summary of HIV global epidemic 2020
- 7 mil ppl with HIV in 2020. Steady number
- Aquired in 2020 – 1.5 million
- Ppl dying from HIV related causes – 680,000
- Talked abt the 90-90-90 goal for 2020
- In 2019, had 81% ppl knowing of their HIV infection
- 67% on treatment who know their disease status
- 59% of those ppl achieved viral suppression
Women covered for ART more than men
US density distribution on AIDs view
- Darker = more density of HIV
- SE coast + west coast most
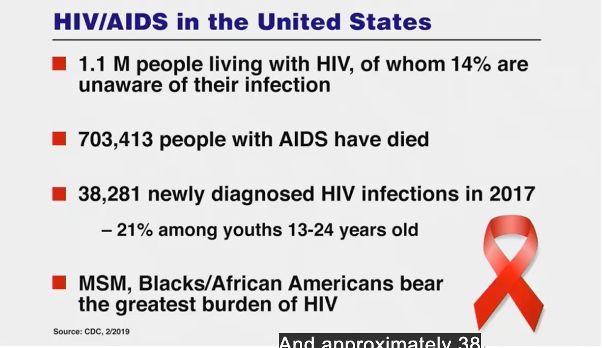
- Populations at risk = MSM = men who have sex with men, African americans
Est HIV incidence
Est HIV incidence
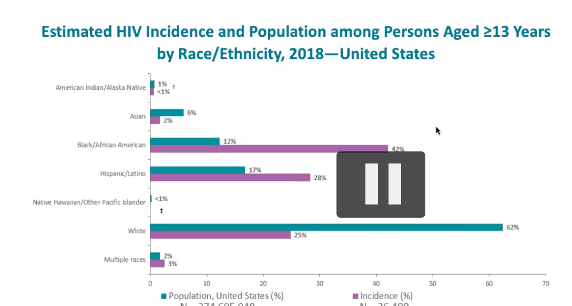
- Demographic % of population in the US compared to their
propotion of having HIV among the groups
- Ex: whites are 62% of the population but make up 25% of the HIV cases
- African americans/blacks are 12% of population, but represent 42% of HIV cases in the US
new HIV diagnoses in US for most affected subpopulations, 2019
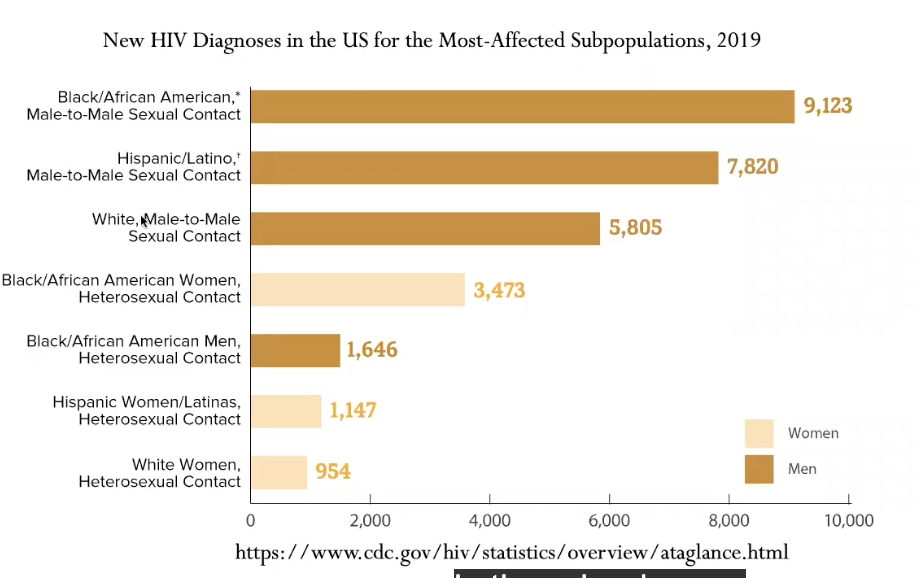
20,000 of 38,000 are MSM
- majority are black/aferican american individuals
New HIV diagnoses in US by age
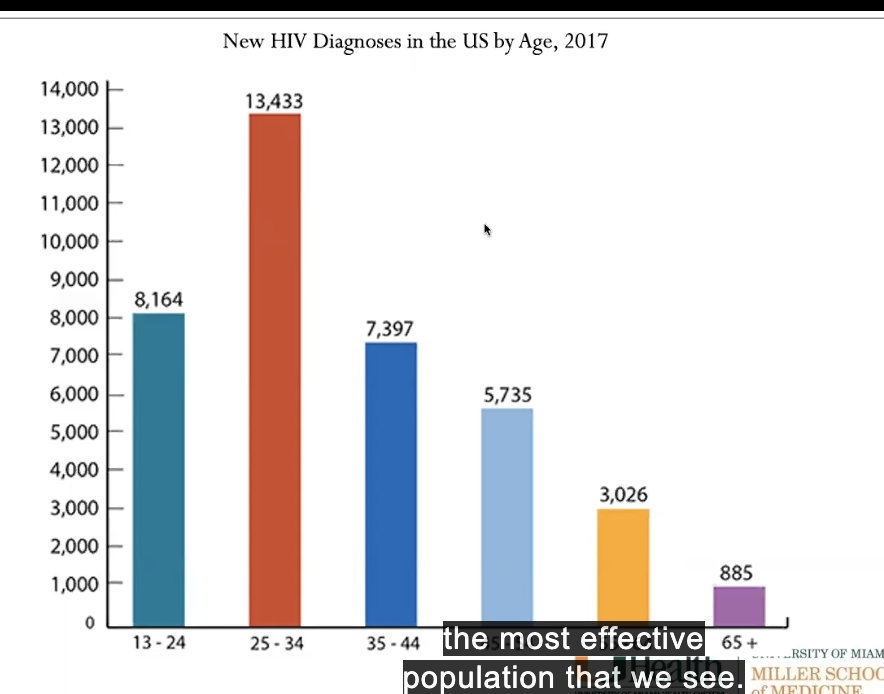
younger ppl dominate - most affected population (25-34 yrs)
HIV diagnosis rate by county of residence
- miami area - highest rate per population (btw 20-43 / 100,000)
- average of US = 12 per 100,000
- miami dade county - epicenter
elements that are critically important that we follow in HIV
- linkage to care
- retention in care
- viral load suppression
pic shows linkage to care within 1 month of HIV diagnosis
darker color = worse
florida is actually better, but still not where want
cont. from last: retention in care
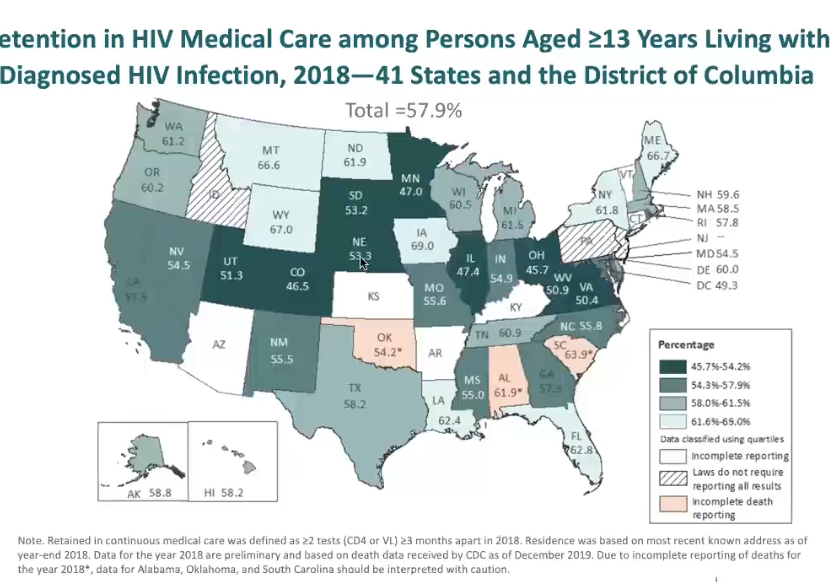
ability to keep ppl in care at least 2x per year
darker color = worse
better in florida, midsection of US worse
cont.: viral load suppression
viral suppression = 200 copies virus/ml (want ppl to be <20 copies now)
darker colors worse
florida not very good in this one (only 62-66% on ARV therapy are suppressed)
some states are bad in all 3
ending the HIV epidemic
a plan for the US
editorial talking abt plan for ending HIV epidemic
- involved all divisions of of health + human services. mostly led by NIH/CDC
FOUND:
- of 3007 counties in the US, over 50% of of HIV infections were in only 48 of these counties
- majority of infections among black/african american and hispanic/latino MSM, high incidence among trans + ppl who use intravenous drugs
- 7 mostly southern states have disproportionate occurrence of HIV in rural areas
US areas with highest burden of HIV diagnosis
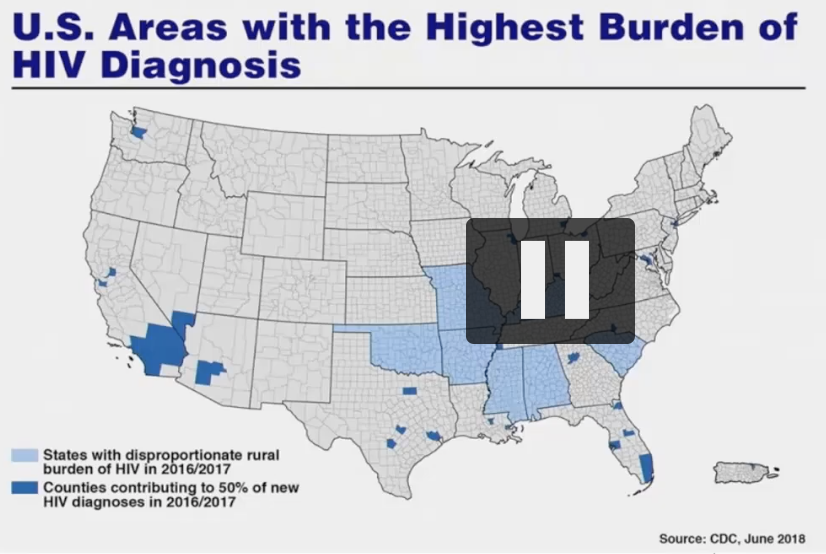
wanna focus on these areas to make biggest impact
how to do that? see next card
-> came up with plan for ending HIV epidemic (plan for america)
75% in HIV infections in 5 years and at least 90% reduction in 10 years
- ambitious goal
sits on 4 pillars:
- diagnose all ppl w/ HIV as early as possible
- treat the infection rapidly + effectively to achieve sustained viral suppression
- protect ppl at risk of HIV using potent and proven prevention and interventions, including PrEP, a medication that can prevent HIV infections
- respond rapidly to detect and respond to growing HIV clusters and prevent new infections
change in criteria for initiating ART
1998 - right after started using combination ARV therapy
used to treat ppl depending on their CD4 cell level, now, treat EVERY INFECTED PERSON POSSIBLE
in 2012, started treating everyhing HIV+ who was willing to take treatment
- now treat right away (earlier than before)
- this
change happened bc some things
- before didnt know all side effects, of resistent, etc.
this changed bc of 052 study that came out (next card)
HPTN 052 study
prevention study
looked at couples where 1 had HIV and 1 did not
randomized control - treatment given to 1 partner
- showed no linked infections when HIV suppressed by ARV therapy
= suppression is critical to transmission (undetectable = untransmittable)
= realized should treat ppl early to prevent transmission
initiation of antirevtroviral therapy in early asynptomatic HIV infection (2011-2015 study)
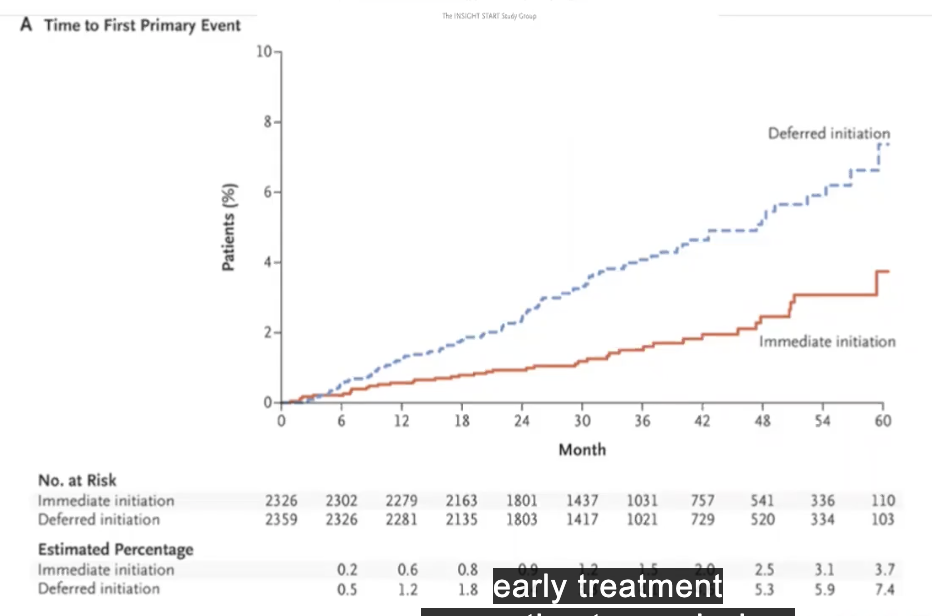
to show whether if start therapy early, compare to started later, does this make better outcome for person?
individual with higher CD4 count had better outcome
primary event cane = death, heart attack, etc.
treat ppl early = prevent time to the first primary event
confirmed early treatment better than waiting
(now know dont just prevent transmission, but allows individual to DO BETTER)
ppl living with HIV (PLWH) in miami-dade county along HIV care continuum
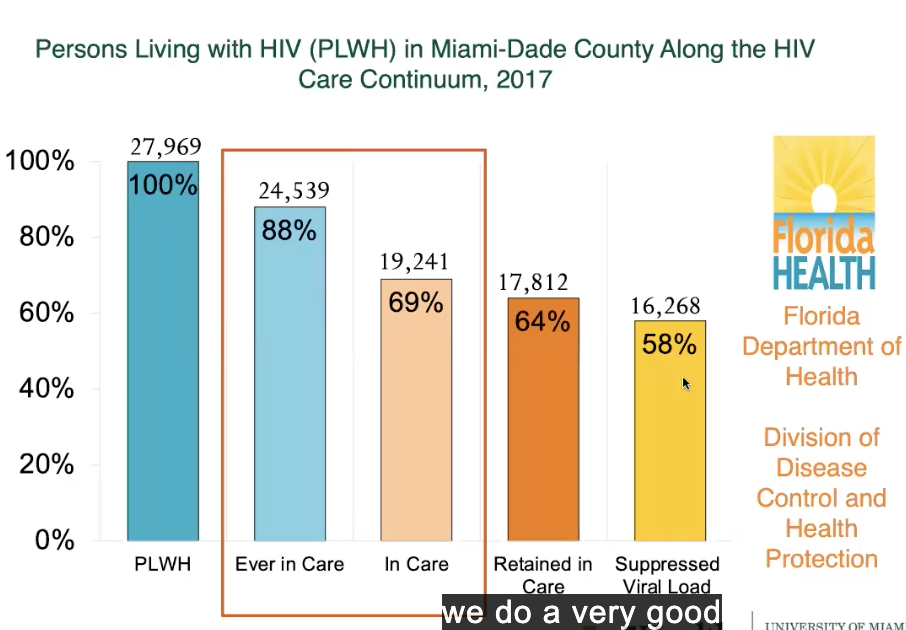
88% ever in care drop 20% (difference) to 69% in care
in care/retained = small difference (69 vs 64%)
and can usually suppress - only 58% of all people living with HIV are virally suppressed
where can make biggest impact? by retaining ppls + getting them into care
caribbean countries - looking for mechanisms to get ppl into care

tried to get ppl treatment quickly after diagnosis
results indicated that ppl able to be taken into care around same day were able to be suppressed
san francisco did same thing
- had clinics where if someone diagnosed w/ HIV -> would sent them same day directly into care so they get started on ARV therapy
doing it early - can suppression quicker = great benefit so can decrease transmission
implemented rapid testing at UM
immediate initiation program in public/academic medical center in the US
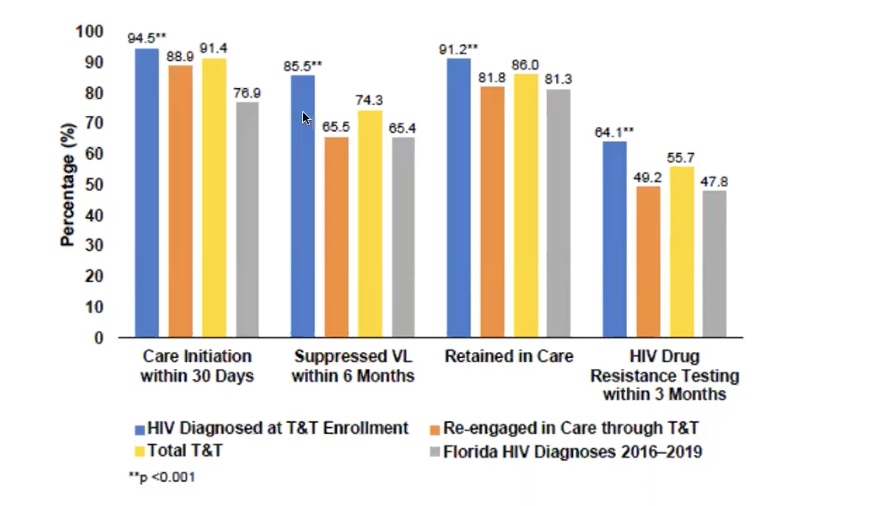
miami test and treat rapid response program
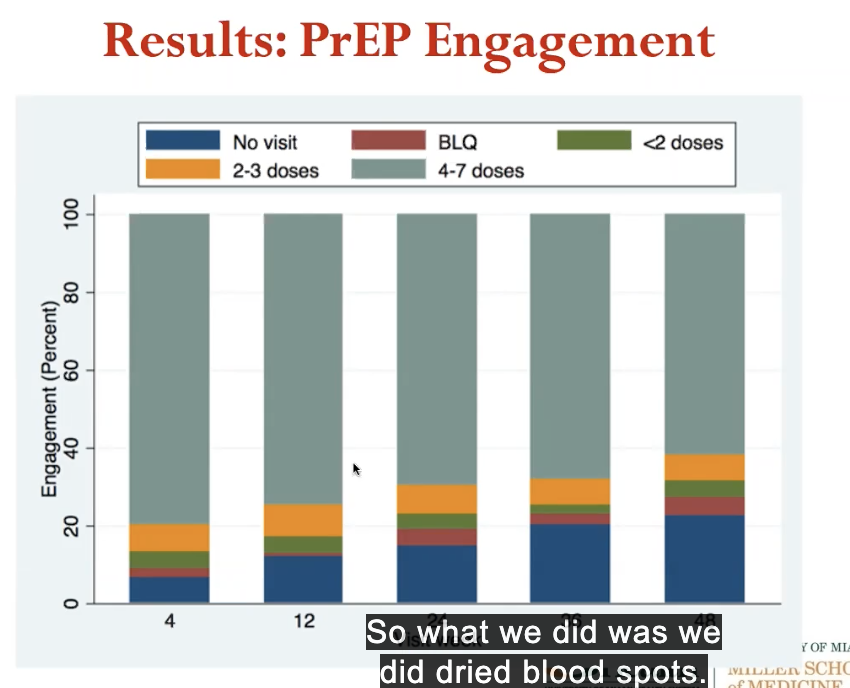
what did this mean for viral load suppression? and impact on our ability to keep them in care?
traditional linkage to care pathway (L)
high acceptability in 1st year
2016 Dr. Hansel worked to get infectious disease elimination act (IDEA) passed at state level
- approved + miami made needle exchange program. very successful
- gives out needle exchange
- decreased # deaths in miami-dade county
rapid identification and investigation of an HIV risk network among ppl who inject drugs - miami Fl 2018
cohort of individuals who tested positive
none got it from eachother, but from other means
important at this time:
- were doing test + treat program
- dr. hansel -> insidivuals diagnosed immediately started on ARV therapy when diagnosed
common btw all studies done: when rapid test + treat ppl, median time for viral suppression after start ARVS is
70 days
even state did test + treat
also brought ppl who fell out of care back in
# ppl who whas care reinitiated, suppressed viral load retained in care, retained in care, etc.
pre exposure prophylaxis (PrEP)
- give ppl treatment to prevent transmission of HIV before get HIV
study - pre exposure chemoprophylaxis for HIV prevention in men who have sex with men
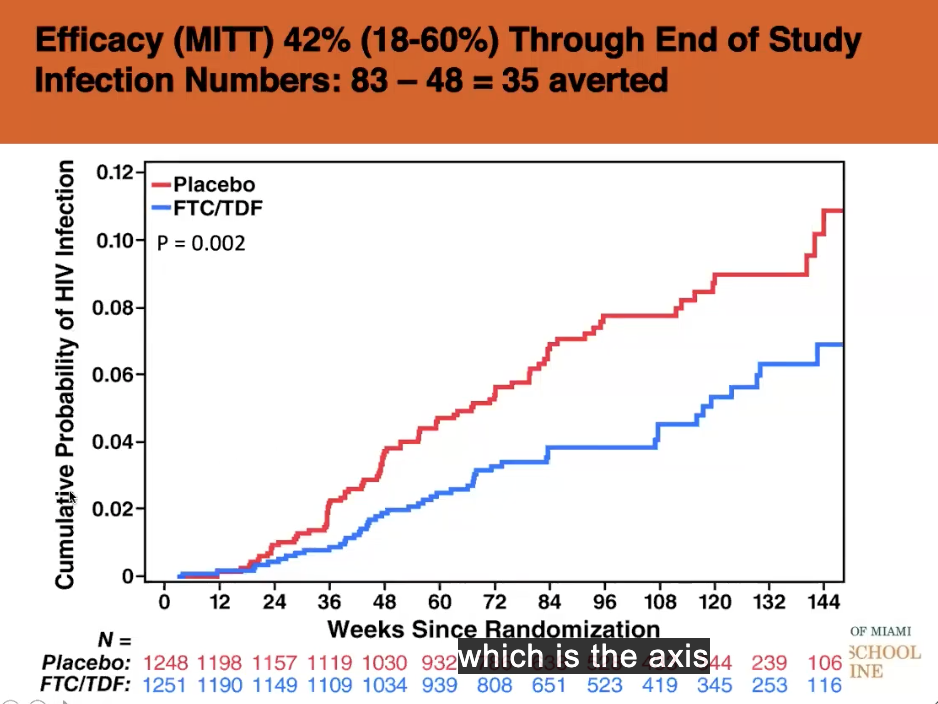
used dual drug - gave in randomized control trial
- either durg or placebo to high risk men
found preexposure prophylaxis DOES prevent HIV aquisition
blue = less aquisition (y axis) compared to placebo (almost 40% difference)
2012 FDA approved 1st drug (dual combination) for use in preventing HIV infection
WHO did the same
didnt know how to make it more effacacious
why do we need PrEP demonstration projects?
- will MSM want PrEP?
- how will MSM use PrEP?
- how will sexual practices change?
- will PrEP be safe in the real world?
= questions in 2012
implementing PrEP in the real world
US PrEP demonstration project
- aids czar contacted kolber + asked if wanted to participate in project in san fransisco regarding PrEP in real world
demo project
NIAID funded PrEP demonstration project
multi site prospective openlabel
wanted to look at 500 at risk individuals in real world setting (MSM and trans women)
offered up to 48 weeks of prEP
in 3 places
- san fransisco city clinic
- STD clinic in miami
- whitman walker clinic
methods
- HIV neg MSM and trans women enrolled oct 2012-jan 2014
- behavioral risk criteria:
- condomless anal sex w/ 2+ partners
- 2+ episodes of anal sex w/ HIV+ partner
- syphylis, rectal gonorrhea, or chlamydia diagnosis
- no serious medical conditions
- offered up to 48 weeks of drug
- follow up
found: graph attached
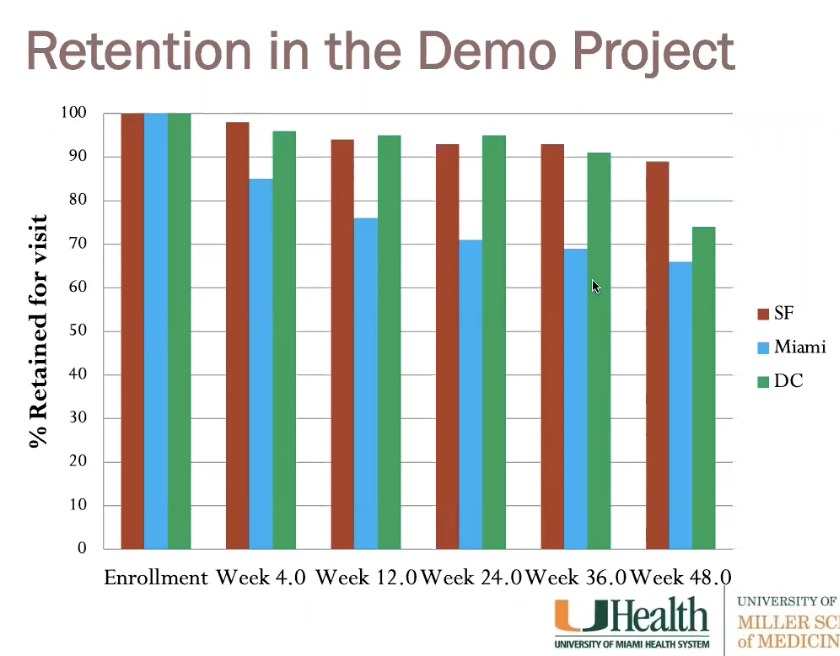
retention in demo project over time
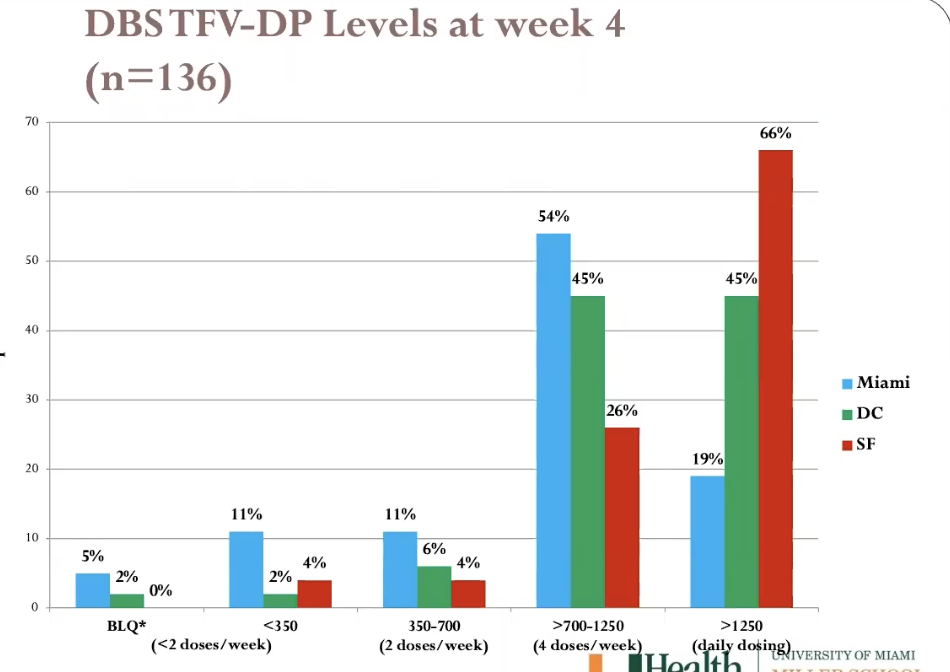
last time gave meds was week 36 (dont count wek 48)
- all consistent and ok except miami (dropped off quick at
first then consistent)
- miami hispanic + younger than other pops
- miami worse at staying on meds
clinical trial evidence for HIV prevention options
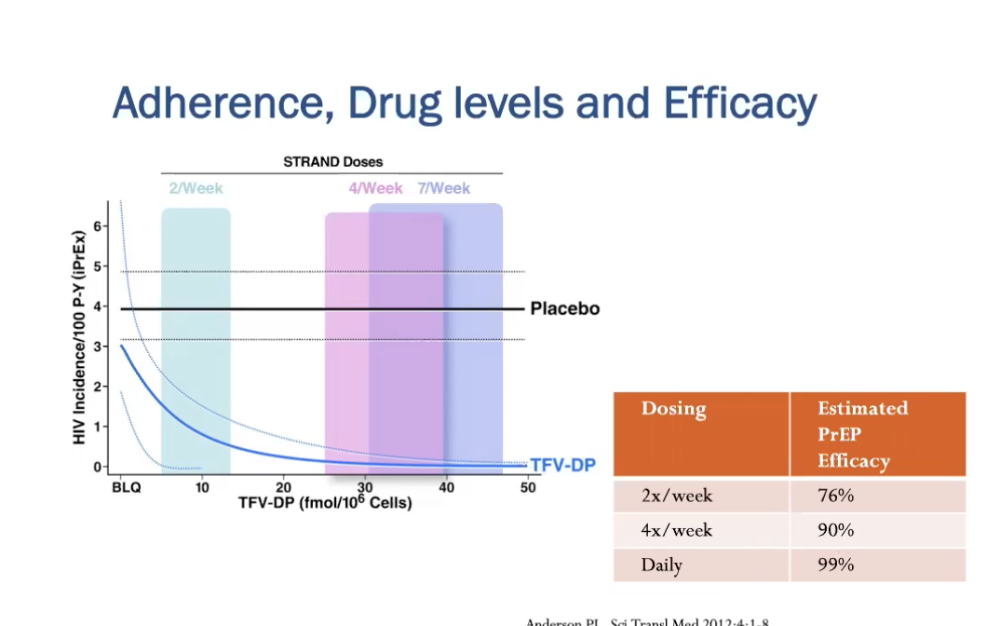
effectiveness/ability to prevent HIV varies a lot
- bc drug level correlates to efficacy
figure:
- x axis - concentration of drug
- y axis - HIV incidence
- blue line = hiv incidence as function of concentration
- abrs reperesent how concentration as function of how many times take it
- only 2x per week = significantly higher hiv incidence than taking it 4 or 7x per week
who should PrEP be offered to?
substantial risk of HIV infection
- MSM
- HIV+ sexual partner
- recent bacterial STI
- high # sex partners
- history of inconsistent/no condom use
- commercial sex work
- heterosexual women/men
- HIV+ sexual partner
- recent bacterial STI
- high # sex partners
- history of inconsistent / no condom use
- commercial sex work
- IDU (intravenous
drug use)
- HIV+ injection partner
- sharing injeciton needles
coverage among perosns aged >16 years
darker = worse
- florida is bad - not a lot of coverage fopr PrEP
HIV PrEP is underutilized
1.1 million individuals in UN at risk for HIV and should be offered PrEP
estimated number of PrEP users end 2018 = 269,000
being PrEPared
- stigma + distrust of medical system prevent at risk ppl of
color from obtaining + benefiting from PrEP
- remember, they are the ones who seem more likely to get it
how many in groups taking it?
HIV prevention pill not reaching most who could potentially benefit - esp african american + latinos
44% ppl who could benefit are african american (500K)
only 1% of those (7K) wre prescribed PrEP
25% ppl who could benefit from PrEP are latino (300K)
only 3% of them (7600) prescribed it
these problems =
overcoming prep adherence problems
need to masintain good drug levels for protection
prep presistence - do ppl stay on or get fatigued?
made injectables, one for PrEP, yet to be approved for it
e
ending aids epidemic
repeated goals again (75% in 5 years and 90% in 10 years)