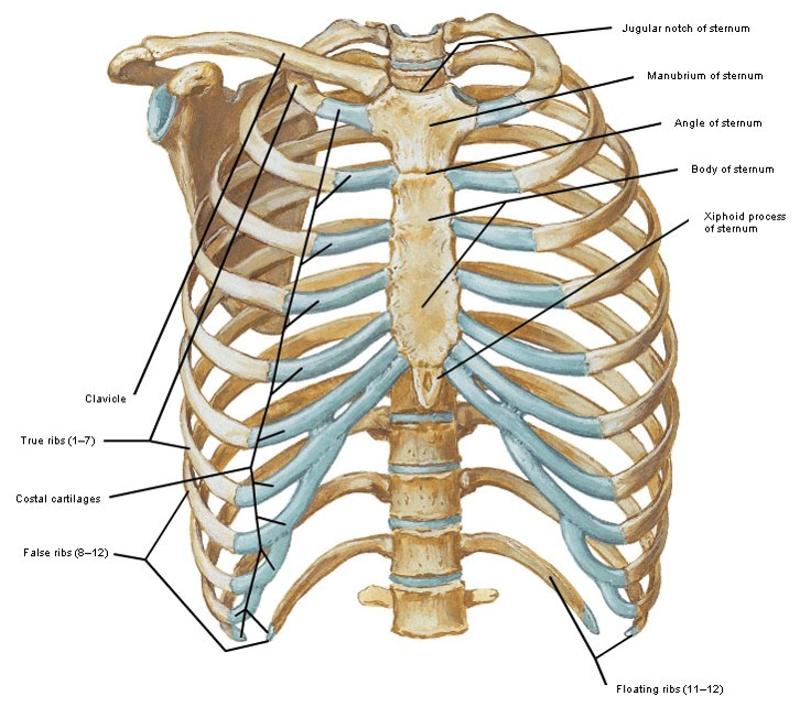
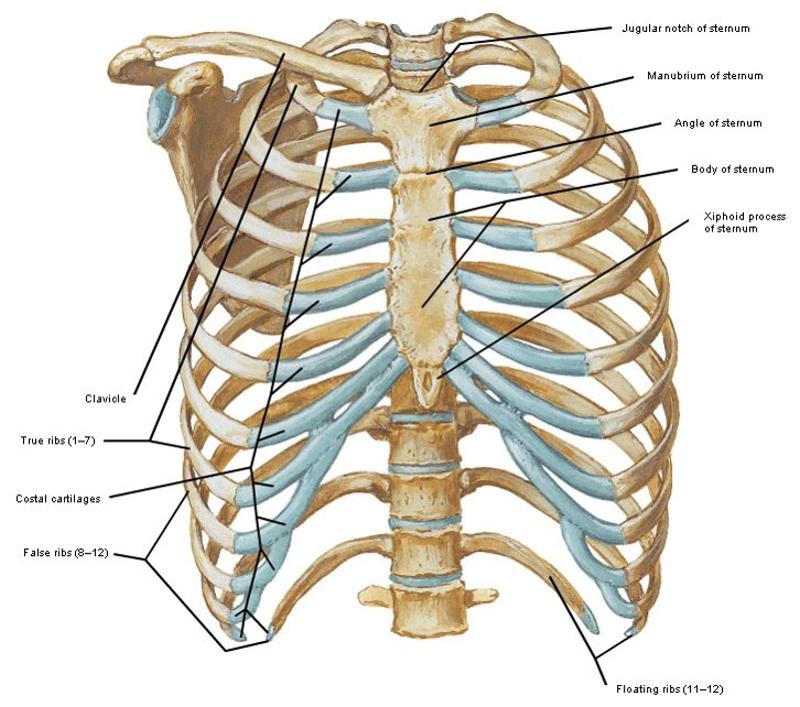
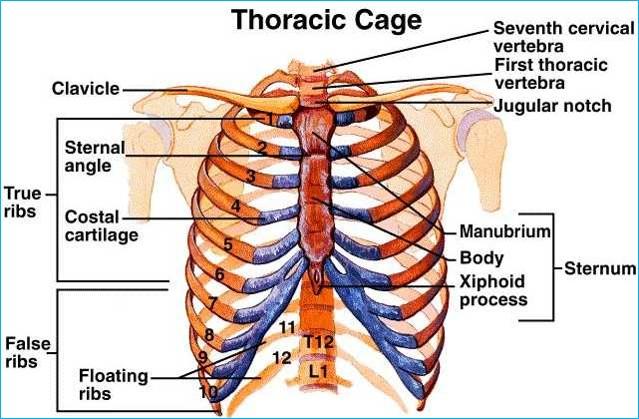
manubrium sterni and body of sternum
- forms a symphysis joint between the inferior manubrium and superior body of sternum at sternal angle (same level as 2nd rib)
-
manubrium- level with 3rd and 4th thoracic
vertebrae
- 2 clavicular notches (sternoclavicular joints)
- costal cartilages- for 1st and 2nd costal cartilages
-
body of sternum- level with 5th-9th thoracic
vertebrae
- costal cartilages- 6 pairs of facets for 2nd-7th costal cartilages
-
Xiphoid process- cartilaginous as a child, ossifies
in adulthood
- articulates with sternum through a symphysis
- costal notches: 1 pair of facets for 7th costal cartilages
ribs
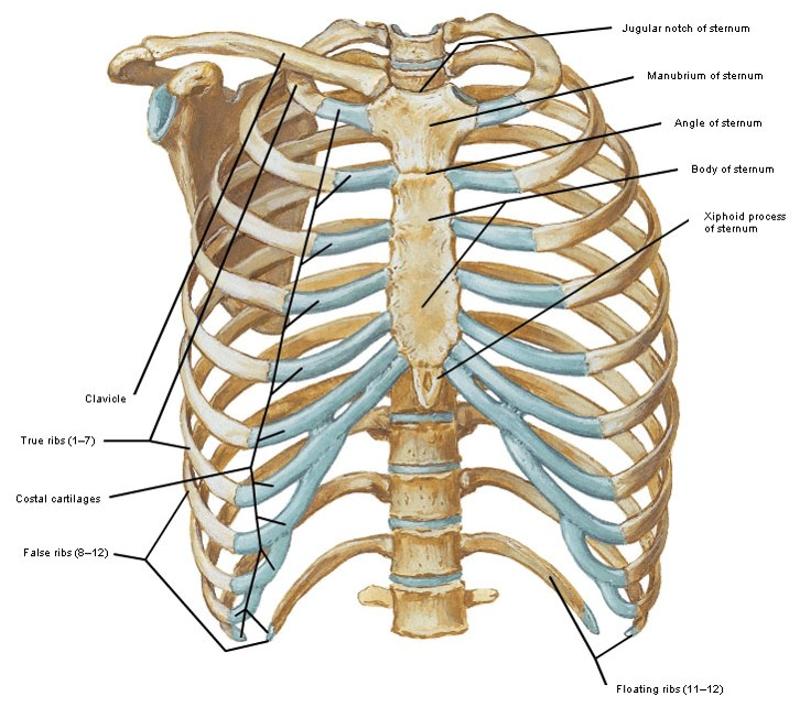
- Arched shafts of bone which articulate anteriorly with sternum and posteriorly with thoracic vert.
- Typically 12 pairs of ribs
- True ribs – 1st 7 pairs of ribs, connected to sternum through their costal cartilage
- False ribs – last 5 pairs of ribs
- Costal cartilages of 8th–10th ribs joined to costal cartilages of ribs just above
- Costal cartilages of 11th & 12th ribs are free at anterior ends – floating ribs
parts of ribs
- infrasternal angle: costal arches meet in midline at xiphoid, angle changes with respiration
- costal groove: undersurface shaft for intercostal arteries and nerves
-
head- posterior with 2 facets and crest in between
- superior facet: vertebral body above
- inferior facet: numerically corresponding vertebral body
- crest attached to intervertebral disc
- Tubercle- junction of neck and shaft with oval facet for articulation with numerically corresponding TP and roughened portion for ligamentous attachment
1st and 2nd ribs
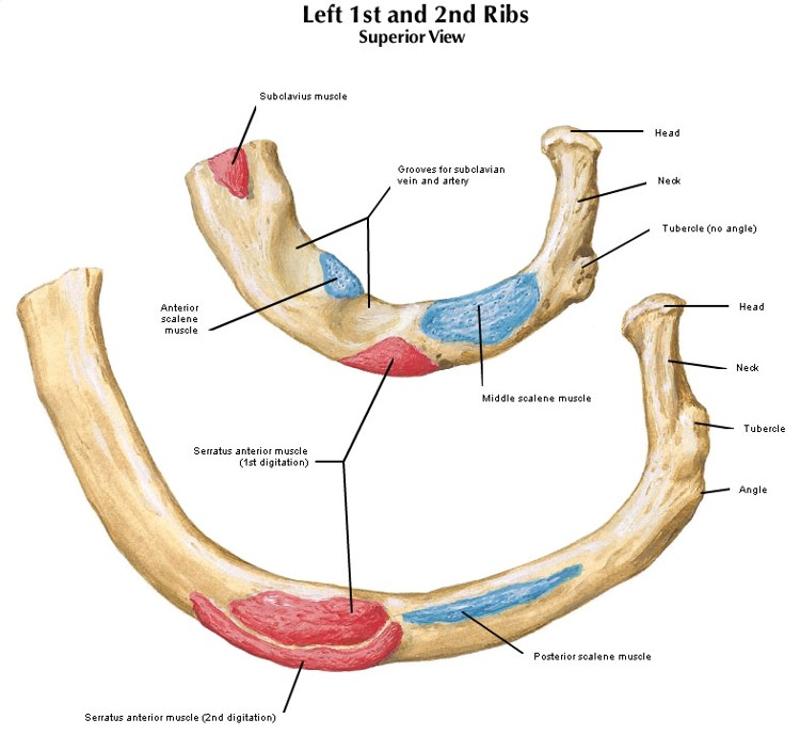
-
1st rib- Shortest, most curved
- Head has single facet for T1 body
- Prominent tubercle
- No angle
- No costal groove
- Scalene tubercle- attachments for scalenous medius and anterior
-
2nd rib
- Longer than 1st rib but similar curvature
- Shaft is not twisted
- Articulates with 2 vertebrae (T1 and T2)
10th, 11th, and 12 ribs
10th rib
- Head has single facet for body of T10 vertebra only
- May or may not articulate with TP
11th and 12th ribs (floating ribs)
- Heads have single facets for bodies of numerically corresponding vert.
- No necks or tubercles
- Ant. ends are pointed & tipped with costal cartilages (do not articulate with costal arch)
- 12th rib is short with no angle or costal groove
costal cartilages
- Flattened bars of hyaline cartilage on anterior parts of ribs
- No movement occurs at costochondral
junctions (where the ribs meet the cartilage)
- do provide chest wall with mobility and elasticity
- With age, may partly ossify and lose their elasticity
- 1st 7 pairs directly connect with sternum
- Next 3 pairs connect with costal cartilages immediately above
- Last 2 pairs are small, pointed & end in muscles of abdominal wall
- medially, the 1st rib connects to sternum via synchondroses (synarthrosis), and the 2-7th ribs articulate through synovial joints
spinal curves
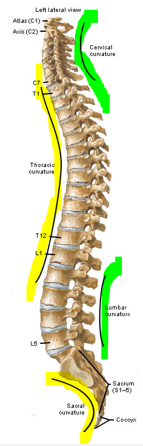
- Kyphotic Curves- Primary Curves
- curve towards anterior side
- Thoracic and sacral region
- Determined by shape of vertebrae
- Lordotic Curves- secondary curves
- curve towards posterior side
- Cervical and lumbar regions
- Regions of greatest mobility
- Enhance weightbearing function of vert. column
- develops from birth to age 10 (adult) with major changes coming as you begin bipedal walking
- sacrovertebral angle is partially due to lumbar vertebrae (esp L5) being deeper anteriorly
vertebral body

-
Thick core of trabecular bone
- Functions in
supporting and distributing weight
- anterior area that only has vertically aligned trabecular bone- likely to fracture
- surrounded by a thin shell of cortical bone
- Functions in
supporting and distributing weight
-
Vertebral endplates
- Superior and inferior surfaces of trabecular bone covered with hyaline cartilage
- Ring Apophyses- epiphyses of the vertebral body where the outer fibers of the vertebral discs attach
-
Uncinate processes- posterolateral part of superior
surface
- Cervical region only
vertebral arch and components
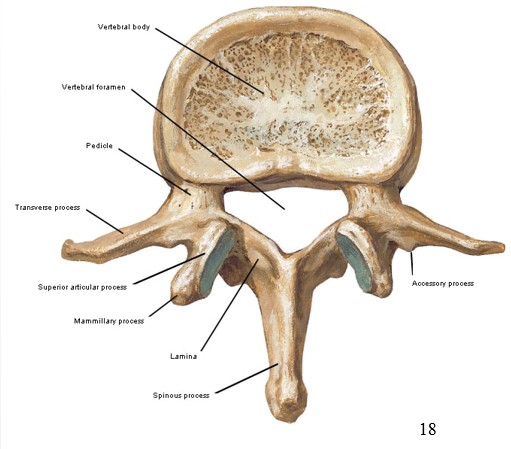
- forms the vertebral foramen (with the vertebral body) and protects neural tissues
- Shape:
- Triangular: cervical, lumbar, and sacral
- Circular: thoracic
- made up primarily of cortical bone (torsional forces)
- Consists of:
-
Pedicles- ventral, ample vascularity
- superior and inferior concavities (notches) form the intervertebral foramen
- Laminae- extend dorsally, fuse in midline
- Spinous process- projects
dorsally from junction between 2 laminae
- function as levers for back extensors
- C2-C6: horizontal, short, and bifid (C7 has single tubercle)
- Articular processes- extend from
junctions of pedicles and laminae
- superior and inferior articular processes with variable orientation by region
- forms articular pillars
- Transverse
processes- projections from junctions between pedicles
and laminae (features vary by region)
- serve as levers for lateral flexors and rotators
- transverse process in cervical vertebrae for passage of vertebral artery
-
Pedicles- ventral, ample vascularity
intervertebral foramina
- formed by the superior and inferior vertebral notches of adjacent vertebrae pedicles
- spinal nerves and dorsal root ganglia pass through
- Cervical Borders:
- posterior: articular pillar (articular facet joints)
- anterior: uncinate process and intervertebral disc
- Thoracic
and Lumbar Borders:
- posterior: facet joints
- anterior: intervertebral disc
- OA in facet joints will lessen disc space and put pressure on spinal nerves
spinous processes shape and inclination
- Shape and inclination varies with region
-
Cervical: thin, short, and horizontal
- bifid C2-C6
- Thoracic: long with downward inclination
- Lumbar: thick and horizontal
transverse processes
projections from junctions between pedicles and laminae
- serve as levers for lateral flexors and rotators
-
Lumbar: L1-L4 TPs are about 1 inch long and thin
- L5 TP is short and thick (so it can fit between ilium bones)
- accessory processes located at roots of TPs (bumps on post side)
-
Cervical: anterior and posterior roots that
terminate in anterior and
posterior tubercles with intertubercular lamella in between
- forms transverse foramen where vertebral artery passes
pars interarticularis and defects
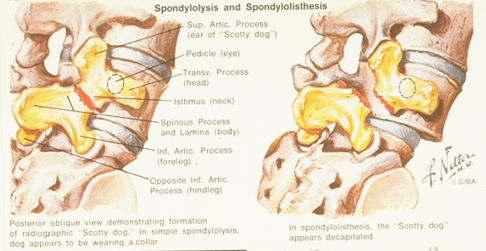
- region connecting the superior and inferior articular processes
- defects only happen in lumbar region (L5)
- L5 looks like a "scotty dog"
-
Spondylolysis- defect in pars
- "step ladder sign"- misalignment of facet joints
- Spondylolisthesis- anterior displacement caused by fractures
sacrum and its parts
- 5 fused sacral vertebrae in a wedge shape
- concave ventrally and convex dorsally
parts:
- Sacral base- top, wider portion which consists of sacral promontory (wider in males), superior articular processes, and ala (wider in females)
-
Sacral canal- triangular shape that contains cauda
equine
- 4 pairs of IVF communicate with 4 pairs of pelvic sacral foramina and 4 pairs of dorsal sacral foramina
Dorsal surface:
- Median sacral crest- from fused sacral spinous processes
- Intermediate sacral crest- fused sacral articular processes
- Lateral sacral crest- fused sacral transverse processes
- Sacral hiatus- inferior end of the sacral canal
- Sacral Cornua- connected to coccygeal cornua through ligaments
- Inferior angles- inferior corners of the sacrum that can be palpated for symmetry
Lateral Surface:
- Auricular surface- covered with hyaline cartilage and articulates with innominate bone
- Areas of ligamentous attachment- roughened areas dorsal to auricular surface
transitional vertebrae
vertabra have features of both adjacent spinal segments where the vertabra change levels
- sacralization- L5 (or part of L5) fuses to the sacrum
- lumbarization- incomplete fusion of S1 to the rest of sacrum
intervertebral discs
- interposed between adjacent vertebrae from C2/3 to L5/S1
- no disc between occiput and C1 and between C1 and C2 (A/O and A/A joints)
- 20-33% of height of vertebral column
- form anterior pillar of vertebral column (with vertebral bodies)
- major compression-bearing structures
- Lumbar region: deeper anteriorly (contributing to lordosis of spine)
-
thoracic region:
jointed laterally to heads of ribs through articular ligaments
- relatively thin, especially upper thoracic discs = less movement at thoracic iV joints (large boody: disc height ratio)
-
Nucleus Pulposus- fine fibrous strands in a
proteoglycan gel (viscoelastic- takes in water)
- 20-50% of disc area with the most in lumbar (9mm), least in cervical (<25% cervical disc volume at birth)
- gel begins to
be replaced by fibrocartilage by age 10 and is indistinguishable
from annulus fibrosis by 60 (comprises viscoelasticity)
- fibrous by 20 years in cervical region
- penetrated by uncovertebral clefts in cervical region
- thoracic region not well developed
- Annulus Fibrosis
annulus fibrosis (AF)
- concentric laminated bands of fibrocartilage and collagenous fibers
- inner fibers attach into cartilaginous endplates
- outer fibers (Sharpey's fibers) attach into ring apophyses and have sensory innervation
-
lumbar discs:
- fibers oriented
obliquely to plane of disc- resist forces from many
directions
- same lamina have parallel fibers, adjacent laminae oriented differently
- posterior laminae joint together and run vertically- more vulnerable to tearing
- fibers oriented
obliquely to plane of disc- resist forces from many
directions
-
Cervical discs: fibers are not
organized in separate laminae, but interweave
- no AF posterolaterally (due to uncovertebral joint clefts)
- anterior AF is major stabilizer in C-spine- often torn in whiplash injuries
- degenerative changes begin after second decade: fibers lose elasticity (esp. post fibers) - vulnerable to tearing
effect of movement on the intervertebral disc
postulated that flexion/extension causes movement of the nucleus, but no evidence has been shown to support this
cannot assume all disc problems should be treated with ext (or flex)
effect of loading on intervertebral disc
in lumbar region:
- in first 2 decades:
- disc is very strong, so a traumatic compressive force is more likely to damage the vertebrae than the disc
- later in
life traumatic compression will result in:
- in lordic (locked back- straight) posture: schmorl's nodes
- in flexed or rotated posture: herniation
- shearing and torsional forces are most damaging to disc
innervation to intervertebral disc
- Sensory nerve endings found in disc as far as half way into AF
- possible source of pain
- Posterior AF supplied by sinuvertebral nerve
- Lateral and ventral parts of AF, along with ALL, supplied by branches of VPR
motion segment
- The smallest segment of the spine that exhibits biomechanical characteristics similar to those of the entire spine
- consists of:
- Two adjacent vertebrae and their articular elements
- Interposed disc
- Connecting ligaments
intervertebral joint
- symphysis joint- disc forms bond between 2 adjacent vertebrae
- Cervical- resemble saddle joints
- disc deformation permits movement between vertebral bodies
- directly related to size of disc
- body-to-disc ratio: closer ratio = larger disc height and more movemen
- Ligaments:
- anterior longitudinal ligament
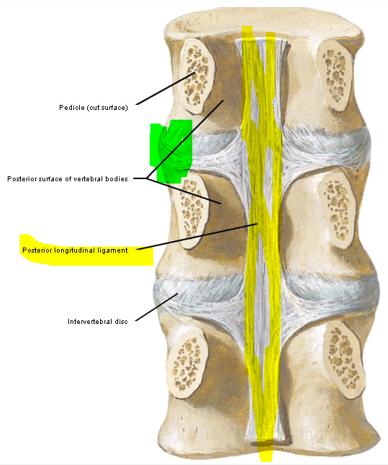
- posterior longitudinal ligament
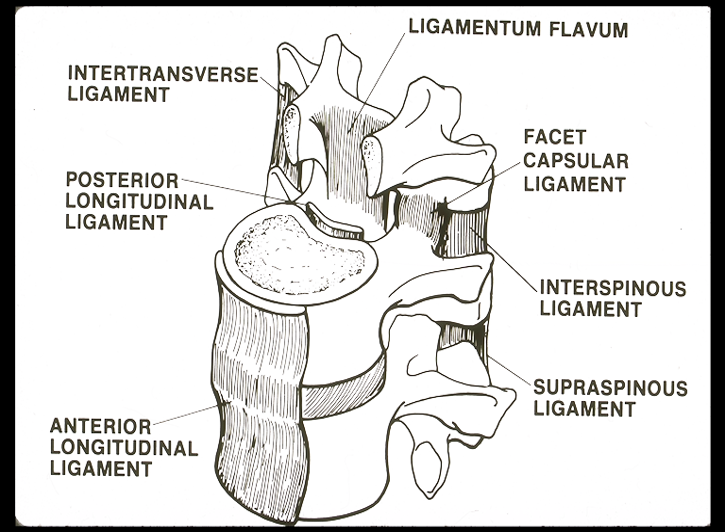
ligaments of intervertebral joint
- anterior longitudinal ligament (ALL)
- reinforce intervertebral joints
- from basilar part of occiput to S1 on anterior aspect of vertebral column
- varies by region:
- Cervical: Thin and narrow
- heavily innervated with pain fiber
- Thoracic: Thick and broad
- Lumbar: Thin and broad
- blends with crura of diaphragm
- posterior longitudinal ligament (pictured)
- from body of axis (C2) to S1 along posterior aspect of vertebral bodies
- forms protective barrier between spinal cord and vertebral column
- broad and uniform in upper thoracic region
- narrow and has projections (denticulated) in lumbar region and lower thoracic region
- risk for posterolateral disc herniation
iliolumbar ligament
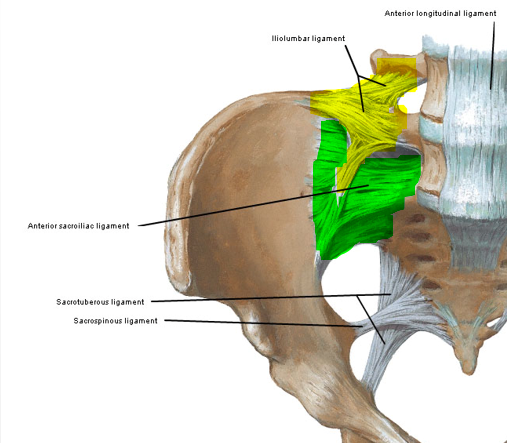
- Reinforcing ligament of Lumbar-Sacral junction
- Arises at tip of L5 TP (& sometimes L4 TP)
- Gives rise to 2 bands
- Upper band projects laterally to iliac crest
- Lower band blends with ventral SI lig.
- develops from metaplasia (turning muscle into ligament) of either quadratus lumborum of L5 fascicle of iliocostalis lumborum (related to more upright posture)
- stabilizes L5/S1 segment during movement (lateral and torsional
forces), esp if there's disc degeneration
- resists anterior shear at L5/S1
facet joints (zygapophyseal joints)
- Synovial joints formed between superior (from the vertebra below) and inferior (from vertebra above) articular processes of adjacent vertebrae
- Enclosed by fibrous joint capsule
- May contain intra-articular inclusions (ex. Fat pads)
- Facet joint orientation: different in different regions
- facets stabilize spine, protecting discs from shear forces and excessive movements
-
facet joint
capsule- strongest of posterior ligaments, but fairly loose
in cervical spine and taut in lumbar spine
- reinforced ventrally by ligamentum flavum and laterally by intertransverse ligaments
articular facet joint orientation
- Cervical: between frontal and transverse planes
- Upper cervical spine: ONLY transverse plane
- Contribute minimally to weight bearing and impede forward translation (from frontal plane orientation)
- Superior Facet: up and back
- Inferior facet: down and foreward
- Thoracic: frontal plane
- Resist forward translation
- Allows side bending
- facet joint capsules more taut than in cervical region
- Lumbar: Upper facets oriented in sagittal plane, L4/5 between sagittal and frontal plane, L5/S1 highly variable
- Resist forward translation and axial rotation (ant shear)
- Sup Facet: concave and faces dorsomedially
- Inferior facet: is convex and faces ventrolaterally
- allows motion primarily in sagittal plane
ligaments of vertebral arch
- Ligamentum flavum
- Supraspinous ligament
- Interspinous ligament
- Nuchal ligament
-
Intertransverse ligaments- between adjacent
transvers processes
- blends with intertransverse muscles
- round cords in thoracic region
ligamentum flavum
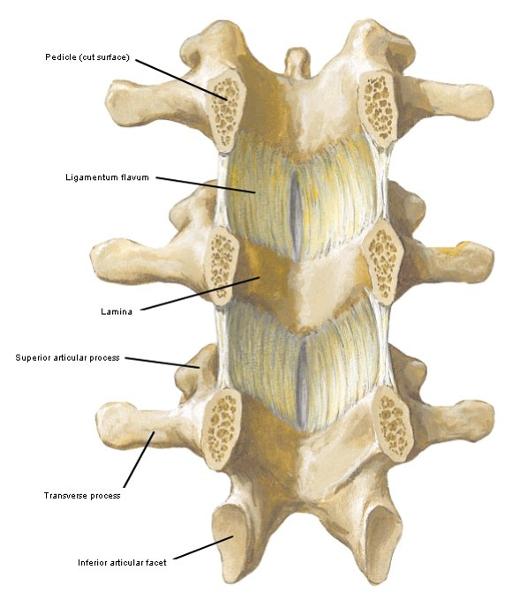
connects laminae of adjacent vertebrae from C1/C2 to sacrum (thickest in lumbar)
- yellow elastic tissue- allows stretching during flexion and springs back to allow extension
- accommodates large changt in intralaminar distance in flex/ext
- too stretchy to limit movement
- loses elasticity with age- can buckle under the spine during extension
- only connects to C1/C2 because
myodural bridges between C2 (suboccipital muscles) and dura mater to
prevent the dura mater from folding in on itself during extension
- myodural passes through C1/C2, so ligamentum flavum can't fit
- relatively thick in thoracic region
supraspinous ligament
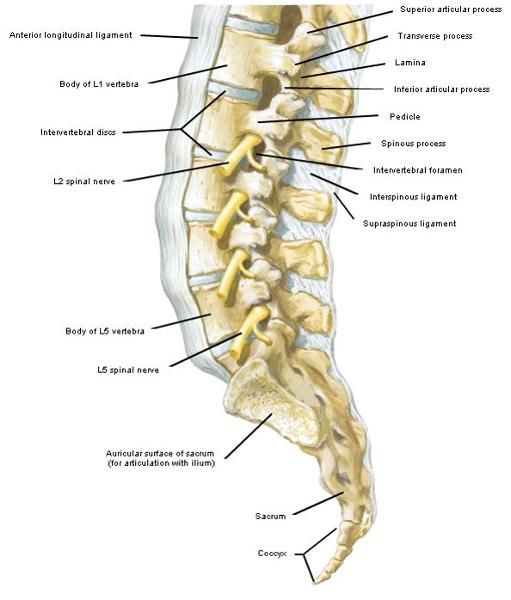
C7 to sacrum (or L5), connecting tips of SPs
- thicker in lumbar spine, blending with adjacent fascia in thoracic region
- not present in cervical spine
interspinous ligament
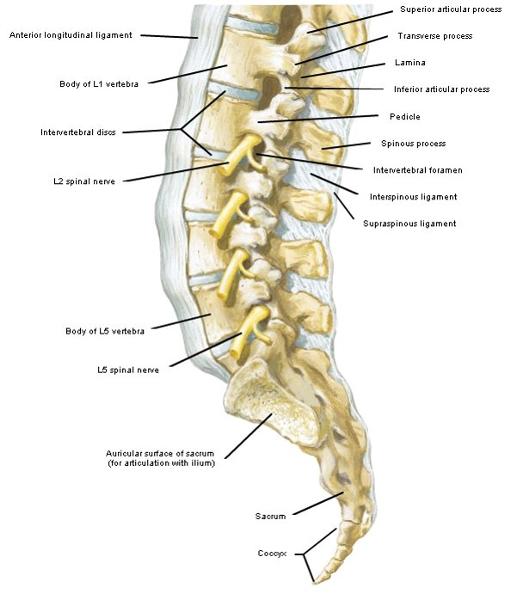
extends between adjacent SPs
- thinner than supraspinous lig, thickest in lumbar spine, lacking in cervical spine, thin in thoracic region
- fibers have a dorsorostral orientation (opposite what is in picture)- cannot resist shear forces
- not present in cervical spine
nuchal ligament
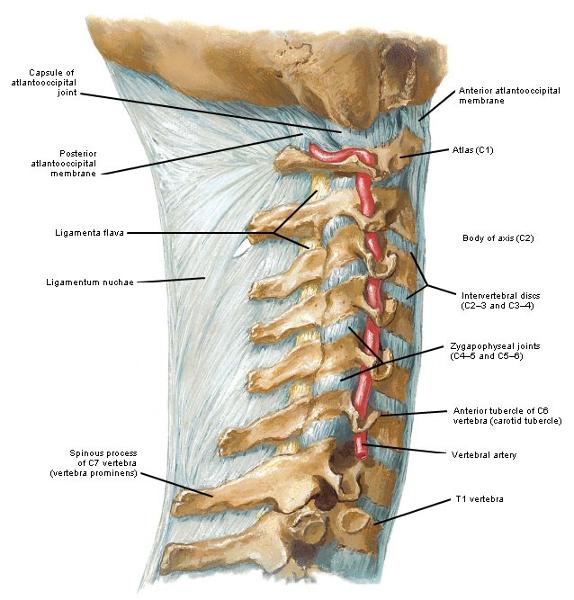
C7 to occiput connecting cervical SPs
- midline raphe is origin to: upper trapezius, splenius capitis and rhomboid minor
- (Deeper) midline fascial septum separates semispinalis capitis muscle bellies
- homologous to interspinous and suprspinous ligaments in cervical region
characteristics of muscles of the vertebral column by grouping
- Unisegmental muscles- DPR
- Short, deep, connecting adjacent vertebra
- Found along entire length of vertebral column
- too small to contribute significantly to powerful motion
- stabilize adjoining vertebrae for more effective action of longer postvertebral muscles
- Postvertebral muscles- DPR
- Longer, more superficial “chains” of muscles down vertebral column
- Found along entire length of vertebral column
-
Lateral muscles- VPR
- Not found in thoracic region
-
Prevertebral muscles- VPR
- Not found in thoracic region
Ventral and Dorsal Compartments of Spine
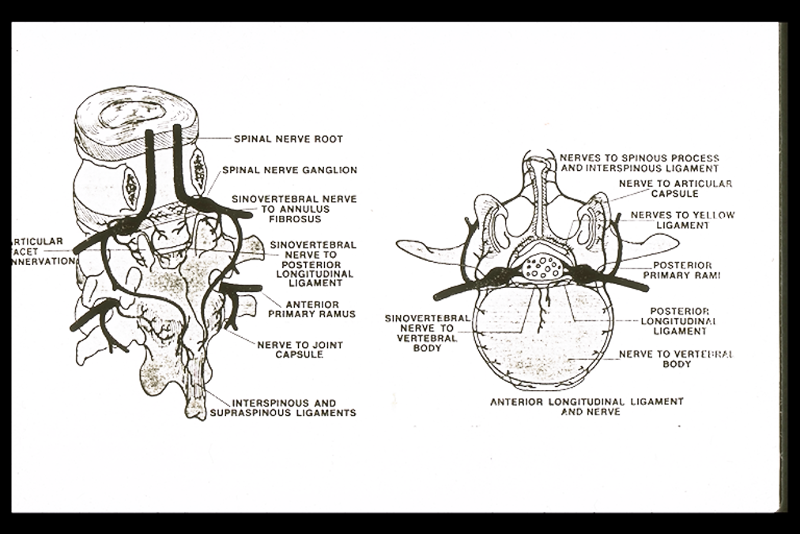
- Ventral compartment
- Innervated by ventral primary rami (sinuvertebral nerve to much of compartment)
- Structures include:
- ventral dura mater, intervertebral discs, ALL, PLL, prevertebral muscles, vertebral bodies and pedicles
- Dorsal compartment
- Innervated by
dorsal primary rami
- cervical and thoracic regions: divides into medial and lateral branches
- lumbar region: divides into medial, intermediate, and lateral branches
- Structures include:
- neural arches, facet joints and ligaments, deep muscles of back
sinuvertebral nerve
- Innervation to much of ventral compartment
- Branch from VPR which goes back into vertebral canal
- Supply to ventral dural sac, blood vessels, posterior annulus and PLL
- has sensory innervation= possible source of pain
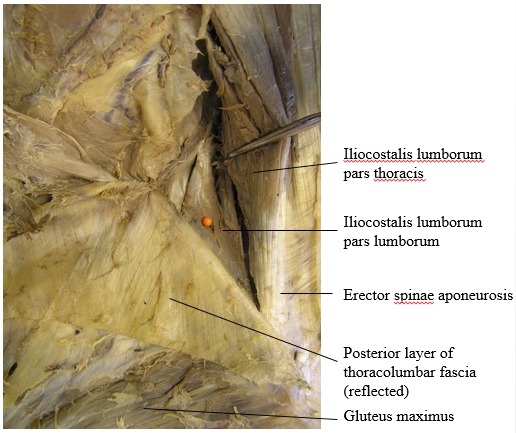
iliocoatalis lumborum
-
Pars lumborum: deeper, shorter
- 4 large muscular fascicles (L1-L4)
- iliolumbar lig may represent missing L5 fascicle
-
Pars thoracis: superficial, longer
- 8-9 fascicles with small muscle bellies
- long caudal tendons that form lateral erector spinae aponeurosis (ESA) with longissimus thoracis pars thoracis
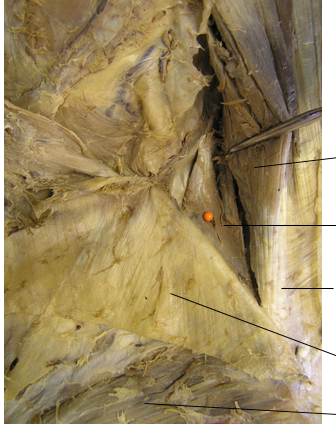
label the structures indicated by the lines
erector spinae anatomy clinical relevance
- Tenderness around PSIS could be due to tear or avulsion in
lumbar intermuscular aponeurosis
- aponeurosis has a small insertion on PSIS -> large stresses
- Fascicles of ILpL and LTpL
could act independently (muscle spasm)
- reducing lumbar
lordosis
- flat back commonly seen in patients with acute episodes of Lower back pain (LBP)
- reducing lumbar
lordosis
thoracolumbar fascia
3 layers:
-
Anterior- from anterior lumbar TPs
- nothing attaches, but it covers the anterior side of quadratus lumborum
-
Middle- from tips of lumbar TPs
- gives rise to transverse abdominis between rib 12 and iliac crest
-
Posterior- from thoracic and lumbar SPs and
interspinous and supraspinous ligaments
- latissimus dorsi and serratus posterior inferior attach
- acts as retinacula to prevent bowstringing of low back extensors
- superficial lamina- oriented caudomedially
- deep lamina- oriented
caudolaterally
- best developed in lumbar-sacral region between L4/L5 and sacral SPs to iliac crest and PSIS
- acts as accessory posterior ligs to resist flexion moment
- fibers from L5 and S1 fuse with ESA, fibers from L3 (& L2) fuse with middle layer of TLF at lateral raphe
All 3 layers fuse at the lateral border of the erector spinae to for the lateral raphe (gives rise to posterior fibers of internal abdominal oblique)
single plane movement of lumbar vertebrae
- rotation and translation along A/P (sagittal), M/L (frontal), and vertical axes
- motion described relative to vertebra below and primarily in the sagittal plane (due to facet orientation)
- lower levels slightly more mobile
-
flex/ext- high degree of individual variability,
can be limited by hip extensor or lumbar spine tightness
- 2-3mm of anterior translation of upper vertebra on lower during flexion (most at L4/L5, least at L5/S1)
- first 50-60 degrees are lumbar flexion then remaining movement is from rotating the pelvis
segmental motion in lumbar spine
- axial rotation
- L3/L4 and L4/L5 are slightly more mobile than other segments
- lateral bending
- more motion at upper 3 segments (L1-L3), less motion at L4/L5, and least at L5/S1
- L5/S1 tends to bend in opposite direction
- in neutral and extension side
bending and rotation are opposite
- no correlation in flexion
muscular activation during lifting
back extensors, posterior hip, and abdominals can all be activated and increase with an increased weight of load and increased distance between the load and the body
back extensors contribute more when the back is extended- beneficial to protect the spine
keeping the load closer to your body will help to avoid shear forces
cervical intervertebral joint movement
- flexion/extension in sagittal plane
- lateral flexion
coupled with rotation in plane of facet joints
- broad disc limits lateral flexion
- uncinated process provides lateral stability by limiting lateral flexion
cervical facet joints (typical joints C2/3-C6/7) and their motions
- think of them as planar joints (only gliding and concavity are not as important)
- Orientation in oblique plane motions:
- facilitates sagittal plane motion
- flexion: upper
facets move superiorly and anteriorly on lower facets
(minimal facetal contact in full flexion)
- limited by tension in PLL, articular capsule, and ligamentum nuchae
- extension: opposite flexion, limited by tension in ALL, impact of SPs, and sup articular process of vertebra below with TPs of vertebra above
- flexion: upper
facets move superiorly and anteriorly on lower facets
(minimal facetal contact in full flexion)
- requires axial rotation
and lateral flexion always coupled to the same side
- opposite rotation in A/A joint allows you to keep your head straight during lateral bending
- provides for some weight-bearing capability
- impediment to forward translation
- facilitates sagittal plane motion
- Inferior articular facet
- Slightly concave
- Face inferiorly and anteriorly
-
Superior articular facets
- Slightly convex
- Face superiorly & posteriorly
- Enveloped in baggy capsules-lax in neutral position and taut in extremes of motion
- May contain intra-articular
inclusions
- Fat pads, fibroadipose menisci
Atlanto-Occipital Joints (A/O Joints) and movements
- synovial ellipsoid joint
- Atlantal facets- concave,
tilted medially, occipital condyles- convex
- convex on concave
- 2 joints act as one to move around the transverse axis (nodding) and AP axis (slight amount of flexion)
-
Movement during
flexion: occipital condyles roll anteriorly and glide
posteriorly (ext is opposite)
- more A/O joint movement in extension (25 deg) than in flexion (10 deg)
- Movement during lateral flexion: Ipsilateral occipital condyle
glides anteriorly, medially & inferiorly (other condyle moves
oppositely)
- some conjuct rotation occurs to opposite side (~5 deg)
Atlanto-Occipital joint capsule and ligaments
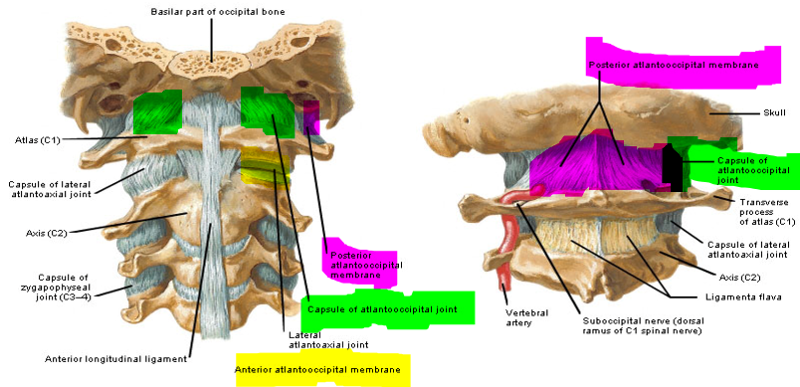
-
fibrous
Capsule- thickened posterolaterally
- thin and sometimes lacking medially where the joint may communicate with the bursa between dens and transverse ligament
-
anterior
atlanto-occipital membrane: broad, dense
membrane between foramen magnum and anterior arch of atlas
- strengthened by anterior longitudinal ligament
-
posterior
atlanto-occipital membrane: broad, thin membrane
between foramen magnum and posterior arch of atlas
- arches over groove for vertebral artery forming opening for artery
atlanto-axial joints (A/A joints)
Lateral
- synovial joints with thin and loose capsules
- shapes of facet surfaces are debatable
Median
- synovial pivot joint between dens and ring formed by anterior arch of atlas and transverse ligament
- posteriorly, larger synovial cavity lies between transverse ligament and dens
Movement
- occurs simultaneously at all 3 joints
- lateral joints support the weight of the head via the alas
- medial joint guides rotation
-
Primary movement-
rotation: dens should not move, but acts as a pivot around
which movement occurs
- when upper facet glides forward or back it also descends (if both surfaces are convex)
- limited by alar ligaments
- Small amount of flexion/ext
- flex- inferior facets of atlas roll anteriorly and glide posteriorly; anterior arch of atlas glides inferiorly (ext is opposite)
transverse ligament
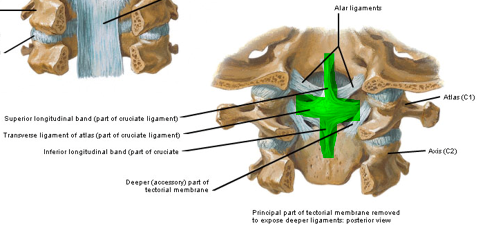
thick, strong band dividing the ring of the atlas into 2 unequal parts that form a cross "Cruciform ligament":
- major transverse part
- small band- extends up to occipital bone and down to body of axis (between tectorial membrane and apical ligament)
attached on each side to tubercle on lateral mass
medial portion lined with cartilage for articulation with dens
keeps dens in contact with anterior arch of the atlas during all movements (so it doesn't touch the spinal cord)
tectorial membrane
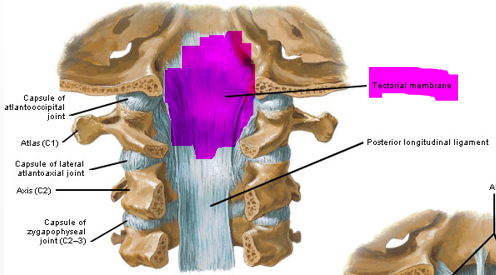
cranial extension of posterior longitudinal ligament within vertebral canal
broad, strong
runs from body of axis (C2) to occipital bone in front of foramen magnum
may act as a back up to the traverse ligament to limit posterior movement of dens
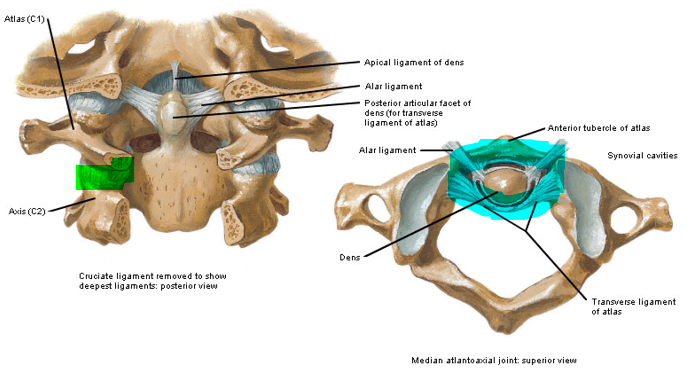
alar ligament
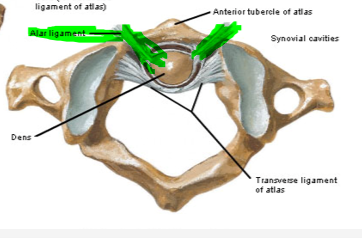
- 2 strong cords run from dens obliquely superiorly and laterally to condyles of occiput
- Primary restraints for
contralateral rotation &
lateral flexion
- secondary restraint for flexion
- Most taut with flexion or extension combined with rotation
apical ligament of dens
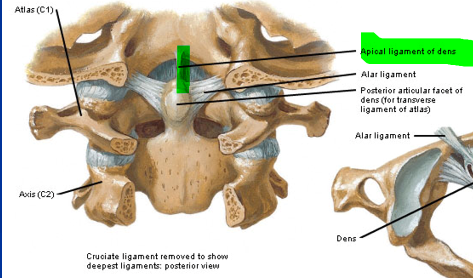
from tip of dens to anterior margin of foramen magnum
very thin
lies between upper band of cruciform (transverse) ligament and anterior atlanto-occipital membrane
movements in thoracic spine
- movements are limited- so they don't interfere with respiration
- flexion/extension
- minimal due to frontal orientation of facets
- there is more movement as you move caudally
- rotation
- relatively free in thoracic region
- more in upper levels, decreases as you move caudally
- limited by ribs and facet joints
- costal cartilages of ribs deform to same side as rotation
- Lateral flexion
- limited (especially in upper thoracic levels) by resistance of ribs and sternum, not by facet orientation
- Coupled
movement
- Upper thoracic – Side bending and rotation are same
- Lower thoracic – inconsistent coupling pattern
costovertebral joints and ligaments
- Synovial joints formed between heads of ribs and thoracic vertebral bodies and interposed intervertebral discs
- 1st, 10th, 11th & 12th ribs articulate with a single vertebral body
- Fibrous Capsule- Single capsule surrounds jt. formed between rib head, adjacent vertebra and IV disc
-
Intra- articular
Lig.–Located within capsule, extending from crest
of rib to IV disc, dividing jt. into 2 separate cavities
- Absent in costovertebral jts. of 1st, 10th, 11th & 12th ribs
-
Radiate Ligament- 3 bands extend from head of rib
- Superior band -To body of upper vert.
- Inferior band - To body of lower vert.
- Intermediate band- To interposed disc
costotransverse joints and ligaments
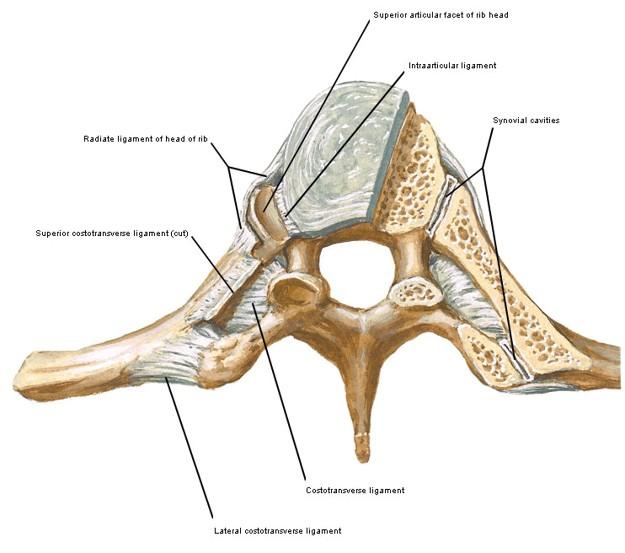
- Synovial joints formed between tubercles of ribs and facets on transverse processes
- Absent at 11th and 12th ribs
- Fibrous Capsule-thin
- Superior Costo- transverse lig. –From neck of rib to TP of vertebra above
- Costotransverse Lig .- From neck of rib to anterior TP of corresponding vertebra
- Lateral Costo-transverse Lig.–From non-articular part of rib tubercle to TP tip
sternocostal joints
- Periosteum and perichondrium are continuous at these junctions
- 1st costal cartilage unites with manubrium at synchondroses (synarthrosis)
- 2nd –7th costal cartilages articulate with sternum at modified synovial joints
- slight gliding occurs at sternocoastal joints with respiration
- mostly the ribs move as a unit with the sternum
Interchondral joints
synovial joints
located between 6th and 7th, 7th and 8th, and 8th and 9th costal cartilages
enclosed in a fibrous capsule by interchondral ligaments
movement of ribs
- slight gliding occurs at sternocoastal joints with respiration
- mostly the ribs move as a unit with the
sternum
- up to 3cm of movement from full inspiration to full expiration in healthy individuals
-
minimal movement at costovertebral and
costotransverse joints due to strong ligamentous support
- ribs rotate about an axis passing through the center of both joints and through the neck of the ribs
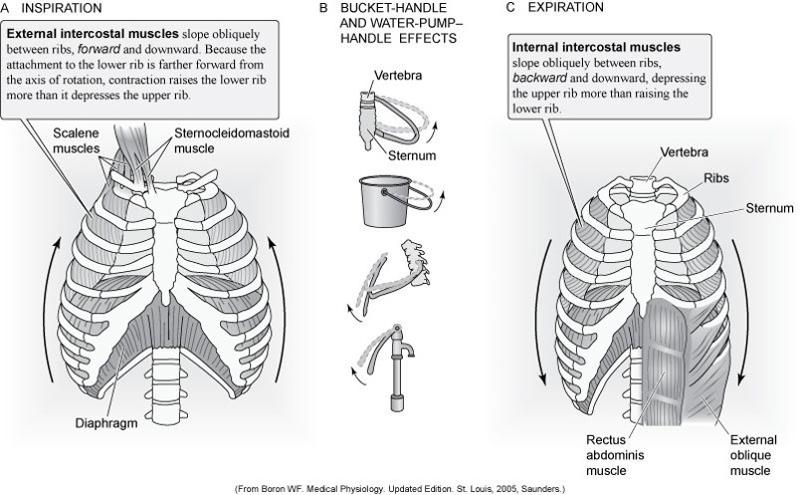
- ribs 1 and 2 -move upward and laterally (minimal with quiet respiration)
-
ribs 3-6: pump handle (movement increases A/P diameter of thorax)
- axis of rotation approximated frontal plan (movement in sagittal plane)
- do not increase infrasternal angle
-
ribs 7-10: bucket handle (increases transverse diameter of
thorax)
- axis of rotation in sagittal plane
- increases the infrasternal angle
-
ribs 11-12: can move slightly in all directions
- depressed by quadratus lumborum so diaphragm can act more efficiently during inspiration
posterior triangle
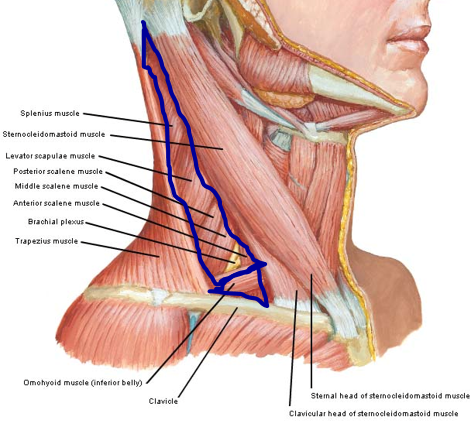
borders:
- anterior: sternocleidomastoid
- posterior: trapezius
- inferior: clavicle
- inferior belly of omohyoid muscle subdivides the posterior triangle into an upper occipital triangle and a lower supraclavicular triangle
musculo-aponeurotic walls of abdomen
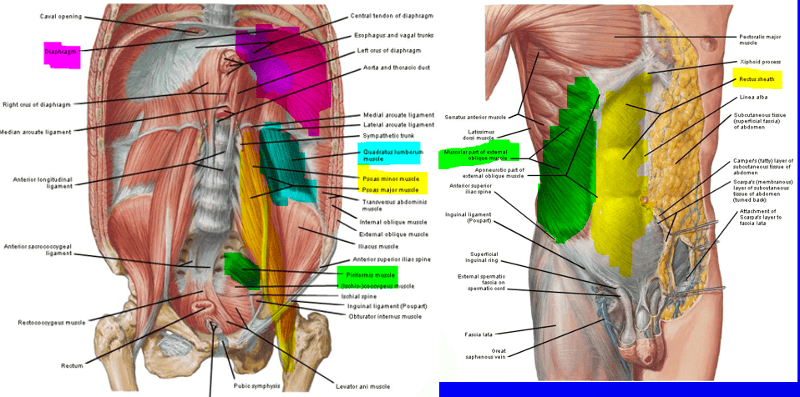
- Anterior wall
- Rectus abdominis
- Pyramidalis
- Rectus sheath
- Lateral wall
- Transversus abdominis
- Internal oblique
- External oblique
- Iliacus
-
Posterior wall
- Psoas muscles (major and minor)
- Quadratus lumborum
- Piriformis
-
Superior Wall
- Diaphragm
- Inferior wall
- Muscles of pelvic floor
fascial lining of muscular wall
- fascial lining made up of loose connective tissue
- Continuous fascial layers that line body wall forming separation between muscular wall and peritoneum (serous membrane covering organs in abdominal and pelvic cavities)
- Fascia:
- Transversalis fascia- Lines transversus abdominis
- Diaphragmatic fascia-Lines diaphragm
- Iliac fascia- Lines iliacus
- Anterior layer of TLF- Lines quadratus lumborum
- Pelvic fascia- Covers pelvic floor muscles
fascia of abdominal wall
- upper part is single layer of fatty subcutaneous tissue
- lower part has 2 layers
- Fascia of
Camper- superficial fatty
subcutaneous layer
- continuous with superficial fascia of thigh
- Fascia of
scarpa- deep membranous
- attached medially to linea alba and symphysis pubis, and continuous below with fascia lata of thigh
- somewhat adherent to external oblique and rectus sheath.
- Fascia of
Camper- superficial fatty
subcutaneous layer
aponeurosis of external oblique
- Most fibers extend inferomedially, anterior to rectus abdominis, to end in Linea Alba
- Below, it attaches to pubic symphesis and crest to tubercle
- Forms Inguinal Ligament between ASIS & pubic tubercle
inguinal canal
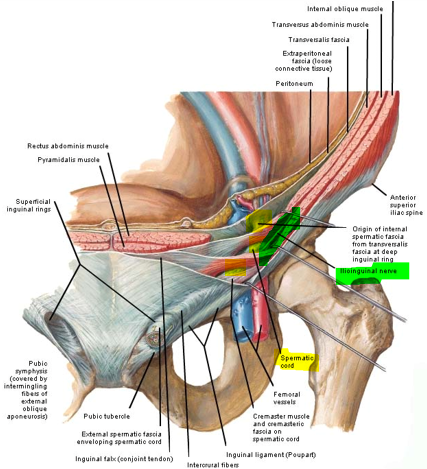
- Contains spermatic cord ( in men, round ligament in women) and ilioguinal nerve
- Extends from deep inguinal to superficial inguinal rings
- Deep inguinal ring - opening in transversalis fascia (lining transverse ab muscle)
- Superficial inguinal ring - opening in aponeurosis of ext oblique just sup & lat to pubic tubercle
- Potential weak spot in abdominal wall - inguinal hernia
aponeurosis of internal oblique
- Upper 2/3 splits to enclose rectus abdominis and ends in linea alba
- Ant. layer blends with aponeurosis of ext. oblique
- Post. layer blends with aponeurosis of transversus abdominus
- Lower 1/3 does not split, but remains entirely anterior to rectus abdominis to end in linea alba
- Thoracoabdominal, subcostal, iliohypogastric and ilioinguinal nerves run between transversus and internal oblique
aponeurosis of transversus abdominis
- Upper 3/4 passes behind rectus abdominis to blend w/aponeurosis of internal oblique
- Lower 1/4 passes anterior to rectus abdominis
Rectus Sheath
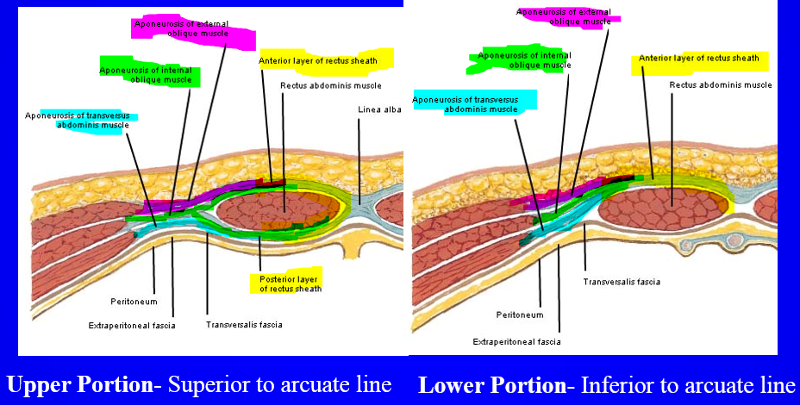
- Aponeurotic sheath enclosing Rectus abdominis
- Ends in midline to form linea alba, blending with rectus sheath of opposite side
Upper portion- above arcuate line
-
anterior layer:
anterior portion of apo of internal oblique and external oblique
- runs cuadomedially (direction of external oblique)
- runs rostromedially (direction of internal oblique)
Lower Portion- below arcuate line
- anterior layer: apo of transversus abdominis, internal ab oblique, and external ab oblique
abdominal hollowing (drawing in maneuver)
- Selective activation of transversus abdominis, without
recruitment of internal abdominal oblique
- bring belly button towards butt or bring ASIS together
- transversus and internal oblique both are activated and important in stabilizing the spine
- Thought that transversus is critical muscle in feedforward control for support of lumbar spine – “motor control issue”
connective tissue of rectus abdominis
-
Linea Alba- Tendinous raphe, extending from xiphoid
to pubic symphysis
- separating Rectus abdominis (RA) into right and left sides
-
Tendinous intersections- 3 zig-zagging
intersections that interrupt RA
- at level of umbilicus, level o xiphoid, and midway between those 2
- adherent to rectus sheath
- Linea semilunaris- lateral border of RA
musculo-aponeurotic brace around trunk
- Aponeurotic sheaths around muscles that extend and flex vertebral column
- Thoracolumbar fascia posteriorly
- Rectus sheath anteriorly
- Flat
abdominal muscles exert lateral pull on both lateral
raphe &
linea semilunaris
- lateral tension on TLF may contribute to stiffening L-spine
- Spinous processes & linea alba act as anchor points for Medial/Lateral stability
diaphragmatic apertures (hiatus)
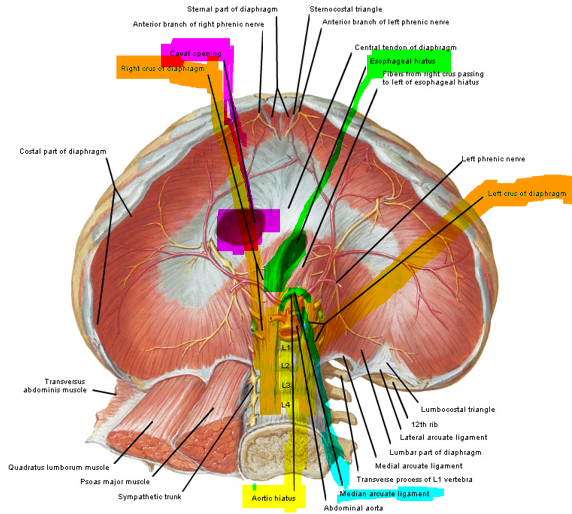
-
Aortic
aperture- over vertebrae (behind diaphragm) and
between the 2
crura
- surrounded by median arcuate ligament (so it will not change size)
-
Esophageal aperture-In muscular part
behind central tendon
- can close since it is surrounded by muscles when it is not needed
- Vena caval aperture- Within central tendon on right side
abdominal muscles and low back pain
- Possible that synchronized effort of selected spinal
stabilizers (quadratus lumborum and transversus
abdominis) together with diaphragmatic action enhances both
breathing efficiency and stability of lumbar spine
- low back pain is a “motor control issue”
muscular activity in respiration
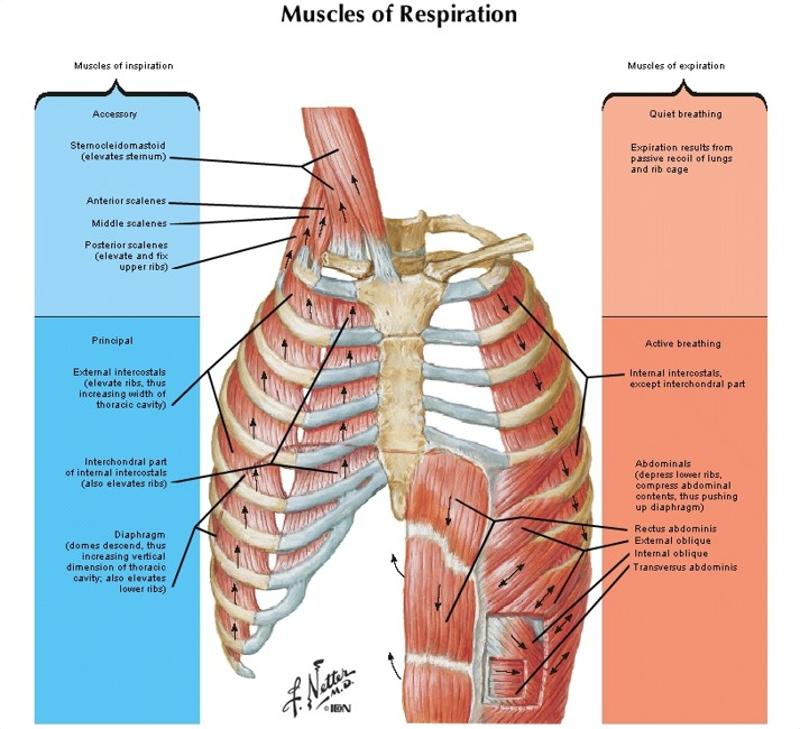
inspiratory muscles= diaphragm and external intercostals
expiratory muscles= abdominals, internal intercostals
- Quiet Inspiration- diaphragm expands causing a negative pressure which draws in air
-
Diaphragm is
primary muscle
- affected by positions- can get in more air if upright
- Upper intercostals may show continuous active
- Scalenes may be active to elevate 1st rib
-
Quiet Expiration– recoil causes a positive pressure
which forces air out of the lungs
- Passive process due to relaxation of diaphragm and elastic recoil of lungs
-
deep inspiration
- Increased activity in diaphragm and intercostals
- Quadratus lumborum fixes last rib
- Accessory muscles-
hypertrophy of these muscles in COPD
- Scalenes and SCM elevate 1st rib and sternum
- Serratus posterior superior elevates ribs
- Erector spinae extends Thoracic spine to increase width of intercostal spaces so greater range for rib movement
-
Deep expiration- increase intra-abdominal pressure
forcing diaphragm up and drawing lower ribs down and medially
- Accessory muscles- abdominals (especially obliques and transversus)
- internal intercostals and latissimus dorsi may also help by depressing rib cage and decreasing thoracic volume
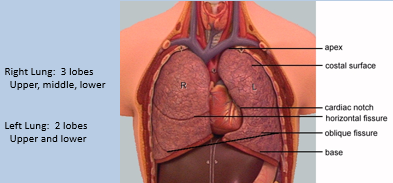
physical components of the lungs
-
pleurae- visceral (outer surface
of lungs) and parietal (inner surface
of chest wall) membranes that cover the
lungs
- pleural effusion- fluid stuck between the lungs and chest wall
- Parenchyma – substance of the lung, porous/spongy
- Cone shaped – apex (top of lungs near clavicle), base (bottom near T10)
- 3 borders (anterior, posterior, and inferior) and 2surfaces (costal and medial)
- right lung: 3 lobes (superior, middle, inferior) separated by fisures
- left lung: 2 lobes (upper and lower) with cardiac notch
- Hilus – point at which the nerves, vessels, and primary bronchi penetrate the parenchyma
- Enter at the Roots – principal bronchus, pulmonary artery, pulmonary veins, bronchial arteries/veins, pulmonary nerve plexus, lymph vessels
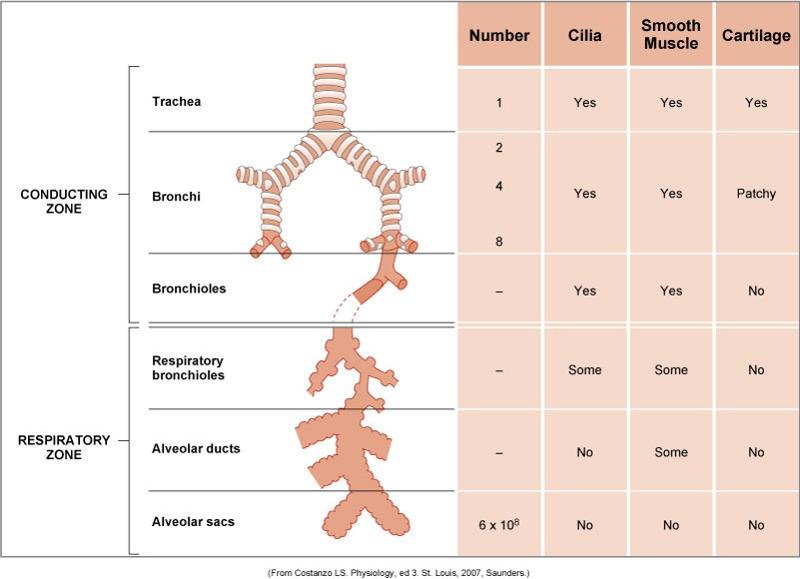
respiratory system
- Upper Respiratory Tract
- Nose- warm and filter air coming in, humidification
- Pharynx- throat (5-6 in long tube
- Larynx- houses vocal chords, controls airflow (important for cough)
- Lower Respiratory Tract
- Tracheobronchial Tree – conducting airways
- Trachea- tube that separates into bronchi
- Main stem/lobar bronchi
- Segmental/ subsegmental bronch
- Terminal respiratory ( Acinar ) units- alveoli where gas exchange takes place
- Innervation of the lungs- can be painful if there is trauma to that area
intercostal nerves
- VPR of first 11 pairs of thoracic nerves
- run along
costal grooves with intercostal vessels
- lying between internal and innermost intercostals
- give
rise to lateral cutaneous branches
- pierce external intercostal muscle near midaxillary line and then external intercostal membrane and pectoralis major
- ends as anterior cutaneous nerves to chest (upper 5 nerves)
- lower 6 VPR nerves become cutaneous for abdomen wall
- upper 5 VPR nerves supply chest wall muscles
intercostal arteries
-
Posterior intercostal arteries
- first 2: arise posteriorly from supreme intercostal artery (from subclavian)
- lower 9: arise posteriorly from thoracic aorta
- Anterior intercostal arteries- Arise anteriorly from internal thoracic artery (branch of subclavian)
- Posterior & anterior intercostal arteries anastomose with each other
pelvic inlet
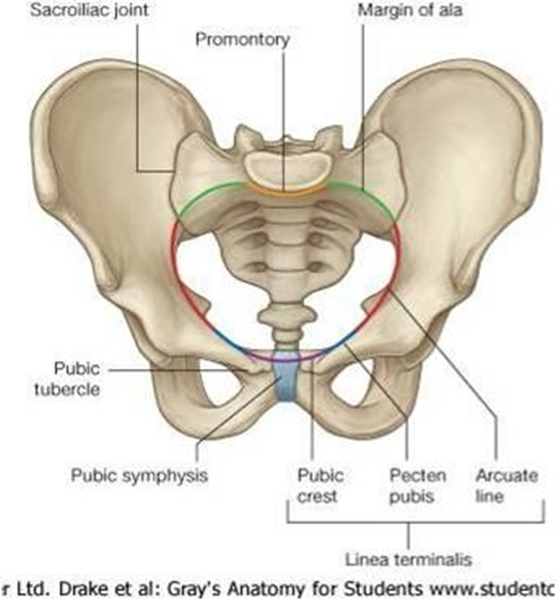
measured when women give birth to see if they can deliver vaginallly
transverse diameter wider in AP direction than males
Borders
- Promontory
- Ala of Sacrum
- linea
terminales
- Arcuate Line
- Pecten Pubis (Pectineal Line)
- Pubic Crest
pelvic outlet
Borders
- Pubic Arch
- Ischiopubic Rami
- Ischial Tuberosities
- Sacrotuberous Ligamen
- Coccyx
pelvic gender differences

Male
- Narrower
- Heart-Shaped Pelvic Inlet
- Iliac Crests are Higher and More Pronounced
- smaller pelvic outlet
Female
- Open, Circular, larger Pelvic Inlet
- Broader Sciatic Notch
- More Outward Flare of the Iliac Crests
pelvic shapes
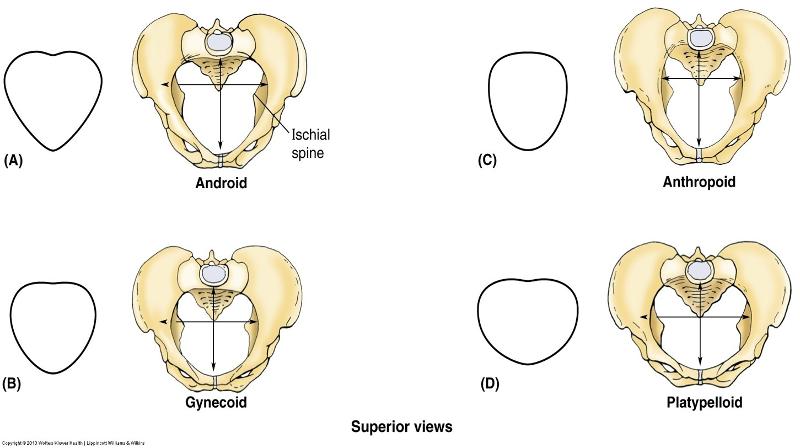
Gynecoid is most common in females
anthropoid and platypelloid are most common in females
superficial and deep muscles of pelvic diaphragm and innervations from sacral plexus
Superficial- sexual
- Ischiocavernosus- support pelvic viscera
- Bulbospongiosis/Cavernosus
- male: Contributes to erection/ejaculation; also aids in emptying urethra
- female: Compresses vestibular bulb and constricts vaginal orifice
-
Compressor (Sphinctor)
Urethrae
- Male: Compresses urethra to maintain urinary continence
- Female: Compresses urethra and Vagina to maintain urinary continence
-
Transverse Perineal
- Superficial- fixes perineal body
- Deep
Deep- support
- Levator Ani- pudendal nerve (anterior division sacral plexus S2-4)
- Puborectalis- Supports & aids continence of rectum by maintaining anorectal angle
- Pubococcygeus- support pelvic viscera
- Iliococcygeus- support pelvic viscera
- Pubovaginalis- Supports anterior pelvic viscera
-
Coccygeus- support
pelvic viscera
- not part of levator ani muscles
-
Obturator
Internus-nerve to obt internus and gemellus superior
(Ant div L5,S1)
- Lateral rotator and abductor of the hip
- Piriformis
function of the pelvic diaphragm
- dynamic support of the pelvic viscera
- tonically active to help maintain fecal an urinary continence
- Actively
Recruited Under Conditions of Intra-Abdominal Pressure to Maintain
Continence
- Forced Expirations (laugh, cough, sneeze, lift)- pelvic floor moves down with diaphragm during inspiration and up during expiration
- Relaxation Required for Urination and Defecation
5 S's of function
- Support &
- Stability- for everything that sits above these muscles (organs, bladder, “core stability”)
- Sexual- get and maintain an erection and women’s orgasm
- Sphincter- prevent fecal or urinary continence
- Sub-pump function- helps pump blood back into circulation
key points in pelvic floor pt
- The Pelvic Floor has a range of motion (ROM)
- 1/4, 1/2, 3/4, and Full ROM (Closure at the Vagina)
- Reliant upon patient’s ability to fully contract (Kegel) and fully relax the Levator An
- Lifting up to the pubic bone
- Muscle Strength of the Levator Ani can be Assessed
- Circumferential squeeze and lift both contribute to the grade
- Laycock scale: for manual muscle testing
- 0/5 =no contraction at all (nerve damage)
- 3/5
=circumferential squeeze but no lift
- all that is needed for normal function
- 5/5 =circumferential squeeze and significant amount of lift
- Coordination during functional activity is KEY
Athletica Pubalgia
- A general term describing chronic pubic/inguinal pain
- “High-energy twisting activities where abnormal (extreme) hip
ROM and resultant pelvic motion leads to shearing across the pubic
symphysis or tendinous insertions of the adductors and rectus
abdominus”
- hockey goalies, soccer player
- Often from trunk hyperextension and thigh hyperabduction
- in athletes with strong adductor muscles but relatively weak lower abdominal muscles (transversus abs, int and ext obliques)
- not a sports hernia (when contents of inguinal canal would come out of canal)
osteitis pubis
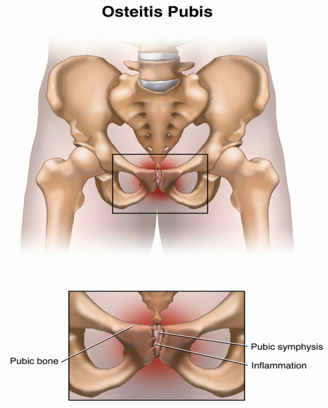
- Inflammation of the Pubic Symphysis and surrounding muscle insertions in athletes
- very central pain, tender to palpation
- men have more stable SI joints, so they are more likely to have shearing in symphysis (women have more SI joint dysfunction)
- Sometimes seen prior to athletica pubalgia or “sports hernia”
rectus diastasis
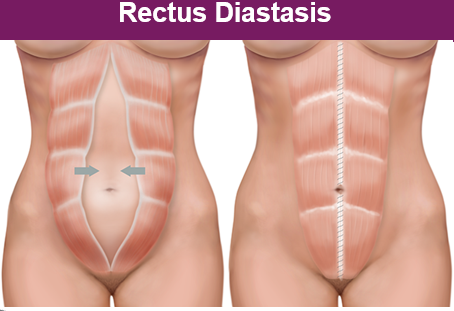
- Commonly seen in women after pregnancy or men with “beer
bellies”
- want to separate rectus abdominis to make room for
baby but it should close again soon after, but may last long
after delivery
- less common in women who exercise regularly and have strong abdominals
- Predisposition due to hormonal and biomechanical changes
- up to a 2 finger width separation is normal
- want to separate rectus abdominis to make room for
baby but it should close again soon after, but may last long
after delivery
- Muscle wall has been repeatedly stretched-creates a structural deficit at the abdominal wall
- Can occur above, at, and/or below umbilicu
- core is low pressure so major increases in pressure will go through the split in the rectus (weakest point)
- Appropriate postural strength and coordination of functional movement strategies are key to closure
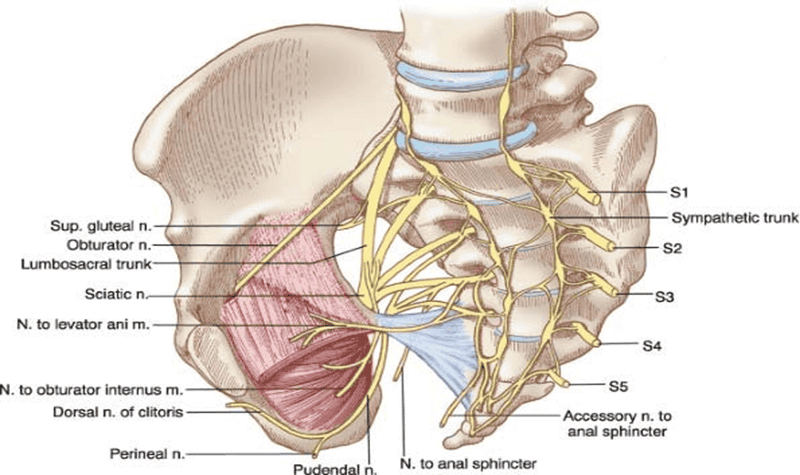
pudendal nerve entrapment (pudendal neuralgia)
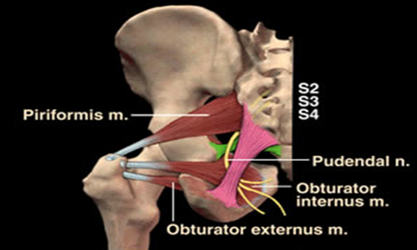
- exits through greater sciatic foramen then through lesser
sciatic foramen then splits into 3 branches:
- dorsal clitoral/penis, perineal, inferior rectal
- many places the pudendal nerve can get trapped, but
generally between:
- sacrospinous and sacrotuberous ligaments
- tension/contraction of the obturator internus could compress the pudendal nerve
- ADLs like sitting can put pressure on that area and compress the nerve
bony thorax
- covers and protects the major organs of the cardiopulmonary system
- consists of:
- sternum (manubrium, body and xiphoid)
- ribs (true ribs= 1-7,
false ribs 8-10, floating ribs 11-12)
- rib fractures are very painful since ribs are always moving with breathing and there is a rich blood and nerve supply
mediastinum
- Lies between right and left pleura of lungs
- Contains all thoracic viscera (heart, great vessels, trachea, esophagus) except the lungs
- Mediastinal shift- collapse of one side of the lungs can cause the mediastinum to move further to one side
tissues of the heart
- Pericardium – outermost layer, covers heart surface and anchors heart to chest
-
Myocardium-
muscular midwall of heart, facilitates pumping action; contractile
elements
- thickness is related to resistance heart must pump against (hypertrophy= less efficient)
- Myocardial cells- 3 unique characteristics (rhythmicity, automaticity, conductivity), only cells in the only that can do those functions
- Endocardium-thin layer lining inside of cardiac chambers, continuous with inner heart structures and blood vessels
functions of myocardial cells
3 unique characteristics, only cells in the only that can do these functions
- automaticity- contract without stimulus
- rhythmicity- beat rhythmicly
- conductivity- transmit impulse
chambers of the heart
- Right atrium-receiving chamber for deoxygenated blood from systemic circulation.
- Right ventricle-pumps blood through pulmonary circulation.
- Left atrium-receiving chamber for oxygenated blood from the lungs.
- Left ventricle-propels blood to the systemic circulation
valves of the heart
- keep blood moving in 1 direction
- dysfunction= heart murmur and a more turbulent, less efficient valve
-
Atrioventricular valves:
- Mitral Valve- between LA and LV, composed of 2 leaflets (bicuspid valve)
- Tricuspid valve-between RA and RV, composed of 3 leaflets
- Semilunar Valves (3 cusps):
- Pulmonary valve-between RV and pulmonary artery.
- Aortic valve-between LV and aorta
conduction system of heart
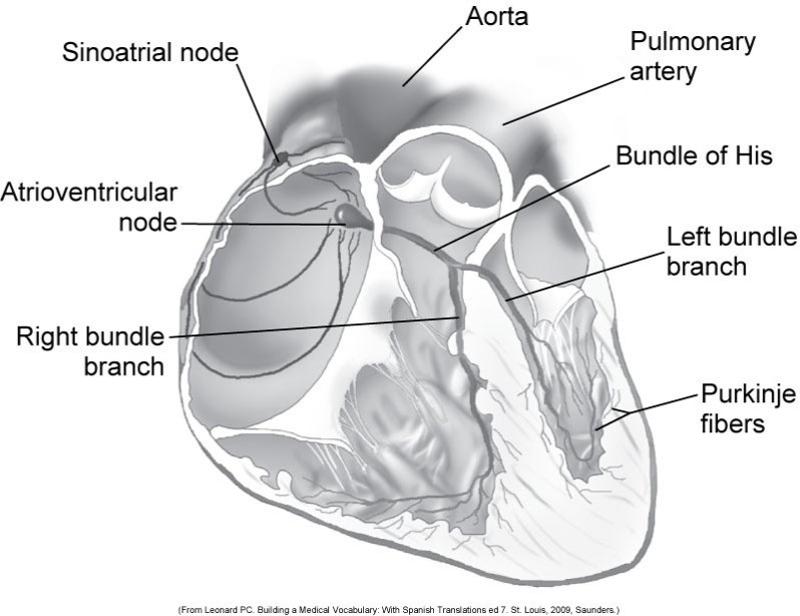
how impulse is conducted through heart
- Sinoatrial (SA) node- primary pacemaker (60-100 bpm)
- Atrioventricular (AV) node- secondary pacemaker
- Bundle of His- separates into right and left bundles
- Purkinje- separated into fibers into each ventricle
Innervation
- Parasympathetic – vagus nerve
- Sympathetic – epinephrine and norepinephrine
cardiac and pulmonary vessels
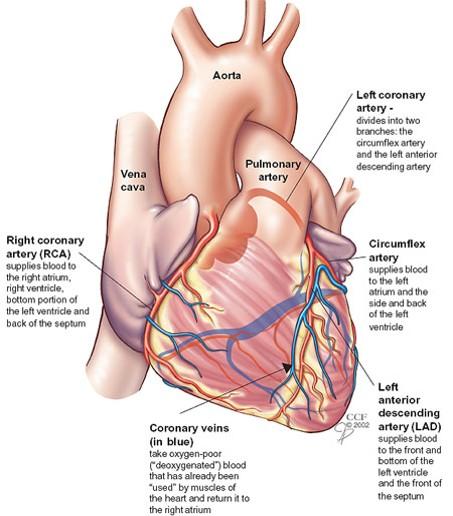
- Aorta
- Aortic sinuses
- Coronary arteries- supply blood to heart muscles
-
Right Coronary Artery
- Arises from right anterolateral surface of the aorta
- Descends into coronary sulcus
-
Left Coronary Artery
- Originates from left anterolateral aspect of the aorta
- Splits into the anterior interventricular (left anterior descending) and circumflex
- Brachiocephalic trunk
- Left common carotid artery
- Left subclavian
- Pulmonary Artery- right ventricle to lungs
- Pulmonary Veins- lungs to left atrium, No valves
- Vena cava- Superior vena cave ends into right atrium
- Cardiac veins- drain into coronary sinus
- Arteries- Wall composed of elastic and fibrous connective tissue, smooth muscle
- Smooth muscle receives autonomic stimulation from alpha-receptors
- Arteries to arterioles to capillary beds
- Endothelium–Functions include filtration, permeability,
vasomotion, clotting, and inflammation
- damage (high BP, smoking) makes it more permeable to cells- atherosclerotic changes
-
Veins- Thinner walls, larger diameter, less elastic
tissue
- Valves create unidirectional flow (problems= varicosities)
- Blood is transferred back to heart through muscle pump