Recovery Room Record
Designed to care for patients immediately after surgery or anesthesia. TJC requires this form to include patient's condition and level of consciousness when entering and leaving the unit; vital signs; status reports of infusions, surgical dressings, tubes, catheters, or drains; and any treatment provided in the unit.
Pathology Report
Documents tissue examinations that may be microscopic in addition to being macroscopic (gross). The tissue or object is identified, a clinical diagnosis is provided, and an opinion requested.
Operative Report
Must be included in records of all patients who undergo surgery. Top portion provides identifying data, including the names of the surgeon and any assistants, and the date, duration, and name of the procedure. A postoperative diagnosis is required and a preoperative diagnosis is also desirable for comparison. Body of report contains full description of the surgical approach, normal and abnormal findings, organs explored, procedures, implants, ligatures, sutures, and the number of packs, drains, and sponges used, and the condition of the patient at the conclusion of surgery.
Discharge Summary
Reviews the patient's course. Begins with the reason for admission and includes chronological descriptions of significant findings from examinations, tests, procedures, and therapies performed along with the patient's response. Details regarding discharge are also recorded, including the condition on discharge related to the condition on admission and follow-up instructions specifying medications, level of physical activity, diet, follow-up care, and patient teaching. Attending physician records this.
MDS
Minimum Data Set
Standardized, comprehensive assessment instrument that CMS requires be completed for residents of skilled nursing facilities. Collects administrative and clinical information. States have the option of having supplemental data collected with the approval of CMS.
•CMS requires this to be completed
•Collects
administrative and clinical information
•Must be collected
at
•Start of therapy
•Change of therapy
•End of
therapy (discharge)
•Significant change in status assessment
CMS uses the data for Long-Term Care.
UHDDS
Uniform Hospital Discharge Data Set
Promulgated by the secretary of the Department of Health, Education, and Welfare in 1974, as a minimum, common core data on individual hospital discharges in the Medicare and Medicaid programs.
Abbreviation List
An official list of approved abbreviations maintained by healthcare organizations, to avoid misunderstandings from either poor handwriting or the fact that many abbreviations have more than one meaning.
Abbreviation, Acronym, and Symbol Rules
If more than one definition exists, the preferred approach is to avoid the abbreviation entirely.
TJC prohibits the use of dangerous abbreviations, acronyms, and symbols in patient records.
Progress Notes
Interval statements that document the patient's illness or condition and response to treatment as specifically as possible. Person writing the notes is responsible for recording observations about the patient's progress and response to treatment from the perspective of his profession.
Incident Report
Reports completed by health care professionals when an incident occurs. Nonjudgmental factual accounts of the event and any consequences. Used to correct problem-prone areas and in preparation for possible legal action.
Administrative documents that are not included in the patient's record.
Interdisciplinary Patient Care Plan
The foundation around which patient care is organized. Contains input from the unique perspective of each discipline involved in patient's care. Includes assessment, statement of goals, identification of specific activities or strategies to achieve those goals, and periodic assessment of goal attainment. Valuable tool in evaluating both individual patient care and overall organizational patient care performance.
Problem List
Includes specified clinical problems, a diagnosis, a summary and stressor exposure. It's an ongoing list of clinically significant health status events and factors (resolved and unresolved) in a patient's life. It is a master list of all a patient's problems or diagnoses.
In a POMR, the problem list includes titles, numbers, and dates of problems and serves as a table of contents of the record.
Transfer Record or Form
When a resident is transferred to a facility, this record provided by the hospital, physician, or other facility should accompany the patient or follow immediately. The form facilitates the continuity of care and should include reason for admission, diagnosis, current medical information, and rehabilitative potential.
Prenatal Record
or
Antepartum Record
Begins in the office or clinic of the OB or midwife. Ideally started early in pregnancy, record includes a comprehensive history and physical examination with particular attention to menstrual history, reproductive history - including live births and abortions, a risk assessment, and attendance at any birth classes.
Includes initial and subsequent history, physical examination, recording of clinical information, and monthly visits up to 28 weeks of gestation, biweekly visits to 36 weeks gestation, and weekly visits until the time of delivery, and routine chemical urinalysis.
Labor and Delivery Record
This record tracks the patient form admission through delivery to the postpartum period. Evaluation is made by physician including updated history, data on contractions, status of membranes, presence of significant bleeding, time and content of the patient's last intake of food or fluid, drug intake and allergies, choice of anesthesia, and plans to breast- or bottle-feed. Mother and baby are monitored frequently. At delivery, details regarding the mother are recorded and the neonate is described - Apgar score, sex, weight, length, onset of respiration, abnormalities, and treatment to the eyes.
Postpartum Record
Includes information about the condition of the mother after delivery. Special attention is given to assessing the lochia and condition of the breasts, fundus, and perineum as well as the postoperative status.
History and Physical Time Frames
TJC requirements: Comprehensive H&P must must be completed and available within 24 hours - sooner if surgery is to be performed. An interval H&P is permitted as long as patient is admitted within 30 days for the same condition with any changes noted.
Disease Index
A numerically sequenced list of diseases and conditions diagnosed in hospital patients. This is a case finding source for the cancer registry that is compiled from these codes. A listing in diagnostic code number order.
Number Control Index
Identifies new health record numbers and the patients to whom they were assigned.
Physician's Index
Identifies all patients treated by each doctor. A listing of cases in order by physician name or number.
Because information contained in the physician's index is considered confidential, identification codes are often used rather than physicians' names.
Patient Index
Links each patient treated in a facility with the health number under which the clinical information can be located.
OASIS
Outcome Assessment Information Set
Set of data elements that represent core items of a comprehensive assessment for an adult home-care patient. It is used to measure patient outcomes in outcome-based quality improvement. This assessment is performed on every patient who receives services from home-health agencies that participate in the Medicare or Medicaid programs. This assessment is the basis of the Home Health Prospective Payment System.
DEEDS
Data Elements for Emergency Department Systems
Set of data elements that represent core items of a comprehensive assessment for an emergency department.
Interdisciplinary Plan of Care
The foundation around which patient care is organized because it contains input from the unique perspective of each discipline involved in the patient's care. Includes an assessment, statement of goals, identification of specific activities or strategies to achieve those goals, and periodic assessment of goal attainment.
ONC
Office of the National Coordinator for Health InformationTechnology
In 2004, President Bush created this position. This office and role within Health and Human Services (HHS) is charged with providing national leadership in support of government and private efforts to develop the standards and infrastructure to more effectively use information technology to achieve quality health care and to reduce health care costs. This person reports to the Secretary of the HHS.
OSHA
Occupational Safety and Health Administration
This group is responsible for developing standards and regulations and conducting inspections and investigations to determine compliance, and it proposes corrective actions for noncompliance in matters related to occupational safety and health.
SOAP What is the S?
Subjective - Records what the patient states is the problem.
Describes the patient’s current condition in narrative form. This section usually includes the patient’s chief complaint, or reason why they came to the physician.
SOAP What is the O?
Objective - Records what the practitioner identifies through the history, physical examination, and diagnostic tests. Documents objective, repeatable, and traceable facts about the patient’s status.
Includes: Vital signs; Findings from physical examinations, such as posture, bruising, and abnormalities; Results from laboratory; Measurements, such as age and weight of the patient.
SOAP What is the A?
Assessment - Combines the subjective and objective into a conclusion. The Physician’s medical diagnoses for the medical visit on the given date of a note written.
SOAP What is the P?
Plan - What approach is going to be taken to resolve the problem. This describes what the health care provider will do to treat the patient – ordering labs, referrals, procedures performed, medications prescribed, etc.
MPI
Master Patient Index
Index that identifies all patients who have been treated by the facility and lists the number associated with the name.
Cross-references the patient name and medical record number.
Operation Index
A list of all procedures that have been performed in a facility.
Point-of-Care Service and Documentation
Allows caregivers to capture and input data where health care service is provided and may be done at the time of patient care. This system can collect data directly from monitoring devices such as those in intensive care units.
It ensures that appropriate data are collected.
Data Comprehensiveness
All data items are included. The entire scope of the data is collected, and document intentional limitations. Denotes that all data items are included.
Data Granularity
The relative degree of detail, specificity, or size of components; in health care, _____ is often used to describe the specificity with which a diagnosis is made or how much detail is included in the workflow and process being mapped.
The attributes and values of data should be defined at the correct level of detail.
Data Precision
Data values should be just large enough to support the application of the process.
Data Accuracy
Data are the correct values and are valid. The data represent what was intended or defined by their official source, are objective or unbiased, and comply with known standards.
Reliability
Refers to consistency of data.
Timeliness
Refers to data being available within a time frame helpful to the user.
Validity
Meaning the right thing was measured.
Accuracy. The accuracy of data.
Commission on Accreditation of Rehabilitation Facilities
CARF
Independent accrediting agency for rehab facilities.
Mission is to promote the quality, value, and optimal outcomes to people with disabilities.
Sets and maintains standards directed at improving quality of care, conducting research, identifying competent organizations that provide rehabilitative services, and providing an organized forum in people served, providers, and others can participate in quality improvement.
This private, not-for-profit organization is committed to developing and maintaining practical, customer-focused standards to help organizations measure and improve the quality, value, and outcomes of behavioral health and medical rehabilitation programs.
Federal Register
A Monday-Friday publication of the National Archives and Records Administration that reports regulations and legal notices issued by federal agencies, presidential proclamations and executive orders, and other documents as directed by law or public interest.
CMS publishes both proposed and final rules for the Conditions of Participation for hospitals in this.
Electronic Document-Management System
EDMS System
The method used to maintain and combine paper and electronic records.
One advantage is that it can help manage tasks because it can facilitate various functions that must be performed, often simultaneously or in a specific sequence.
Ex: When patient is discharged, a notification is sent to an analyst that record is ready for analysis and coding.
Computer Prescriber Order Entry
CPOE
Electronic systems that support physicians and other applicable licensed healthcare professionals in developing and documenting instructions for the care of the patient, including the ordering of medications, diagnostic studies, food and nutrition, nursing services, and treatments.
These systems contain some clinical decision support functionality that provides the user with standard order sets that reduce data entry time; alerts about the possibility of drug interactions, allergic reactions, or a potential overdose; warnings for potential duplicate diagnostic tests and therapies; reminders about the need to renew or discontinue an order; and other relevant information.
Regional Health Information Organization
RHIO
Organizations that are working together to develop a means of sharing health information for patient care and other uses, typically within a geographic area.
Part of the development of a national health information infrastructure.
Omnibus Budget Reconciliation Act of 1987
OBRA 1987
It brought attention and support to the production and dissemination of scientific and policy-relevant information that improves quality, reduces cost, and enhances effectiveness of health care and established the Agency for Healthcare Research and Quality (AHRQ).
Required CMS to develop an assessment instrument to standardize the collection of SNF patient data. This instrument is the resident assessment instrument (RAI) and includes the MDS 3.0.
Data Dictionary
A descriptive list of the data elements to be collected in an information system or database whose purpose is to ensure consistency of terminology.
Data Element
An individual fact or measurement that is the smallest unique subset of a database.
Ex: Age, gender, insurance company, or BP
Data Set
A list of recommended data elements with uniform definitions that are relevant for a particular use.
Accession Register
A number assigned to each case as it is entered into a cancer registry.
Quantitative Analysis
Involves checking for the presence or absence of necessary reports and/or signatures
Qualitative Analysis
Involves checking for documentation consistency - comparing what was written to what was actually done.
Utilization Review
The process of evaluating the efficiency and appropriateness of health care services according to predetermined criteria.
R-ADT System
Registration-Admission, Discharge, and Transfer System
A type of Administrative information system that stores demographic and insurance information and performs functionality related to registration, admission, discharge, and transfer of patients within the organization.
Tracks when a patient was registered, admitted, discharged and/or transferred.
ORYX Initiative
A Joint Commission initiative that supports the integration of outcomes data and other performance measurement data into the accreditation process.
Goal if the initiative is to foster a comprehensive, continuous, data-driven accreditation process for healthcare facilities. They want to integrate outcomes and other performance measures into the accreditation process through data collection about specific core measures.
Uses nationally standardized performance measures to improve the safety and quality of healthcare.
Core Performance Measures
Considered tools that provide an indication of an organization's performance and used by the JC within the ORYX initiative. Used to assess how well healthcare organizations provide care.
Used by Joint Commission, CMS, and healthcare plans like Blue Cross.
Used to determine where to focus QI activities and accreditation surveys.
Sets include:
- Acute Myocardial Infarction
- Heart Failure
- Pneumonia
- Surgical Care Improvement Project
- Pregnancy and Related Conditions
- Hospital Outpatient Department
- Children's Asthma Care
- National Hospital Inpatient Quality Measures-Hospital-Based Inpatient Psychiatric Services
Database
Contains the H&P in a PMOR (problem-oriented medical record)
Initial Plan
Describes diagnostic, therapeutic, and patient education plans.
Straight Numeric Filing Systems
Records are arranged consecutively in ascending numeric order. The number assigned to each file in the health record number.
Terminal-Digit Filing System
Considered the most efficient system. Good for facilities with a heavy record volume. Allows for even file expansion .
The last digit or group of digits is the primary unit used for filing, followed by the middle unit and the last unit of numbers.
Ex: 44-37-98
98 is the primary unit, 37 is the secondary unit, and 44 is the tertiary number.
98 = file section, 37 = shelf number, 44 = folder number
Middle-Digit Filing System
Primary digit is the middle unit of numbers, the secondary is the unit to the left, and the tertiary is the last unit.
Ex: 44-37-98
37 is the primary unit, 44 is the secondary unit, and 98 is the tertiary number.
37 = file section, 44 = shelf number, 98 = folder number
Serial-Unit Numbering System
Combines the strengths of both the Serial and the Unit Numbering Systems. Numbers are assigned in serial number (the patient gets the next available number at each encounter). However, the old record is brought forward and filed under the new number creating a unit record.
Serial Numbering System
A patient receives a unique numerical identifier for each encounter or admission to a healthcare facility. Numbers are issued in a series with each patient receiving the next available number in the series.
Each encounter is stored under its own number. Retrieval of all records is difficult and inefficient.
Unit Numbering System
Most common in large healthcare facilities. The patient receives a unique health record number at the time of the first encounter. This is the patient's number for each subsequent encounter thereafter.
In case of duplicate charts, all charts should be moved to first number given to the patient on his/her first encounter with facility.
Conditions of Participation requires patient health records are kept for how long?
5 years
Roll Microfilm
Open reel (roll) microfilm is either 16mm or 35mm film that wraps around a spool. It usually comes in 100foot lengths, though it can come in lengths of up to 215 feet.
- Open reel film has the following characteristics:
- It is the oldest form and also the least expensive because it can store a large amount of information in a small place
- It provides a high measure of file security because images can be detached only by cutting the film
- It can be indexed simply with target sheets or odometer readings or by sophisticated high speed retrieval with blips, bar codes, or sequential numbering
Cartridge Microfilm
Roll microfilm that has been placed in a compact plastic holder, which is self-threading in compatible retrieval equipment.
- It threads onto a reader and is handled more easily
- It allows faster access to information
- It can take advantage of sophisticated index coding
Jacket Microfilm
A microfilm jacket is a fiche-sized acetate or polyester carrier that contains three to eight sleeves or channels into which strips or single images of either 16mm or 35mm roll micro-film are inserted.
One jacket can hold up to sixty images. The top of the jacket contains an index area,which can be typed or written on. A jacket allows a file to be updated—new material can be inserted into the unused channels as it is filmed.
- It can be used for records that are frequently updated
- The area at the top of the fiche allows easy access and file reference
- Jacket to fiche duplication is inexpensive
- The jacket protects the microfilm while it is being used
- Microfiche readers are inexpensive
- It provides quick access to the records
Outguide
When a file is removed from the system, this is inserted in its place to alert that the file is being used. It has a small pocket into which a charge out slip can be placed to track the location of the removed file. The large pocket is used to hold documents and information that accumulates while the file is out.
File Guide
This is used to break large numbers of records into smaller groups so you can find them faster. Like signposts on a highway, these stand out from the folders to signal major divisions in the filing system.
Database Management System
DBMS
A collection of computer programs that controls the creation, maintenance, and use of a database. It allows different application programs to access the database. It maintains the data definitions (data dictionary) for all the data elements in the database and enforces data integrity and security constraints.
Hypertext Markup Language
HTML
A standardized system for tagging text files to achieve font, color, graphic, and hyperlink effects on World Wide Web pages.
Structured Query Language
SQL
Used to store and retrieve data in relational databases. It gives the information system the ability to query and report on data and to insert, update, and delete data from the data base.
A common language used in data definition and data manipulation.
A fourth generation computer language that includes both Data Definition Language (DDL) (a standard for commands that define the different structures in a database. DDL statements create, modify, and remove database objects such as tables, indexes, and users) and Data Manipulation Language (DML) (a family of syntax elements similar to a computer programming language used for selecting, inserting, deleting and updating data in a database) components and is used to create and manipulate relational databases.
Extensible Markup Language
XML
A markup language that defines a set of rules for encoding documents in a format which is both human-readable and machine-readable. Designed to describe data, not to display data.
Executive Information Systems
EIS
A type of decision support system used by high-level managers that draws data from the organization's other databases.
An information system designed to combine financial and clinical information for use in the management of business affairs of a healthcare organization.
A type of management information system intended to facilitate and support the information and decision-making needs of senior executives by providing easy access to both internal and external information relevant to meeting the strategic goals of an organization.
Provides information on the census, updates the master patient index, and distributes demographic data.
Management Information System
MIS
Collects, stores, modifies, and retrieves the transactions of an organization to help middle managers make decisions about their departments' objectives.
Data might include
- Admission, discharge, and transfer data
- Data on the number of dictated reports, coded records, filed records, and incomplete records
- Structured reports
- Production schedules
- Productivity analysis
Financial Information System
FIS
The accounting/financial programs and data necessary for running a healthcare facility.
Include functions such as payroll preparation and accounting; accounts payable; patient accounting, including billing and accounts receivable processing; cost accounting; general ledger accounting; budgeting; and financial statement preparation.
Internet
An international network of computer servers that provides individual users with communications channels and access to software and information repositories worldwide.
Intranet
A computer network that uses Internet Protocol technology to share information, operational systems, or computing services within an organization.
Extranet
A systems of connections of private Internet networks outside an organization's firewall that uses Internet technology to enable collaborative applications among enterprises.
Clinical Information System
CIS
A category of a healthcare information system that includes systems that directly support patient care.
Designed primarily to support patient care by providing healthcare practitioners with access to timely, complete, and relevant clinical information that is used to diagnose, treat, and manage patient care.
Interfaced System
In computing, an interface is a shared boundary across which two separate components of a computer system exchange information. The exchange can be between software, computer hardware, peripheral devices, humans and combinations of these.
A large collection of clinical information systems and hospital information systems that are designed to share data without human or technical intervention.
Integrated System
In engineering, system integration is defined as the process of bringing together the component subsystems into one system and ensuring that the subsystems function together as a system.
Online Analytical Processing
OLAP
A data access architecture that allows the user to retrieve specific information from a large volume of data.
Performs multidimensional analysis of business data and provides the capability for complex calculations, trend analysis, and sophisticated data modeling.
Clinical Data Repository
CDR
A central relational database that focuses on clinical information.
Helps manage data from many different sources, ancillary systems in the hospital, or other provider settings as well as from direct entry of structured data by the clinician. It can make this data readily available and process this data in CDS (clinical decision support).
Limited to data retrieval.
Supports the management of data for an EHR.
Contains structured and unstructured data. Database optimized for for online transaction processing (OTAP). Transactions relating to patient care - lab results, enter order, post vital signs, record meds administered.
Ex: You are working with a database that is created from multiple databases being stored in a single database. Good for laboratory, pharmacy, and radiology data.
Clinical Data Warehouse
CDW
A database that makes it possible to access data from multiple databases and combine the results into a single query and reporting interface.
Contains structured data only. Database optimized for online analytical processing (OLAP). Analysis of data relating to a population of patients - aggregate data to identify patterns, compare measures, data mining, predictive modeling.
Application Service Provider Model
A business that provides computer-based services to customers.
A third party service company that delivers, manages, and remotely hosts standardized applications software via a network through an outsourcing contract based on fixed monthly usage or transaction-based pricing.
Good for large facilities.
Light Pen
A handheld, penlike photosensitive device held to the display screen of a computer terminal for passing information to the computer.
A handheld, light-emitting device used for reading bar codes.
International Classification on Functioning, Disability, and Health
(ICF)
A classification system that is structured around
- Body functions and structure
- Domains of activities and participation
- Environmental factors that interact with all these components
Systematized Nomenclature of Human and Veterinary Medicine international
(SNOMED)
A coding system, controlled vocabulary, classifications system, clinical reference terminology, and thesaurus.
Based on SNOP.
Systematized Nomenclature of Pathology
(SNOP)
Organizes information from surgical pathology reports.
Logical Observation Identifiers, Names and Codes
(LOINC)
Used to represent laboratory and clinical measurements, survey questions, clinical documents, and diagnostic reports.
National Practitioner Data Bank
A data bank established by the federal government through the 1986 Healthcare Quality Improvement Act that contains information on professional review actions taken against physicians and other licensed healthcare practitioners, which healthcare organizations are required to check as part of the credentialing process.
Healthcare Quality Improvement Program
History
Instituted in 1992 by CMS. Original mission was to promote the quality, effectiveness, and efficiency of services to Medicare beneficiaries. It was to
- Monitor and improve quality of care
- Communicate with beneficiaries, healthcare providers, and practitioners
- Promote informed health choices
- Protect beneficiaries from poor care
Healthcare Quality Improvement Program
Today
Today's approach to improving health of beneficiaries involves the analysis of patterns of care to promote changes in the healthcare delivery system.
Now focuses on 6 clinical priority areas:
- Acute myocardial infarction
- Breast cancer
- Diabetes
- Heart failure
- Pneumonia
- Stroke
MEDPAR
Medicare Provider Analysis and Review
A collection of data from reimbursement claims submitted to the Medicare program by acute care hospitals and skilled nursing facilities that is used to evaluate the quality and effectiveness of the care being provided.
Made up of acute care hospital and skilled nursing facility claims for all Medicare claims. It is frequently used for research on topics such as charges for particular types of care and MS-DRGs.
The limitation of this data for research purposes is that the file contains only Medicare patients.
Vital Statistics
Data related to births, deaths, marriages, and fetal deaths.
RxNorm
A clinical drug nomenclature developed by the FDA, the Department of Veterans Affairs, and HL7 to provide standard names for clinical drugs and administered dose forms.
Systematized Nomenclature of Medicine Clinical Terminology
(SNOMED CT)
A standardized vocabulary, sometimes referred to as a controlled reference terminology.
A systematized, multiaxial, and hierarchically organized nomenclature of medically useful terms.
A comprehensive clinical terminology.
The most comprehensive controlled vocabulary.
Standard Nomenclature of Disease and Operation
SDNO
The first medical nomenclature to be universally accepted in the United States
Unified Medical Language System
UMLS
A project sponsored by the National Library of Medicine.
Provides a way to integrate biomedical concepts from a variety of sources to show their relationships. This process allows links to be made between different information systems for purposes such as electronic health record systems.
Meant to be read by machines - not humans.
CPT
Current Procedural Terminology
A nomenclature of codes and medical terms that provides standard terminology for reporting physicians' services for third-party reimbursement.
Can be used to gather stats for outpatient surgical services.
HCPCS
An alphanumeric classification system that identifies healthcare procedures, equipment, and supplies for claim submission purposes.
An umbrella for all the coding levels below it.
Level I HCPCS Codes
Maintained by AMA - Called CPT codes
CPT Codes used for physicians' services and hospital outpatient coding. Identifies surgical procedures, office visits, lab services.
Updated annually, effective January 1.
5 Numeric Characters
The umbrella for Category I, II, and III codes
Level II HCPCS Codes
Maintained by CMS - Called HCPCS codes or National Codes
Used for reporting medical services not covered in CPT - injectable drugs, chiropractic services, dental procedures, ambulance services, prosthetic devices, supplies, durable medical equipment, and selected provider services.
Updated annually, effective January 1.
Alpha-numeric Codes Beginning with A-V
Category I Codes
Include the following sections
- E & M
- Anesthesia
- Surgery
- Radiology
- Pathology/Laboratory
- Medicine
Category II Codes
Supplemental performance tracking codes
Use is optional
Category III Codes
Temporary emerging technology codes
Discrete Data
Separate and distinct values or observations; for example, patients in the hospital because each patient can be counted.
Continuous Data
Data that can be measured on some scale representing values or observations that have an indefinite number of points along a continuum; for example temperature.
Nominal Data
Values or observations that that can be labeled or named, but not ranked or measured; allow data to be coded, for example 1=Male, 2=Female.
Ordinal Data
Values or observations that can be ranked.
Ex: Patient satisfaction surveys where 1=very satisfied and 5=not satisfied
Reliability
Refers to consistency between users of a given instrument or method.
Validity
Assesses relevance, completeness, accuracy, and correctness. Measures how well a data collection instrument measures what it should measure.
Frequency Polygon
A graphical device for understanding the shapes of distributions. They serve the same purpose as histograms, but are especially helpful for comparing sets of data.
Frequency Distribution
A table or graph that displays the number of times a particular observation occurs.
Examples
- Histogram
- Tables
Inpatient Service Day
Services received by one patient during one 24-hour period.
Daily Inpatient Census
Total number of patients treated during a 24 hour period.
The number of inpatients present at census-taking time each day, plus any inpatients who were both admitted and discharged after the census-taking time.
Daily Census
Total number of patients treated during a 24 hour period.
The number of inpatients present at census-taking time each day, plus any inpatients who were both admitted and discharged after the census-taking time.
Inpatient Census
The number of inpatients present at any one time. A snapshot of one moment in time.
International Classification on Functioning, Disability, and Health
ICF
Approved by World Health Assembly in 2001
Created in 1980 by World Health Organization and was known as International Classification of Impairments, Disabilities, and Handicaps.
Structured around the following broad concepts:
- Body functions and structures (A & P)
- Activities and participation (Individual tasks and life involvement)
- Additional information on severity and environmental factors (problems in body, limitations and restrictions, and physical, social, and attitudinal environment where people live.
National Drug Codes
NDC
Administered by the FDA.
The official data set for reporting drugs used by pharmacies.
Used to maintain drug inventories in pharmacies.
Codes that serve as product identifiers for human drugs, currently limited to prescription drugs, insulin, and a few selected OTC products.
Identifies the vendor, product, and trade package size.
DSM-IV-TR
Glossary of descriptions of mental disorders. All codes are fully compatible with ICD-9 & 10.
Implant Registry
Developed for the purpose of tracking the performance of implants, including complications, deaths, and defects resulting from implants, as well as implant longevity.
Implants
A material or substance inserted into the body.
Ex: Breast implants, heart valves, or pacemakers.
Transplant Registries
There are several types of databases
- Patients who need organs
- Potential donors
- Post-transplant information on recipients and donors
Are often national or even international in scope.
Cancer Registries
The most common type of registry located in hospitals of all sizes and in every region of the country.
There are two types:
Facility-Based which is used primarily for improved patient care, also for understanding of cancer - including causes, methods of diagnosis, and treatments.
Population-Based whose emphasis is on identifying trends and changes in the incidence of cancer within the area.
Cancer Registry Reference Date
The date the registry began accessioning cases.
International Classification of Diseases for Oncology
ICD-O
Used to classify neoplasms according to their site, behavior, morphological characteristics, and how they are graded.
National Library of Medicine
NLM
The world's largest medical library and a branch of the National Institutes of Health.
Produces two databases:
- MEDLINE
- UMLS
MEDLINE
Medical Literature, Analysis, and Retrieval System Online
Best known database from NLM.
Includes bibliographic listings for publications in the areas of medicine, dentistry, nursing, pharmacy, allied health, and veterinary medicine.
ASTM
American Society for Testing and Materials
A system of standards developed primarily for various EHR management processes. Identifies structure and content for the EHR.
A national organization whose purpose is to establish standards on materials, products, systems, and services.
A standards development organization that develops standards for a variety of industries in the US. The _____ Technical Committee on Healthcare Informatics E31 is charged with the responsibility for developing standards related to the EHR. It was created to help communicate that information from one provider to another for referral, transfer, or discharge of the patient.
Trauma Registry
Database on patients with severe traumatic injuries and may be used for performance improvement and research in the area of trauma care.
Birth Defects Registry
Collect information on newborns with birth defects. Provide information on the incidence of birth defects, causes and preventions, trends, improving medical care and target interventions for preventable defects.
Active surveillance systems use trained staff to identify cases in all hospitals, clinics, and other facilities through review of patient records, indexes, vital records, and hospital logs.
READ Codes
A standard terminology for describing the care and treatment of patients.
From the UK's National Health Service's Clinical Terms and is being migrated over to SNOMED CT.
ABC Codes
Five-digit HIPAA compliant alpha codes (e.g., AAAAA) used by licensed and non-licensed healthcare practitioners on standard healthcare claim forms (e.g., CMS 1500 Form) to describe services, remedies and/or supply items provided and/or used during patient visits.
Contain both a short description and an expanded definition of the service, remedy and/or supply item.
SPECIALIST Lexicon
One of three of the UMLS components - Metathesaurus, Semantic Network, and this one.
It includes commonly occurring English words and biomedical vocabulary. The entry for each word or term records the syntactic, morphological, and orthographic information used with associated NLP (Natural Language Processing) tools.
Secondary Data Source
Data derived from the primary patient record.
Examples
- Facility-Specific Indexes
- MPI, Disease, Operation, and Physician Indexes
- Registries
- Disease, Cancer, Trauma, Birth Defects, Diabetes, Implant, Transplant, and Immunization Registries
- National and State Administrative Databases
- MEDPAR File, NPDB, Healthcare Integrity and Protection Data Bank (HIPBD), and State Administrative Data Banks
- National, State, and County Public Health Databases
- National Healthcare Survey, Vital Statistics, Clinical Trials, Health Services Research Databases, NLM, Health Information Exchange, Data for Performance Measurement
Secondary Data
The information that is generated from the patient record.
Why it is collected
- Quality, Performance, and Patient Safety
- Research
- Population Health
- Administration
CPT Level I Modifiers Uses
- Significant, separately identifiable E/M service by the same physician on the same day of a procedure or other service
- Increased Procedural Service
- Anesthesia by a Surgeon
- Multiple Procedures
- Surgical Care Only
- Post-Op Management Only
- Pre-Op Management Only
- Two Surgeons
- Procedure Performed on Infants Less Than 4 KG
- Surgical Team
- Assistant Surgeon or Minimum Assistant Surgeon
- Multiple Modifiers
- Multiple outpatient hospital E/M encounters on the same date
- Bilateral Procedure
- Reduced Services
- Staged or related procedure or service by the same physician during the post-op period
- Distinct Procedural Service
- Discontinued outpatient procedure prior to or after the administration of anesthesia
- Repeat procedure or service by the same or another physician
- Unplanned return to the OR by the same physician following initial procedure for a related procedure during the post-op period
- Unrelated procedure or service be the same physician during the post-op period
- Repeat clinical diagnostic lab test
CPT Level II Modifier Uses
- Left/Right Side
- Upper/Lower Left Eyelid
- Upper/Lower Right Eyelid
- Left/Right Hand Digits
- Left/Right Foot Toes
- Left Circumflex Coronary Artery
- Left Anterior Descending Coronary Artery
- Left Main Coronary Artery
- Right Coronary Artery
- Ramus Intermedius Coronary Artery
North American Nursing Diagnosis Association
NANDA
Nursing vocabulary used to develop, refine, and promote terminology that accurately reflects nurses' clinical judgements.
Used to classify nursing diagnoses in all nursing settings and is terminology used designed to define patient responses, document care for reimbursement, and to allow for the inclusion of nursing terminology in building clinical EHRs.
Healthcare Cost and Utilization Project
HCUP
A group of healthcare databases and related software tools developed through collaboration by the federal and state governments and healthcare industry to create a national information resource for patient-level healthcare data.
It is an initiative of the Agency for Healthcare Research and Quality (AHRQ)
The Nation’s most comprehensive source of hospital data, including information on in-patient care, ambulatory care, and emergency department visits.
It enables researchers, insurers, policymakers and others to study health care delivery and patient outcomes over time, and at the national, regional, State, and community levels.
Agency for Healthcare Research and Quality
AHRQ
Agency most involved in health services research.
Looks at issues related to the efficiency and effectiveness of the healthcare delivery system, disease protocols, and guidelines for improved disease outcomes.
Record-Over-Record Benchmarking
Method of calculating errors in a coding audit that allows benchmarking with other hospitals, and permits that reviewer to track errors by case type.
This method of calculating errors considers each health record coded incorrectly as one error.
The advantages are
- It allows for benchmarking with other hospitals that frequently use it.
- Permits reviewers to track errors by case type
- Enable reviewers to relate productivity with quality errors on a case-by-case basis
- Is much quicker to calculate
Disadvantages
- It lacks specificity because it does not identify the coder's ability to assign codes that must be reported.
- It does not identify the number of secondary diagnosis or procedures missed by the coder.
Radiology Professional Component
Describes the services of a physician who supervises the taking of the x-ray film and the interpretation of the results.
Radiology Technical Component
Describes the services of the person who uses the equipment, the film, and other supplies.
Radiology Global Component
Describes the combination of the professional and technical components.
Topography of Neoplasms
Site of the neoplasm
Morphology of Neoplasms
Cell structure and form of neoplasm
Grading of Neoplasms
Variation from normal tissue of neoplasms
Differentiation of Neoplasms
Another term for variation from normal tissue of neoplasms.
Data Dictionary
A descriptive list of the data elements to be collected in an information system or database whose purpose is to ensure consistency of terminology.
It ensures each piece of data can mean only one thing.
Clinical Vocabulary
A formally recognized list of preferred medical terms.
A list or collection of all clinical words or phrases with their meanings.
PEG Procedure
A safe and effective way to provide food, liquids and medications (when appropriate) directly into the stomach through a tube.
General Equivalency Mappings
GEMS
Mappings between ICD-9-CM and ICD-10-CM developed and released by the National Center for Health Statistics (NCHS) to facilitate the transition from one code set to another.
Skilled Nursing Facility
SNF
Assessment Instrument is MDS (Minimum Data Set).
Case-Mix Management or Diagnosis Grouping is RUG (Resource Utilization Group).
Resource Utilization Group
RUG
Classification for resources used.
Patients are classified into 1 of 66 possible groups based on info from MDS. There are 52 Upper Groups and 14 Lower Groups.
These subsequently classify residents into 7 payment categories.
Ambulatory Payment Classification
APC
Case-Mix Management or Diagnosis Grouping used in ASCs (Ambulatory Surgical Centers).
OPPS (Outpatient Prospective Payment System) or HOPPS (Hospital Outpatient Prospective Payment System) used for reimbursement.
Payment status indicator "N" means payment is packaged into the payment for other services.
Based on CPT and HCPCS coding.
Clinical lab services are excluded under OPPS/HOPPS and this methodology.
Home Health
Diagnosis Grouping or Case-Mix Management System used is Home Health Resource Group (HHRG).
Assessment Instrument is OASIS
Coding is HIPPS
Claim Submission is HAVEN
Outpatient Prospective Payment System Packaged Items
OPPS
- Minor Ancillary Services
- Inexpensive Drugs
- Medical Supplies
- Implantable Devices
- Anesthesia
- Recovery Room
RBRVS
A system of classifying health services based on the cost of furnishing physician services in different settings, the skill and training levels required to perform the services, and the time and risk involved.
Fee-for-service payment system.
Payment system for physicians and some other health professionals.
Payments based on 3 components
•Relative Value Unit (RVU)
- Unit of measure to compare resources required to perform services.
RVU is the sum of the following 3 Elements:
•Physician Work
(WORK)
•Practice Expenses (PE)
•Malpractice
(MP)
•Geographic Adjustment - Applied to each of the three
elements - Geographic Practice Cost Indexes (GPCI)
•Conversion
Factor (CF) - A constant, across the board multiplier that applies to
the entire RVU. When multiplied, it transforms the RVU into a Medicare
Physician Fee Schedule (MPFS)
Coding used is HCPCS or CPT
Formula is
(Work RVU)(Work GPCI) +
(PE RVU)(PE GPCI) +
(MP
RVU)(MP GCPI) = SUM
SUM * CF = MPFS
Ambulatory Patient Group
APG
A visit based classification that describes the amount and type of resources consumed during the visit. These are codes that go into the APC.
Nonparticipating Providers
or
nonPARs
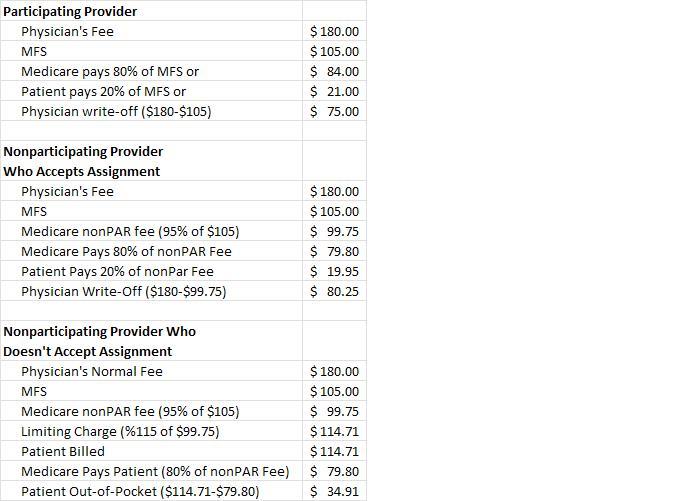
Providers who do not sign a participation agreement with MEDICARE.
If they accept assignment, they are paid 95% of the MEDICARE payment a participating provider would receive.
If they do not accept assignment then the provider is subject to Medicare's limiting charge rule which states providers may not charge a patient more than 115% of the nonparticipating fee schedule. The patient pays the provider and Medicare reimburses the patient.
For examples see pic
Accept Assignment
The provider accepts, as payment in full, the allowed charge from the fee schedule from Medicare. They cannot and will not bill the patient the balance.
Ex: Bill is $500 but the fee schedule allows $300 in reimbursement. The provider will not bill the patient for the remaining $200.
Balance Billing
Billing the patient for the amount not covered by insurance.
Remittance Advice
Statement sent the provider explaining payments made by third party payers
MS-DRG
Has 25 major diagnostic categories divided into surgical and medical partitions.
Type of a case mix group (CMG) that puts patients into groups based on the amount of resources used.
Only one is assigned per inpatient.
Developed by CMS for inpatient hospital care to Medicare patients. Facility is reimbursed a set fee for each group.
Electronic Data Interchange
EDI
A standard transmission format using strings of data for business information communicated among the computer systems of independent organizations.
The electronic (computer-to-computer) exchange of data.
Provides the ability to edit, submit, and pay healthcare claims by way of electronic transfer.
Health Information Exchange
HIE
A plan in which health information is shared among providers.
Also for facilities that have no relation with each other.
Formally Regional Health Information Organizations.
Encoder
Specialty software used to facilitate the assignment of diagnostic and procedural codes according to the rules of the coding system.
Grouper
Computer program that uses specific data elements to assign patients, clients, or residents to groups, categories, or classes.
Used to assign patients to case-mix groups and MS-DRGs for reimbursement.
Scrubber
An internal auditing system that reviews claims for errors before they are sent for payment.
Types of Errors They Can Find
- Incompatible dates of service
- Nonspecific or inaccurate diagnosis and procedure codes
- Lack of medical necessity
- Inaccurate revenue code assessment
UB-04
Billing form used by facilities to submit claims for payment.
The single standardized Medicare form for standardized uniform billing, for hospital inpatients and outpatients.
Also used by third party payers and most hospitals.
CMS-1500
Billing form used by physicians and other noninstitutional providers and suppliers to submit claims for payment.
CMS-1491
Billing form used by ambulance services to submit claims for payment.
Medicare Summary Notice
Statement sent to the patient to show how much the provider billed, how much Medicare reimbursed the provider, and what the patient must pay the provider.
Coordination of Benefits
Method of integrating benefits payments from all health insurance sources to ensure that payments do not exceed 100% of the covered healthcare expenses.
Explanation of Benefits
A statement sent by a third party payer to the patient to explain services provided, amounts billed, and payments made by the health plan.
ASC
Ambulatory Surgical Center
Bilateral procedures are reimbursed at
150%
Calculate CMI (Case Mix Index)
Multiply each RW (Relative Weight) by number of patients. Add total of RWs.
Add total number of patients.
RW/# of Patients
HIPPA requires the retention of health insurance claims and accounting records for a minimum of _____ years.
Six
Fraud
Knowingly making false statements or representation of material facts to obtain a benefit or payment for which no entitlement would otherwise exist.
A willful and intentional misrepresentation that could cause harm or loss to a person or the person's property.
Intentionally making a claim for payment that one knows to be false.
Abuse
Unknowing or unintentional submission of an inaccurate claim for payment.
Payment Status Indicator
Assigned to every HCPCS/CPT code under the Medicare hospital outpatient prospective payment system to identify how the service or procedure described by the code would be paid (ex: fee schedule, APC, reasonable cost, unpaid, etc).
These are letters A-H, K-P, Q1, Q2, Q3, R-V, X, and Y. Reimbursement book pg 177.
C = Inpatient-only services
N = Packaged into APC payment
S = Significant procedures, multiple procedure reduction does not apply
T = Surgical procedures, multiple production reduction applies
V = Medical Visits
X = Ancillary Services
Medical Necessity
Term used to indicate that the service or procedure is reasonable and necessary for the diagnosis or treatment of illness or injury consistent with generally accepted standards of care.
Healthcare services and supplies that are proved or acknowledged to be effective in the diagnosis, treatment, cure, or relief of a health condition, illness, injury, disease, or its symptoms and to be consistent with the community's accepted standard of care.
Only those services, procedures, and patient care are provided that are warranted by the patient's condition.
Stark I Law
Prohibits a physician from referring Medicare patients to clinical laboratory services where a doctor or member of his family has a financial interest.
Never Events
Errors in medical care that are of concern to both the public and health care professionals and providers, clearly identifiable and measurable (and thus feasible to include in a reporting system), and of a nature such that the risk of occurrence is significantly influenced by the policies and procedures of the health care organization.
Errors in medical care that are clearly identifiable, preventable, and serious in their consequences for patients.
Sentinel Events
Any unanticipated event in a healthcare setting resulting in death or serious physical or psychological injury to a patient or patients, not related to the natural course of the patient's illness.
3-Day Payment Window
or
72-Hour Rule
Requires that outpatient pre-admission services that are provided by a hospital up to 3 calendar days prior to a patient's inpatient admission be covered by the IPPS MS-DRG payment for
- Diagnostic Services
- Therapeutic (or non-diagnostic services) whereby the inpatient principal diagnosis code (ICD-9-CM) exactly matches the code used for pre-admission services.
Interrupted Stay
Discharge in which the patient was discharged from the inpatient rehabilitation facility and returns within 3 calendar days.
Reimbursement continues as if the patient never left and is considered 1 discharge and 1 payment.
Medicare Physician Fee Schedule
MPFS
The maximum amount of reimbursement that Medicare will allow for a service.
Consists of a list of payments for services defined by a service coding system, ex: HCPCS.
Formula:
(Work RVU * Work GPCI)+(PE RVU * PE GCPI)+(MP RVU * MP GCPI) = Sum
SUM * CF = This
It is most affected by the CF
This replaced the Medicare physician payment system of "customary, prevailing, and reasonable" charges whereby physicians were reimbursed according to their historical record of the charge for the provision of each service.
Global Payment
Method of payment in which the third-party payer makes one consolidated payment to cover the services of multiple providers who are treating a single episode of care.
Ex: Home health. One payment covers speech therapy, physical therapy, occupational therapy, skilled nursing visits, home health aide visits, medical social services, and non-routine medical supplies.
Total-Episode-of-Care is the most comprehensive version of this type of payment.
Charge Capturing
This process involves the gathering of charge documents from all the departments within the facility that have provided services to patients to make certain that all charges are coded and entered into the billing system.
Revenue Cycle
The regularly repeating set of events that produces revenue.
The major components are
- Preclaims submission activities - collects patients' info
- Claims processing activities - capture of all billable services, claim generation, & claim corrections
- Accounts receivable - manages the amounts owed to a facility by the customer and third-party payers
- Claims reconciliation and collections - EOBs, MSNs, RAs, sent and collections contacts customers for delinquent amounts.
Who can apply for and receive a waiver from CMS that allows them not to participate in the IPPS?
- Cancer Hospitals
- Children's Hospitals
Hold Harmless
Status in which one party does not hold the other party responsible.
Financial protections to ensure that certain types of facilities (ex: children's hospitals) recoup all of their losses due to the differences in their APC payments and the pre-APC payments.
Local Coverage Determinations
LCD
Review policy that describes the circumstances of coverage (describes when and under what circumstances Medicare will cover a service) for various types of medical treatment. It advises physicians which services Medicare considers reasonable and necessary and may indicate the need for an advance beneficiary notice.
Developed by CMS and Medicare Administrative Contractors.
National Coverage Determinations
NCD
Review policy that describes the circumstances of coverage (describes when and under what circumstances Medicare will cover a service) for various types of medical treatment. It advises physicians which services Medicare considers reasonable and necessary and may indicate the need for an advance beneficiary notice.
Developed by CMS and Medicare Administrative Contractors.
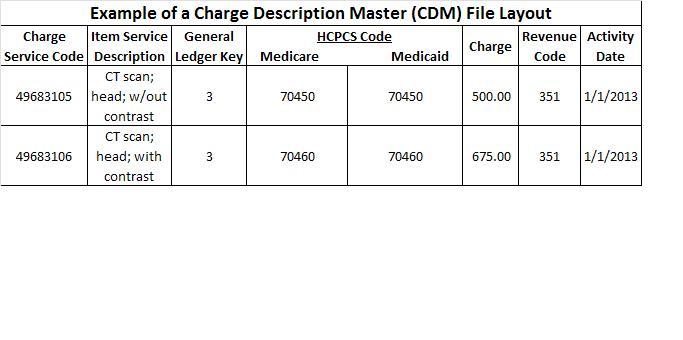
This information is printed on the UB-04 claim form to represent the cost center (eg- -lab, radiology, cardiology, respiratory, etc.) for the department in which the item is provided. It is used for Medicare billing.
- HCPCS
- Revenue Code
- Charge/Service Code
- General Ledger Key
B. Revenue Code
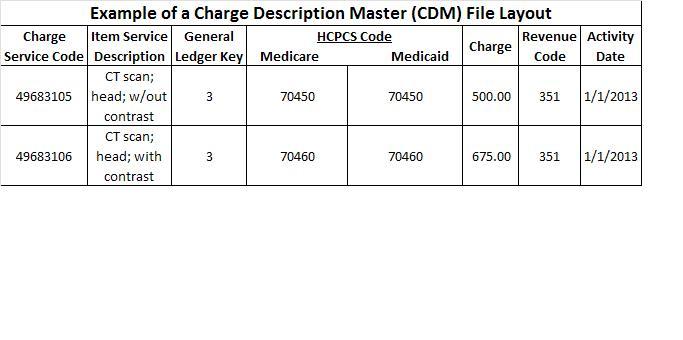
This information is used because it provides a uniform system of identifying procedures, services, or supplies. Multiple columns can be available for various financial classes.
- HCPCS Code
- Revenue Code
- General Ledger Key
- Charge/Service Code
A. HCPCS Code
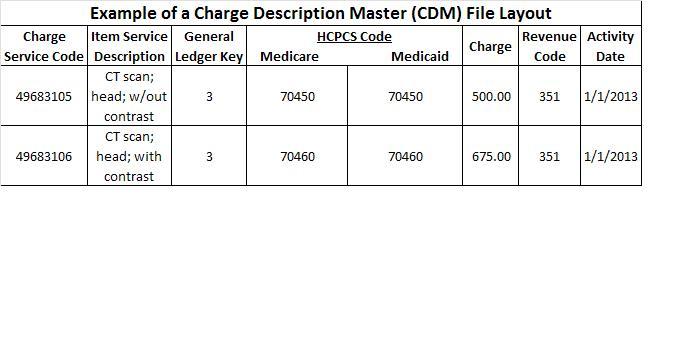
This information provides a narrative name of the services provided. This information should be presented in a clear and concise manner. When possible, the narratives from the HCPCS/CPT book should be utilized.
- General Ledger Key
- HCPCS
- Item/Service Description
- Revenue Code
C. Item/Service Description
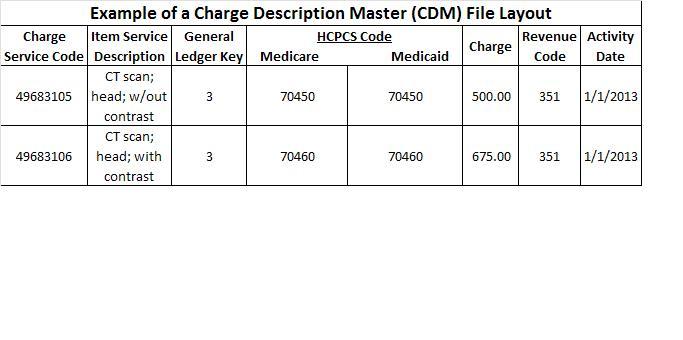
This information is the numerical identification of the service or supply. Each item has a unique number with a prefix that indicates the department number (the number assigned to a specific ancillary department) and an item number (the number assigned by the accounting department or the business office) for a specific procedure or service represented on the chargemaster.
- Charge/Service Code
- HCPCS Code
- Revenue Code
- General Ledger Key
A. Charge/Service Code
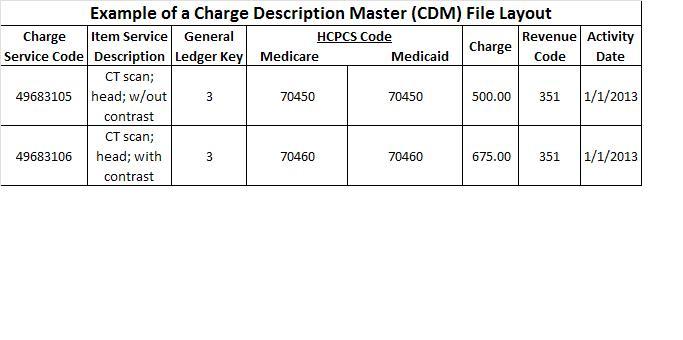
This information is used to assign each item to a particular section of the general ledger in a particular facility's accounting section. Reports can be generated from this information to include statistics related to volume in terms of numbers, dollars, and payer types.
- General Ledger Key
- Charge/Service Code
- Revenue Code
- HCPCS Code
A. General Ledger Key
Discharged Not Final Billed
DNFB
Includes all patients who have been discharged from the facility but for whom the billing process is not complete.
What is the federal fiscal year?
October 1 - September 30 of following year.
National Provider Identifier
A 10-digit, intelligence-free, numeric identifier designed to replace all previous provider legacy numbers. This number identifies the physician universally to all payers. This number is issued to all HIPAA-covered entities and is mandatory on the CMS-1500 and UB-04 claim forms.
OIG's Workplan
A document published by the Office of Inspector General every year. It details the OIG's focus for Medicare fraud and abuse for that year. It gives healthcare providers an indication of general and specific areas that are targeted for review. It can be found on CMS' website.
Advance Beneficiary Notice
A document signed by the patient indicating whether he wants to receive services that Medicare probably will not pay for.
Lifetime Reserve Days
Original Medicare covers up to 90 days in a hospital per benefit period and offers an additional 60 days of coverage with a high coinsurance. These 60 reserve days can be used only once during your lifetime but do not have to be applied towards the same hospital stay.
They are covered under Medicare Part A.
They are usually reserved for use during the patient's final (terminal) hospital stay.
They are not renewable, meaning once they are used, the patient is responsible for the total charges.
Inpatient Rehab Facility
Diagnosis Grouping is CMG (Case Mix Groups)
Assessment Instrument is PAI (Patient Assessment Instrument)
Coding is HIPPS
Hard Coding
HCPCS/CPT codes that appear in the hospital's chargemaster and will be included automatically on the patient's bill.
The process of attaching a CPT/HCPCS code to a procedure located on the facility's chargemaster so that the code will automatically be included on the patient's bill.
Used when coding does not require documentation analysis.
Used for
- Frequently performed procedures
- Radiology
- ECG and other cardiology services
- Electroencephalogram
- Respiratory therapy and pulmonary function
- Rehab services
- Emergency department
Cost Accounting
Accounting method that attributes a dollar figure to every input required to provide a service.
Contractual Allowance
The difference between what the hospital bills and what they receive in payment from third-party payers, most commonly government programs.
Also known as contractual adjustments.
Ex: Providers billed $500 but Medicare contract only allows $400 to be reimbursed.
CMS assigns one _____ to each APC and each _____ code.
Payment Status Indicator, HCPCS
Corporate Integrity Agreement
When healthcare providers are found guilty under any of the civil false claims statuses, the OIG is responsible for negotiating these settlements, the provider is placed under this.
A document that outlines the obligations an entity agrees to as part of a civil settlement. An entity agrees to the CIA obligations in exchange for the OIG’s agreement that it won’t seek to exclude entity from participation in Medicare, Medicaid or other Federal health care programs.
Regarding hospital emergency department and hospital outpatient E/M CPT code assignment, which assignment is true?
Each facility is accountable for developing and implementing its own methodology.
Medicare A
Covers
- Hospital Care
- SNF Care
- Nursing Home Care (as long as custodial care isn't the only care you need)
- Hospice
- Home Health Services
Medicare B
Covers
- Medically Necessary Services - services or supplies that are needed to diagnose or treat your medical condition
- Preventative Services - health care to prevent illness or detect it at an early stage when treatment is most likely to work the best
Medicare C
Medicare Advantage
Plans offered by private companies approved by Medicare. Part A and Part B are covered in this.
Drugs may or may not be included.
Medicare D
Prescription drug coverage.
Incident to Billing
Some services are performed by a nonphysician practitioner (such as a Physician Assistant). These services are in integral yet incidental component of a physician's treatment. A physician must have personally performed an initial visit and must remain actively involved in the continuing care. Medicare requires direct supervision for these services to be billed. This is called _____.
Healthcare Effectiveness Data Information Set
HEDIS
Sponsored by National Committee for Quality Assurance (NCQA)
A set of standard performance measures designed to provide healthcare purchasers & consumers with the information they need to compare the performance of managed healthcare plan.
Measure of access (at least one visit to a provider within 3 years)
Measures of quality (cholesterol screenings)
Measures of member satisfaction (cost per month)
Structure and Content Standards
Information standards that provide clear descriptors of data elements to be included in computer-based patient record systems.
Establish and provide clear and uniform definitions of the data elements to be included in the EHR systems. Specify the type of data to be collected in each data field and the attributes and values of each data field, all of which are captured in data dictionaries.
Clinical Data
Documents the patient's health condition, diagnosis, and procedures performed as well as the healthcare treatment provided.
Administrative Data
Includes demographic and financial information as well as various consents and authorizations related to the provision of care and the handling of confidential patient information.
Problem-Oriented Health Record
Problems are organized in numeric order.
Key characteristic of this format is an itemized list of the patient's past and present social, psychological, and health problems. Each problem is indexed with a unique number.
HL7
A standards development organization accredited by the American National Standards Institute that addresses issues at the seventh, or application, level of healthcare systems interconnections.
It develops messaging, data content, and document standards to support the exchange of clinical information.
A family of standards that aids in the exchange of data among hospital systems and physician practices.
American College of Surgeons
Has an approval process for cancer programs.
One of the requirements of this process is the existence of a cancer registry as part of the program.
National Ambulatory Medical Care Survey
A database from the National Health Care Survey that uses the patient health record as a data source.
Data are collected on a representative sample of hospital-based and freestanding ambulatory surgery centers.
Data include patient demographic characteristics, source of payment, information on anesthesia given, the diagnoses, and the surgical and non-surgical procedures on patient visits of hospital-based and freestanding ambulatory surgery centers.
Hospital Acquired Conditions List From CMS
- Catheter-Associated UTIs
- Pressure Ulcers Stages III & IV
- Serious Preventable Event
- Foreign Object Retained After Surgery
- Air Embolism
- Blood Incompatibility
- Vascular Catheter-Associated Infections
- Mediastinitis After Coronary Artery Bypass Graft
- Falls and Trauma
If these occur, hospitals will not receive the higher reimbursement amount.
It is a paying for value-based purchasing system.
National Correct Coding Initiative Edits
Main purpose is to prohibit unbundling procedures. Also to improve the appropriate payment of Medicare Part B claims. Prevents improper payments when incorrect code combinations are on the claim/reported.
Also apply to the APC system and are updated quarterly.
Outpatient Code Editor
OCE
Operates in the systems of Medicare Administrative Contractors (MACs) and provides a series of flags that can affect APC payment because it identifies coding errors in claims.
Chief Privacy Officer
Entities are required to have one per the Privacy Rule.
Role includes
- Developing and implementing privacy policies and procedures
- Maintaining appropriate forms
- Overseeing privacy training
- Participating in compliance monitoring of business associates
- Ensuring that patients' rights are protected
- Maintaining knowledge of applicable laws and accreditation standards
- Communicating with the OCR (Office of Civil Rights) and other entities in compliance reviews and investigations of alleged privacy violations
Privacy
The quality or state of being hidden from, or undisturbed by, the observation or activities of other persons or freedom from unauthorized intrusion.
In healthcare related contexts, the right of a patient to control disclosure of personal information.
Confidentiality
A legal and ethical concept that establishes the healthcare provider's responsibility for protecting health records and other personal and private information from unauthorized use or disclosure.
Libel
Any publication in print, writing, pictures, or signs that injures the reputation of others.
Slander
Speaking false and malicious words concerning another person that brings injury to his or her reputation.
Defamation
The action of damaging the good reputation of someone
Include slander or libel
Statutory Law
Law that is constituted by rules and principles determined by legislative bodies, either Congress or a state legislature.
Term used to define written laws, usually enacted by a legislative body. These vary from regulatory or administrative laws that are passed by executive agencies, and common law, or the law created by prior court decisions.
Consists of ever changing rules and regulations created by Congress, state legislatures, local governments, or constitutional lawmakers.
These are the inviolable rights, privileges, or immunities secured and protected for each citizen by the Constitution.
The include written codes, bills, and acts (regulations).
Administrative Law
A branch of law that covers regulations set by government agencies.
Examples are licensing boards for physicians and nurses, Workman's Compensation Boards, and the Department of Health and Human Services.
Regulations include
- Licensing and supervision of prescribing, storing, and dispensing controlled substances
- Health department regulations, including reporting requirements of certain communicable diseases
- Regulations against homicide, infanticide, euthanasia, assault, and battery
- Regulations against fraud
- IRS regulations that are healthcare related
Common Law
Also called case law.
Is based on decisions made by judges when they apply previous court decisions to current cases.
This means it is based on the judicial interpretation of previous laws, leading to a common understanding of how a law should be interpreted.
Evolves on a case-by-case basis.
Negligence
An unintentional action that occurs when a person either performs or fails to perform an action that a "reasonable person" would or would not have committed in a similar situation.
The plaintiff must be able to show all of the following
- Duty
- Dereliction
- Direct Cause
- Damages
Duty
Must be shown to prove negligence.
The responsibility established by the physician-patient relationship. The obligation one person has to another.
Dereliction or Neglect of Duty
Must be shown to prove negligence.
A physician's failure to act as any ordinary and prudent physician would act in a similar circumstance. Performance or treatment does not comply with the acceptable standard of care.
Direct Cause
Must be shown to prove negligence.
The continuous sequence of events, unbroken by any intervening cause, that produces an injury and without which the injury would not have occurred.
Direct or Proximate Cause
Means that the injury was proximately or closely related to the physician's negligence.
Means that there were no intervening forces between the defendant's actions and the plaintiff's injury - a cause-and-effect relationship.
Ex: Dr ordered blood test. Lab tech performs venipuncture. PT complains of loss of feeling in arm. PT must prove there was no intervening injury between blood draw and pain in arm started. IE - no accident or injury
Breach of Contract
The failure, without legal excuse, to perform any promise or to carry out any of the terms of an agreement.
Failure to perform a contractual duty.
EX: Physician refuses to perform service he promised or PT refuses to pay bill as promised by accepting care form physician.
Contract Elements
Offer/Communication
Price/Consideration
Acceptance
Spoliation
The intentional destruction, mutilation, alteration, or concealment of evidence.
This affects e-discovery.
Freedom of Information Act
A federal law through which individuals can seek access to information without authorization of the person to whom the information applies.
This act applies only to federal agencies and not the private sector.
The Veterans Administration and Defense Department hospital systems are subject to this act, but few other hospitals are.
The only protection of health information held by federal agencies exists when disclosure would "constitute a clearly unwarranted invasion of personal privacy."
Res Ipsa Loquitur
"The thing that speaks for itself."
Applies to the law of negligence. Means the breach of duty is so obvious that it doesn't need further explanation - it can speak for itself and no witnesses are needed.
EX: Leaving sponge in patient, amputating wrong limb, operating on wrong body part.
Respondeat Superior
"Let the master answer"
Means the employer is responsible for the actions of the employee.
Stare Decisis
"Let the decision stand"
Means to abide by, or adhere to, decided cases.
Deposition
Oral testimony that is made before a public officer of the court to be used in a lawsuit.
Interrogatory
Written questions submitted to a party from his or her adversary to ascertain answers that are prepared in writing and signed under oath and that have relevance to the issues in a lawsuit.
Contributory Negligence
Conduct on the part of the plaintiff that is a contributing cause of injuries.
If the plaintiff is found to be fully or in part at fault for the injury, the patient may be barred from recovering any monetary damages.
Doctrine of Charitable Immunity
Premise that charitable institutions could be held blameless for their negligent acts.
Darling v. Charleston Community Memorial Hospital
Established the doctrine of corporate negligence.
Doctrine of Corporate Negligence
The legal doctrine that holds health-care facilities, such as hospitals, nursing homes and medical clinics, responsible for the well-being of patients.
If a health-care facility fails to maintain a clean and safe environment, hire competent and properly trained employees, oversee care and implement safety policies, it can be held liable for any harm to patients.
Privacy Act of 1974
Provides private citizens some control over information that the federal government collects about them by limiting the use of information for unnecessary purposes.
An agency may maintain only the information that is relevant to its authorized purpose.
Citizens have the right to gain access to their records and to copy any of the records.
Only applies to federal agencies and government contractors. Allows patients of a Department of Defense health care facility to request amendments to their record.
Misfeasance
The improper performance of an otherwise proper or lawful act.
Ex: Nurse does venipuncture incorrectly causing nerve damage.
Malpractice
Professional misconduct or demonstration of an unreasonable lack of a skill with the result of injury, loss, or damage to the patient.
Ex: Leaving sponge in patient.
Nonfeasance
The failure to perform an action when it is necessary.
Ex: Failure to give CPR to a patient who collapses in the waiting room.
Malfeasance
Performing an illegal act.
Ex: Nurse prescribing medication.
Informed Consent
Consent granted by a person after the patient has received knowledge and understanding of potential risks and benefits.
Ideal form of consent.
Implied Consent
An agreement that is made through inference by signs, inaction, or silence.
Ex: Sticking arm out for shot.
Courts can release adoption records based on _____.
A court order for good cause.
Advance Directives
The various methods by which a patient has the right to self-determination prior to a medical necessity - includes living wills, healthcare proxies, and durable power of attorney.
Living Will
A legal document in which a person states that life-sustaining treatments and nutritional support should not be used to prolong life.
A type of advance directive.
Patient Self-Determination Act
Encourages everyone to decide about the types and extent of medical care they want to accept or refuse if they become unable to make those decisions due to illness.
This requires all health care agencies to recognize the living will and durable power of attorney for health care and applies to hospitals, long-term care facilities, and home health agencies that get Medicare and Medicaid reimbursement.
Health care agencies must ask whether there is an advance directive and document it the medical record. They also must give patients information about their rights under state law.
Durable Power of Attorney
A legal agreement that allows an agent or representative of the patient to act on behalf of the patient.
A type of advance directive.
Client Server
Predominant form of computer architecture used in healthcare organizations today.
A computer architecture in which multiple computers that store and process application software and data are connected to other computers that enter data and retrieve information.
Ex: A server contains Microsoft Word. Word is accessed from a cubicle and a document is created. The document is saved on the server.
Foreign Key
A key attribute used to link one entity/table to another.
A column of one table that corresponds to a _____ key of another table. Together they allow the two tables to join together.
Used to associate relationships between entities (tables) in a relational database.
Primary Key
An explanatory notation that uniquely identifies each row in a database.
Ensure that each row is unique and must not change in value. Typically a number.
It is good programming practice to create one that is independent of the data in the table.
Interfaces
The zone between different computer systems across which users want to pass information.
Ex: A computer program written to exchange information between systems of the graphic display of an application program designed to make the program easier. Microsoft Windows.
Natural Language Processing
NLP
A field of computer science and linguistics concerned with the interactions between computers and human languages that converts information from computer databases into readable human language.
Digital text form online documents stored in the organization's information system is read directly by the software, which then suggests codes to match the documentation.
Is used in computer-assisted coding (CAC).
Integration Test
Determines how well new systems being implemented work with existing systems.
Digital Certificate
An electronic document that establishes a person's identity online.
A process of identity proofing that generates electronic authentication credentials.
Must be issued by a federally approved credential service provider or certification authority.
Used to implement public key encryption on a large scale.
An electronic document that uses a digital signature to bind together a public key with an identity such as the name of a person or organization, their address, and so forth. Can be used to verify that a public key belongs to an individual.
Uses the letter S at the end of HTTP.
Digital Imaging and Communication in Medicine
DICOM
A standard that promotes a digital image communications format and picture archive and communications systems for use with digital images.
Cloud Computing
Information systems that use the Internet to access data.
Refers to the delivery of computing resources over a network sold as a metered service - like buying electricity.
To keep costs low, the vendor provides the same service to every client, so customization is not possible.
Virtual Private Network
VPN
An encrypted tunnel through the Internet that enables secure transmission of data or to connect remote sites or users.
Designed to reduce the cost of used leased lines through a WAN while maintaining security.
RFP
Request for Proposal
Components include
- Organizational Profile
- Vendor Information
- Functional Specifications
- Operational Requirements
- Technical Requirements
- Application Support
- Licensing and Contractual Details
- Evaluation Criteria
Organizational Profile
Component of the RFP
Describes the healthcare organization making request
- Basic Demographics
- Mission and Goals
- Vision for the EHR
- Current Information Infrastructure
- Specific Constraints
- Instructions for Responding
Vendor Information
Component of the RFP
Asks the vendor for a description of its demographics.
Includes
- Vendor's Size and Longevity
- Years in Business
- Revenues
- Profitability
- Number of Employees
- Product Research and Development History and Plans
- Types of Installations
- Number
- Size
- Status
- Corporate Composition
- Organizational Makeup
- Employee Qualifications and Tenure
- State or Country Where Most Work is Performed
- References
- User Group Information
- Leader
- Size
- Frequency of Meetings
- Contract History
- Any Defaults
- Pending Lawsuits
- IRS Status
Functional Specifications
Component of the RFP
Organization requests a description of functional capability, such as processes and workflows and the product supports, and compares these against its redesigned workflows and processes.
The organization may develop a script describing a scenario, or use case, based on its redesigned workflows and processes and ask vendor how product would perform the inherent functions.
Operational Requirements
Component of the RFP
Should elicit information on the EHR product's
- Data Architecture
- Analytical Processes Supported
- Necessary Interfaces
- Reliability and Security Features
- System Capacity
- Expansion Capabilities
- Response Time
- Downtime
- Other Maintenance Issues
Technical Requirements
Component of the RFP
Vendor should propose the appropriate technical architecture to meet the organization's EHR functional specifications and operational requirements, delineating the specific hardware, networking, and software requirements.
Application Support
Component of the RFP
Vendor proposes an implementation schedule and describes data conversion, acceptance testing, training, and documentation as well as the ongoing support, maintenance, and upgrades it will supply.
Licensing and Contractual Details
Component of the RFP
Vendor is asked to supply its specific one-time bid and recurring costs based on the organization's requirements.
Should also include a request for the vendor's standard contract, financing arrangements, proposed relationships with hardware vendors, and warranty information.
Evaluation Criteria
Component of the RFP
Explains what the organization thinks is the most important so the vendor knows upfront.
BC-MAR
Bar Code Medication Administration Record
One way that an EHR is distinguished from a clinical data repository is that the EHR ____
Has clinical decision support capabilities.
Information Brokering
Buying and selling information.
Decision Support System
DSS
Provides information to help users make accurate decisions.
Knowledge Management System
KMS
A type of system that supports the creation, organization, and dissemination of business or clinical knowledge and expertise to providers, employees, and managers throughout a healthcare enterprise.
Differentiate between the physical and logical data models.
The logical data model shows what the system should do.
The physical model shows how the logical data model will be created.
Back-End Speech Recognition
Specific use of speech recognition technology (SRT) in an environment where the recognition process occurs after the completion of dictation by sending voice files through a server.
Front-End Speech Recognition
The specific use of a speech recognition technology in an environment where the recognition process occurs in real time (or near real time) as dictation takes place.
Data Mart
A well-organized, user-centered, searchable database system that usually draws information from a data warehouse to meet the specific needs of the user.
A subset of the data warehouse designed for a single purpose or specialized use. It performs the same type of analyses as a data warehouse; however, the target area is narrower.
Relational Database
A type of database that stores data in predefined tables made up of rows and columns.
Data that can be stored are
- Currency
- Real Numbers
- Integers
- Strings (Characters of data)
Object Oriented Database
A type of database that uses commands that act as small, self-contained instructional units (objects) that may be combined in various ways.
Data that can be stored are
- Graphics
- Movies
- Audio
Hierarchical Database
A type of database that allows duplicate data.
Laboratory Information System
LIS
An information system that collects, stores, and manages laboratory tests and their respective results.
It can speed up access to test results through improved efficiency from various locations, including anywhere in the hospital, the physician's office, or even the clinician's home.
Radiology Information System
RIS
A system that collects, stores, and provides information on radiological tests such as ultrasound, magnetic resonance imaging, and positron emission tomography.
Pharmacy Information System
System that assists care providers in ordering, allocating, and administering medication.
It focuses on patient safety issues, especially medication errors and allergies and providing optimal patient care.
Must be in place to ensure that CPOE system supports patient safety.
Physical Safeguards
Include the protection of computer systems from natural and environmental hazards and intrusion.
Consist of
- Facility Access Controls - includes establishing safeguards to prohibit the physical hardware and computer system from unauthorized access and to protect the computer system from untoward physical events - fire, flood, electrical malfunction.
- Workstation Security - document what the proper functions to be performed at workstations with access to e-PHI.
- Device and Media Control - facility must specify proper use of electronic media and devices and the physical attributes of the surroundings of a workstation that can access the e-PHI. Includes removal or disposal of equipment.
Risk Management
Encompasses the identification, management, and control of untoward events.
Can aid prevention, intrusion detection, and mitigation of security breaches including identity theft.
Development prompted by the medical malpractice crisis of the 1970s.
Risk Assessment
Identifying security threats, risks, and vulnerabilities, determining how likely it is that any given threat may occur, and estimating the impact of an untoward event.
Usually performed by a multidisciplinary team that has specific knowledge about data security and the organization.
Access Control
A computer software program designed to prevent unauthorized use of an information resource.
The process of designing, implementing, and monitoring a system for guaranteeing that only individuals with a legitimate need are allowed to view or amend specific data sets.
Being able to identify which employees should have access only to data they need to do their jobs.
Authentication
The process of identifying the source of health record entries by attaching a handwritten signature, the author's initials, or an electronic signature.
Proof of authorship that ensures, as much as possible, that log-ins and messages from a user originate from an authorized source.
Authorization
The granting of permission to disclose confidential information.
As defined in terms of the HIPAA Privacy Rule, an individual's formal written permission to use or disclose his or her personally identifiable health information for purposes other than treatment, payment, or healthcare operations.
Administrative Safeguards
Include policies and procedures that address the management of computer resources.
Ex: Policy may state that user must log off when not using computer.
They use
- Password Management - ensures end users can access only the information they have permission to access
- Edit Checks - help ensure data integrity by allowing only reasonable and predetermined values to be entered into computer
- Audit Trail - tracks every single access to data in the computer system
Cracker
An individual with extensive computer knowledge whose purpose is to breach or bypass internet security or gain access to software without paying royalties. The general view is that they break things and their motivations can range from profit, a cause they believe in, general maliciousness or just because they like the challenge. They may steal credit card numbers, leave viruses, destroy files or collect personal information to sell.
Fetal Death
A stillborn baby. Death is prior to the fetus's complete expulsion or extraction from the mother regardless of the length of the pregnancy.
They are neither admitted or discharged from the hospital.
Fetal death occurs when the fetus fails to breathe or show any sign of life - heartbeat, pulsation of the umbilical cord, or movement of the voluntary muscles.
Only intermediate and late fetal deaths are included in fetal death rate calculations.
Average Daily Census
Total Inpatient Service Days for a Period (not NB)
Total number of days
Average LOS
Total Length of Stay (discharge days)
Total Number of Discharges
Percentage of Occupancy
Total Number of Inpatient Service Days X 100
Total Inpatient Bed Count Days x Number of Days
Inpatient Bed Count
Number of available hospital beds, both occupied and vacant, on any given day
Total Inpatient
Sum of all inpatient service days for each of the days in the period.
Length of Stay
LOS
Number of calendar days from admission to discharge.
Total Length of Stay
Sum of the days' stay of any group of inpatients discharged during a specific period.
Inpatient Bed Count Day
Counts the presence ot one inpatient bed (occupied or vacant)
that is set up and staffed for use in one 24-hour period.
Total Inpatient Bed Count Day
Sum of all bed count days for each of the days in a period.
Bed Turnover Rate
Direct Formula
Total Number of Discharges
Average Bed Count for the Period
or
Discharges
Beds
Bed Turnover Rate
Indirect Formula
Use this formula in cases where the bed count changes during the period.
Percentage of Occupancy x Days in the Period X 100
Average Length of Stay
Anesthesia Death Rate
Total Number of Deaths Caused by an Anesthetic Agent X 100
Total Number of Anesthetics Administered
Fetal Death Rate
Stillbirth Rate
Total Number of Intermediate and Late Fetal Deaths X 100
Total Number of Births + Intermediate and Late Fetal Deaths
Gross Hospital Death Rate
Proportion of all discharges that ended in death.
Total Number of Inpatient Deaths (including newborns) X 100
Total Number of Discharges (including deaths and newborns)
Net Hospital Death Rate
Number of Inpatient Deaths (including NB) - Deaths <48 Hours of Admission
Total Discharges (including deaths and NB - Deaths <48 Hours)
That number X 100
Maternal Death Rate
Total Number of Maternal Deaths X 100
Total Number of OB Discharges
Neonatal Death Rate
Infant Mortality Rate
Total Number of NB Deaths X 100
Total Number of Newborn Discharges
Postoperative Death Rate
Number of Deaths Within 10 Days of Surgery X 100
Total Number of Patients Operated on
Newborn Autopsy Rate
Number of Autopsies on NB Deaths X 100
Total Number of NB Deaths
Fetal Autopsy Rate
Number of Autopsies on Intermediate and Late Fetal Deaths X 100
Total Number of Intermediate and Late Fetal Deaths
Gross Autopsy Rate
Total Inpatient Autopsies X 100
Total Inpatient Deaths
Net Autopsy Rate
Total Inpatient Autopsies X 100
Total Inpatient Deaths - Unautopsied Coroner's Cases
Hospital Autopsy Rate (Adjusted)
Total Hospital Autopsies X 100
Number of Deaths of Hospital Patients Whose Bodies are Available for Hospital Autopsy
Newborn
Infants born alive in the hospital
Fetal Death Classifications
Early Fetal Death - <20 weeks gestation 500g or less
Intermediate Fetal Death - 20 weeks to <28 weeks gestation 501-1000g
Late Fetal Death - 28 weeks gestation over 1000g
Verbal Order Authentication
Based on federal and state law.
Must be done within 48 hours if a state time frame doesn't exist.
Clinical Privileges
Granted for no more than 2 years at a time.
Kaizen
A core principle of quality management generally, and specifically within the methods of Total Quality Management and 'Lean Manufacturing'.
Crosby
Focused on Zero Defects
Peters
Identified leadership as being central to the quality improvement process, discarding the word “Management” for “Leadership”.
Deming
Revitalized the Japanese economy.
Quality must be built into the product.
Developed a 14 point plan to help executives to lead their organizations.
Believed merit raises, formal evaluations, and quotas established through benchmarking hinder worker productivity and growth.
Joiner
Maintained that quality begins at the top and funnels down.
Developed the Joiner triangle that consists of
- Quality to ensure customer satisfaction and loyalty.
- A scientific approach to root out underlying causes of problems.
- The all-one-team method that encourages and empowers employees to work together to break down departmental barriers and creates buy-in to improvement, ownership in the process, and commitment to quality.
Juran
Consulted with the Japanese.
Claimed that management could control over 80% of quality defects by using the three central principles of quality: planning, control, and improvement.
Believed that training and hand-on management are basic requirements for meeting the needs of customers.
Force Field Analysis
A performance improvement tool used to identify specific drivers of, and barriers to, an organizational change so that positive factors can be reinforced and negative factors reduced.
Structure Indicators
Measure the attributes of the setting, such as number and qualifications of the staff, adequacy of equipment and facilities, and adequacy of organizational policies and procedures.
Process Indicators
Measure the actions by which services are provided, the things people or devices do, from conducting appropriate tests, to making a diagnosis, to actually carrying out a treatment.
Outcome Indicators
Measure the actual results of care for patients and populations, including patient and family satisfaction.
Control Chart
This has the sideways bell curve with lines indicating two or three standard deviations from the mean.
A type of run chart that includes both upper and lower control limits and indicates whether a process is stable or unstable.
Best tool for differentiating between common cause variation and special cause variation.
Run Chart
Displays data points over a period of time.to provide information about performance and identifies emerging trends or patterns.
Same as a line graph.
Special Cause Variation
An unusual source of variation that occurs outside a process but affects it.
Ex: Upsetting phone call right before BP reading will elevate BP. BP meds will lower BP causing a lower reading.
Common Cause Variation
The source of variation in a process that is inherent within the process.
Ex: BP readings - cuff may be placed slightly differently each time slightly skewing the reading but not by much.
Administrator, Agency for Health Care Policy and Research
AAHCPR
Established by Congress in 1989 "for the purpose of enhancing the quality, appropriateness, and effectiveness of health care services and access to care."
Institute of Medicine
IOM
Published a landmark report in 1991, To Err Is Human, outlining the need for computer-based patient record systems.
Report led the Joint Commission to place emphasis on improving patient safety and sentinel event occurrences through its safety program known as National Patient Safety Goals (NPSG).
Nonprofit organization that is part of the National Academies that provides advice to lawmakers and the public.
Defined what an EHR should be.
National Committee for Quality Assurance
NCQA
An accreditation organization that began accrediting managed care organizations in 1991.
Standards focus on patient safety, confidentiality, consumer protection, access to services, service quality, and continuous improvement efforts.
Recently expanded its programs to include other types of health plans and specialty certifications for non-comprehensive programs such as ones focusing on multicultural healthcare or disease management.
Physician Quality Reporting System
PQRS
An incentive payment system for eligible professionals who satisfactorily report data on quality measures for covered professional services furnished to Medicare beneficiaries.
Six Sigma
Uses statistics for measuring variation in a process with the intent of producing error free results.
This measure indicates no more than 3.4 errors per one million encounters.
Defines improvement opportunities using a critical quality tree.
National Patient Safety Goals
NPSG
Goals issued by the Joint Commission on Accreditation of Healthcare Organizations to improve patient safety in healthcare organizations nationwide.
They outline for healthcare organizations the areas of organizational practice that most commonly lead to patient injury or other negative outcomes that can be prevented when staff utilize standardized procedures.
Intracycle Monitoring
The Joint Commission's emphasis on improving quality of patient care for a participating facility is exemplary through the required self-assessment of this process tool.
Span of Control
Refers to the number of subordinates or departments a supervisor has
Formal Theory of Authority
Authority is based upon the rank or position of the person.
Specialization of Labor
The division of cooperating individuals who perform specific tasks and roles into roles where each does his own task, or part of the whole, and the end product is the result.
Unity of Command
Refers to the principle that a subordinate should have one and only one superior to whom he or she is directly responsible.
Flex Time
Allows their employees to control the work schedule within parameters established by management.
Bona Fide Occupational Qualification
An exception to the Age Discrimination in Employment Act that allows an employer to know employees' ages if they can demonstrate that age makes a difference to the job.
Ex: Waitress must be 18 to serve alcohol.
Trigger Events
- The record of a patient with the same last name or address as the employee
- VIP patient records (e.g., board members, celebrities, governmental or community figures, physician providers, management staff, or other highly publicized individuals)
- The records of those involved in high-profile events in the community (e.g., motor vehicle accident, attempted homicide, etc.)
- Patient files with isolated activity after no activity for 120 days
- Other employee files across departments and within departments (organizations should set parameters to omit legitimate caregiver access)
- Records with sensitive health information such as psychiatric disorders, drug and alcohol records, domestic abuse reports, and AIDS
- Files of minors who are being treated for pregnancy or sexually transmitted diseases
- Records of patients the employee had no involvement in treating (e.g., nurses viewing patient records from other units)
- Records of terminated employees (organizations should verify that access has been rescinded)
- Portions of a record that an individual's discipline would not ordinarily have a need to access (e.g., a speech pathologist accessing a pathology report)
Business Continuity Processes
A program that incorporates policies and procedures for continuing business operations during a computer system shutdown.
Sometimes called contingency and disaster planning.
Data Use Agreement
A legal binding agreement between the OPDIV and an external entity (e.g., contractor, private industry, academic institution, other Federal government agency, or state agency), when an external entity requests the use of personally identifiable data that is covered by a legal authority, such as the Privacy Act of 1974.
The agreement delineates the confidentiality requirements of the relevant legal authority, security safeguards, and the OPDIV’s data use policies and procedures.
It serves as both a means of informing data users of these requirements and a means of obtaining their agreement to abide by these requirements.
It serves as a control mechanism for tracking the location(s) of the OPDIV’s data and the reason for the release of the data and requires that a System of Records (SOR) be in effect, which allows for the disclosure of the data being used.
Federal Sentencing Guidelines
Outline 7 steps as the hallmark of an effective program to prevent and detect violations of the law.
These steps have become the blueprint for an effective compliance program for healthcare organizations.
These were established by the US Sentencing Commission to establish "uniform punishment that is applied to similarly situated defendants upon conviction".
Office of Inspector General
OIG
Issues compliance program guidance for various types of healthcare organizations.Their website posts the documents that most healthcare organizations need to develop fraud and abuse compliance plans.
Investigates and audits healthcare fraud.
Middle Management
Develops, implements, and revises the organization's policies.
Staffing Tools
Used to plan and manage staff resources.
Examples:
- Position Descriptions
- Policies and Procedures
- Training Checklists
- Performance Standards
Deficit Reduction Act of 2005
Made compliance programs necessary.
Was enacted in '06 and is particularly significant from a compliance perspective because it has transformed the nature of compliance programs from voluntary to mandatory.
Mandated a quality adjustment in the MS-DRG payments for certain hospital-acquired conditions. Inpatient hospitals are required to submit POA indicators on diagnoses for all inpatients.
Business Associate Agreements
A written and signed contract that allows covered entities to lawfully disclose protected health information to business associates such as consultants, billing companies, accounting firms, or others that may perform services for the provider, provided that the business associate agrees to abide by the provider's requirements to protect the information's security and confidentiality.
Facilities that have to meet the standards in the Conditions of Participation
- Hospitals
- Home Health Agencies
- Ambulatory Surgery Centers
- Hospices
Audit Trail
A record of system and application activity by users that tracks when an employee has accessed the system and how long the employee has been logged into a system.
It logs:
- Name of individual accessing system
- Date and Time system was accessed
- What the person did (edit, delete, read, etc)
Can be used to to help reconstruct when an adverse event or failure occurred.
Who is primarily responsible for implementing the policies and strategic direction of the hospital or healthcare organization and for building and effective executive management team?
- Board of Directors
- Chief Executive Officer
- Chief Information Officer
- Chief of Staff
B. Chief Executive Officer
Record Copying Fees
Privacy Rule requires that the copy fee for the individual be reasonable and cost based. It can only include the costs of labor for copying, postage if mailed, cost of paper if hard copies are made, or cost of media if electronic copies are made.
Recovery Audit Contractor
RAC
Program was completely implemented in the US by January, 2010.
Used to detect and correct improper payments in the Medicare fee-for-service program.
Cost Control
The one aspect of managed care that has had the greatest impact on healthcare organizations.
Federal Anti-Kickback Statute
A criminal statute that prohibits the exchange (or offer to exchange), of anything of value, in an effort to induce (or reward) the referral of federal health care program business.
Exceptions to this are called Safe Harbors
Joint Commission
Accreditation organization that surveys facilities for compliance and the Medicare Conditions of Participation for Hospitals.
They grant deemed status.
Chief Information Officer
CIO
A senior-level executive who is responsible for
- Leading the strategic IS planning process
- Assisting the leadership team to use IS in support of strategic planning and management
- Overseeing the organization's IRM (Information Resource Management) functions
These functions are performed by the IS department, telecommunications, management engineering, and HIM departments.
This person typically reports directly to the organization's CEO
Chief Privacy Officer
CPO
A position that
- Oversees activities related to the development, implementation, and maintenance of and adherence to, organizational policies and procedures regarding the privacy of and access to patient-specific information
- Ensures compliance with federal, state , and accrediting body rules and regulations concerning the confidentiality and privacy of health related information.
Chief Information Security Officer
CISO
A recently created position that is responsible for
- Overseeing the development, implementation, and enforcement of a healthcare organization's security policies
- Managing the security of all patient-identifiable information, whether stored in paper-based or computer-based systems.
Chief Medical Informatics Officer
CMIO
A relatively new position within the information services organizational structure, typically held by a member of the medical staff and responsible for
- Leading EMR system implementation
- Engaging healthcare professionals in the system's development and use
- Leading the group designated to serve as the central governance forum for establishing the healthcare organization's clinical IS priorities.
Server Redundancy
Situation where two servers are duplicating efforts. Helps ensure continuous availability of electronic data in case one server goes down.
Server Failover
At least two, if not more, servers are performing the same processing on data simultaneously.
Implementation Plan
A much more detailed plan that identifies often what is hundreds or more steps to implement each application. The vendor usually supplies a generic plan for how it likes to implement the EHR. It is important to adjust the vendor's plan outlining implementation details with the organization's plan, which will include some of the same and additional tasks.
Migration Path
A series of steps required to move from one situation to another.
Role Based
A security mechanism that grants users of a system based on their role in the organization.
Ex: Nurses have different access than coders.
Type most often used.
User Based
A security mechanism that grants users of a system based on their identity.
Interoperability
The ability of one computer system to exchange data with another computer system.
X12N
Electronic transaction standards of ASC that allow providers and plans or payers to seamlessly transfer data back and forth.
Identity Matching Alogorithm
Rules established in an information system that predicts the probability that two or more patients in the database are the same patient.
A key piece of data needed to link a patient who is seen in a variety of care settings.
Mainframe
A computer architecture built with a single central processing unit to which dumb terminals and/or personal computers are connected.
They can perform millions of instructions per second, are designed to connect input and output devices over long distances, and can handle hundreds or thousands of users at the same time.
Dual Core
A vendor strategy in which one vendor primarily supplies the financial and administrative applications and another vendor supplies the clinical applications.
Best of Breed
A vendor strategy used when purchasing an EHR that refers to system applications that are considered the best in their class.
Best of Fit
A vendor strategy used when purchasing an EHR in which all the systems required by the healthcare facility are available from one vendor.
What basic components make up every electronic network communications system?
- Transmitters
- Receivers
- Media
- Data
Planning and Analysis Phase
A system development life cycle phase.
The first step in adopting new IS technology.
A process for setting IS priorities within an organization and identifying and prioritizing IS needs based on the organization's strategic goals with the intent of ensuring that all IS technology initiatives are integrated and aligned with the organization's overall strategic plan.
Design Phase
A system development life cycle phase.
Specifies the functions of the system and provides the design or blueprint of the proposed system. Describe's the system's hows.
Implementation Phase
A system development life cycle phase.
Includes the development of the computer programs, testing of the system, and development of system documentation, user training, and system conversion.
Maintenance and Evaluation Phase
A system development life cycle phase.
Ensures both the short and long term success of the information system.
Personal Health Record
PHR
Considered a consumer-centric informatics application.
Kiosk
A computer station that promotes the healthcare organization's services.
A place where a patient can schedule appointments, pay bills, obtain education material, signed informed consents, request ROIs, enter health history data using templates, or engage in an e-visit.
Expert System
A knowledge system built from a set of rules applied to specific problems. It can take the place of a human expert when it comes to problem solving. The system simulates the reasoning process of human experts in certain well-defined areas.
Issues Management
The process of resolving unexpected occurrences.
Ex: Late delivery of needed supplies or an uncovered systems problem.
Audit Log
A chronological set of computer records that provides evidence of information system activity (log-ins and log-outs, file accesses) that is used to determine security violations.
An example of metadata.
Metadata
Descriptive data that characterize other data to create a clearer understanding of their meaning and to achieve greater reliability and quality of information.
Data about data.
Systems Testing
The testing of use cases created in the design phase. Testing should also be done using real patient data, not sample data the vendor has provided or the organization has created for training purposes.
Picture Archiving and Communication System
PACS
An integrated computer system that obtains, stores, retrieves, and displays digital images (x-rays).
WORM Technology
Write Once, Read Many
A data storage technology that allows information to be written to a disc a single time and prevents the drive from erasing the data. The discs are intentionally not rewritable, because they are especially intended to store data that the user does not want to erase accidentally.