If a 24-year-old male comes to you and asks if his LDL is good, and
you see that the reference range for Total Cholesterol is <200
mg/dL. He tells you that his LDL
Cholesterol is 181 mg/dL. What
should you tell him?
His LDL is elevated. Look at his Total Cholesterol value, it’s
probably above 200, but might not be, because his HDL is likely low.
<19 mg/dL is really really low, but it’s not out
of the realm
of possibility.
recommended lipid values for: Triglycerides
Optimal: <115 mg/dL
High Risk: >150 mg/dL
recommended lipid values for: Total Cholesterol
Optimal: <170 mg/dL
High Risk:>200 mg/dL
recommended lipid values for: HDL Cholesterol
Optimal: >40 (♂ male) >50 (♀ female) mg/dL
High
Risk:<35 mg/dL
recommended lipid values for: LDL Cholesterol
Optimal: <110 mg/dL
High Risk: >160 mg/dL
A 57-year-old male is admitted from the ED with a myocardial infarction. How many years does it typically take to develop enough atherosclerosis to become a clinical problem?
Answer: Usually, it takes decades of living on this earth for fatty
plaques and fibrous plaques to develop. We can accelerate the
formation of atherosclerosis by eating diets high in saturated fats.
If we desire to have the opposite effect, we can eat a mostly
vegetarian diet (defined as eating meat <2 times per week) and
exercise 2-3 times per week for 30 minutes which will lead to optimal
cardiovascular health. Of course, there are some pathologies which can
promote atherosclerotic development quicker, but we’re just talking
about
run-of-the-mill atherosclerosis here.
A 54-year-old alcoholic male is complaining of diffuse upper abdominal pain and has been having pale gray stools for the past day. What would you expect his triglyceride levels to be?
Answer:
Elevated. Likely this is because alcohol commonly causes
pancreatitis, which then released a ton of triglycerides and caused
the hypertriglyceridemia. This is an example where the etiology of the
hypertriglyceridemia can be discovered, that does NOT always happen though.
What is the cause of FH?
Answer:
A mutation in the gene that regulates either the
receptor or the utilization of
internalized LDL particles in the
peripheral cells. Mammalian cells are required to
have
cholesterol in their cell membranes, so our cells must produce their
own
cholesterol because they can’t take it in from the outside world.
What is the value to be considered severe hypertriglyceridemia?
Answer:
> 500 mg/dL
Comprehension Bite
What is the deficiency in hypoalphalipoproteinemia?
Answer:
HDL-C
1. A 45-year-old white male is complaining of sudden-onset diffuse
abdominal pain. He has eaten the filling of 17 coconuts today and just
can’t get enough. He is found to have an elevated serum triglyceride
level. He is conscientious about his cholesterol and asks if he needs
to lower his HDL-C levels. The physician quickly tells him that he
does not need to lower his HDL, but is worried about what other
life-threatening consequence in this clinical scenario?
A. Acute
Hepatitis
B. Acute Pancreatitis
C. Biliary Cirrhosis
D.
Chronic Pancreatitis
Answer:
The correct answer is B) Acute Pancreatitis. Remember,
hypertriglyceridemia can cause acute pancreatitis when the level goes
above 500 mg/dL. HDL is the good cholesterol, so there really isn’t a
time when we would need to decrease the HDL only.
A 12-year-old female with a family history significant for myocardial infarctions in 6 of the relatives in her direct line. These heart attacks were all in young family members. She presents to the pediatrician with the following sign as shown in Image 1. In what component of the cholesterol pathway is the likely mutation in this patient if her total cholesterol levels are about 600 mg/dL?
A 12-year-old female
A. HMG-CoA Reductase
B.
Cholesterol Oxidase
C. LCAT
D. LDL Receptor
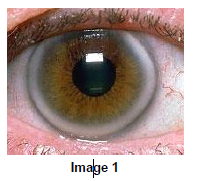
The correct answer is D) LDL Receptor. This patient likely has Familial Hypercholesterolemia (FH), an uncommon, but commonly tested cholesterol abnormality. The patients don’t have the proper genes to use the LDL particles (i.e. they can’t bring them into their cells). Because of this, the blood level of LDL remains extremely high. These patients can have their first heart attack as teenagers. There are several mutations which will cause this but just know that this is caused by an inability for the body to take in the LDL molecule into their cells and use it.
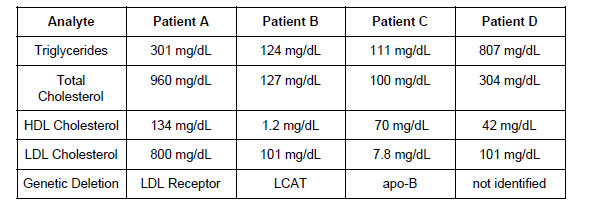
3. The physician on call is given a lipid panel for one of his partner’s patients with hypobetalipoproteinemia. He gets the results mixed up with another patient You offer to help out, which patient has hypobetalipoproteinemia?
A. Patient A
B. Patient B
C. Patient C
D.
Patent D
Answer:
The correct answer is Patient C. This patient has
hypobetalipoproteinemia, which is seen by the genetic deletion of
apo-B which associates itself with LDL-C. This deletion does not allow
for the LDL receptors to recognize the LDL particle with the apo-B
wrapped around it.
Patient A has Familial Hypercholesterolemia.
Patient B has hypoalphalipoproteinemia.
Patient D has Primary Hypertriglyceridemia.
What is the primary function of free fatty acids?
Answer:
Provide the body with tons and tons of energy
As far as apolipoproteins are concerned what is the definition of: Absorption?
lipids that are absorbed from the diet and contain Apo B48
As far as apolipoproteins are concerned what is the definition of: Exogenous?
chylomicrons travelling to the liver in the lymphatics that are newly
created from
the absorbed micelles in the intestinal cells and
contain Apo B-100
As far as apolipoproteins are concerned what is the definition of:Endogenous -
Triglycerides packaged by the liver into VLDL for circulation around
the body
and contain Apo B-100
As far as apolipoproteins are concerned what is the definition of: Reverse -
Cholesterol and Fatty Acids being transported from the peripheral tissues for excretion in the bile and contain Apo A-I and Apo A-II
What is the nomenclature need to know for the following lipoproteins: Chylomicrons
- Apo B-48
Note: Chylomicrons are large triglyceride-rich lipoproteins produced in enterocytes from dietary lipids—namely, fatty acids, and cholesterol. Chylomicrons are composed of a main central lipid core that consists primarily of triglycerides, however like other lipoproteins, they carry esterified cholesterol and phospholipids.
What is the nomenclature need to know for the following lipoproteins: VLDL
- Apo B-100, Apo A-I, Apo C-II, Apo E
stands for very low density lipoprotein. Lipoproteins are made up of cholesterol , triglycerides, and proteins. They move cholesterol, triglycerides, and other lipids (fats) to around the body. VLDL is one of the three main types of lipoproteins. VLDL contains the highest amount of triglycerides.
What is the nomenclature need to know for the following lipoproteins: IDL -
Apo B-100, Apo-E
What is the nomenclature need to know for the following lipoproteins: LDL
- Apo B-100
LDL (low-density lipoprotein) cholesterol, sometimes called “bad” cholesterol, makes up most of your body's cholesterol. High levels of LDL cholesterol raise your risk for heart disease and stroke.
What is the nomenclature need to know for the following lipoproteins: HDL
- Apo A-I, Apo A-II, Apo C-II, Apo E
HDL (high-density lipoprotein) cholesterol, sometimes called “good” cholesterol, absorbs cholesterol in the blood and carries it back to the liver. The liver then flushes it from the body. High levels of HDL cholesterol can lower your risk for heart disease and stroke.
What apolipoprotein tells your body when it’s attached to a fat bag
full of fat,
that it is going to the peripheral tissues?
Answer: Apo B-100
A 32-year-old male runner who eats primarily a Mediterranean diet has an HDL of 55 mg/dL and the value is so low that the machine can’t register a value for LDL. What happened?
This would be expected. An HDL value elevated above the LDL value is what happens in athletes that eat mostly fruits and vegetables and little meat. This is the most optimal circumstance for this man’s cardiovascular health. Of note, estrogen causes HDL-C to be increased so the reference range for women is about 10 mg/dL higher than the range for men. A higher HDL level confers better cardiovascular health for premenopausal women. This advantage disappears after menopause and the cardiovascular risks for females become equal to that of males.
The cholesterol oxidase method has there three steps.
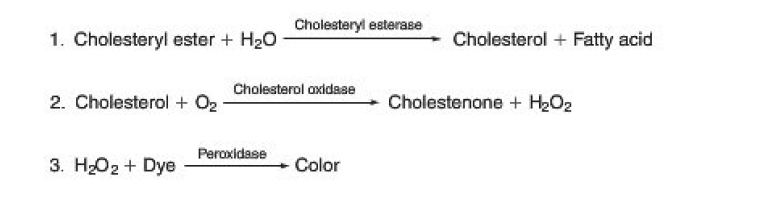
This is a three-step method which produces hydrogen peroxide and a color change from cholesterols.
Calculate the LDL value if the Tchol is 170 mg/dL, HDL-C is 35 mg/dL, and TRIG is 75 mg/dL
120 mg/dL
What do lipids do?
Lipids serve as
1.Energy Storage
2.Membrane Structure
3.Cell Signaling Molecules
Lipids are insoluble in water
What are Clinically Significant: esters?
1.Triglycerides
2.Phospholipids
What are Clinically Significant: Sphingosine derivatives?
1.Sphingomyelin
2.Glycosphingolipids
What are Clinically Significant: Terpenes ?
1.Vitamins A, E, K
What are tags for lipoprotein called?
apolipoproteins
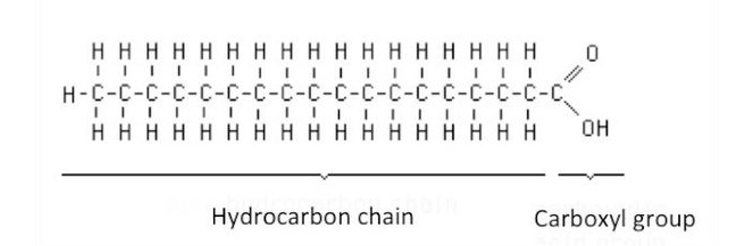
What are Saturated fatty acids ?
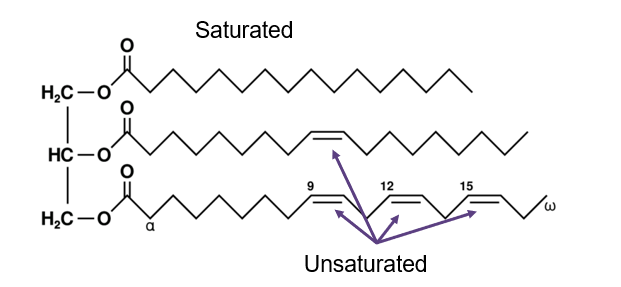
contain an alkyl chain WITHOUT a double bond.
note:
There is no more room to stick any more hydrogen on that chain It is “saturated” with hydrogen
What are Unsaturated fatty acids?
- contain an alkyl chain WITH a double bond
There is room to stick more hydrogen on that chain It is “unsaturated” with hydrogen
What are the 4 clinically significant lipids?
1.Cholesterol
2.Steroid hormones
3.Bile acids
4.Vitamin D
Where does Exogenous cholesterol come from?
it's absorbed from Diet
Where does Endogenous cholesterol come from?
it's produced by the Liver
What is the Apolipoprotein: Apo A-I, A-II =
Chylomicrons and HDL-C - associated with getting lipids into the blood
What is the Apolipoprotein: Apo B-48 =
Chylomicrons, to be shipped from the intestines to the liver
What is the Apolipoprotein: Apo B-100 =
= LDL-C, to be shipped to the periphery and deposited in blood vessels, liver, and muscle...high levels are correlated with risk of myocardial infarction
What is the Apolipoprotein: Apo C-I, C-II, and C-III =
Chylomicrons, HDL-C, and VLDL-C - only found in the extremes of lipid concentrations in lipoproteins (e.g. very high and very low), involved in transfer for the endogenous cholesterol pathway
What is the Apolipoprotein: Apo E =
Chylomicrons and HDL-C (there are others, but these are the important ones to understand) To help me remember, E stands for Exogenous
What is the major role of HDL-C
to maintain an equilibrium of cholesterol
What are most fatty acids bound to?
glycerol forming esters
What is the cause of familial hypercholesterolemia?
A mutation in the LDL-R gene that regulates either the receptor or the utilization of internalized LDL particles in the peripheral cells. Mammalian cells are required to have cholesterol in their cell membranes, so our cells must produce their own cholesterol because they can’t take it in from the outside world.
What are the sign and symptoms of Hypocholesterolemia?
Hyperthyroidism
Hepatic Failure
Malnutrition / Anemia
Starvation / Anorexia
Abetalipoproteinemia
What are the sign and symptoms of Hypertriglyceridemia?
Hypertriglyceridemia can cause Acute Pancreatitis and Acute Pancreatitis can cause hypertriglyceridemia
Can occur because of Acute Alcoholism
High fat meal (lipemic specimens)
Hereditary hypertriglyceridemia
What is Lipoprotein (a) [Lp (a)] a risk factor for?
An independent and very significant risk factor for Coronary Artery Disease (CAD)
Physiologic role is undefined, but an association with CAD has been identified
If a child comes into the ER with an icteric sample and the physician orders a cholesterol assay for some unbeknownst reason, what method(s) would result in a positive interference?
Bilirubin significantly decreases all enzymatic cholesterol assays
What are the reference values and risk factors for the National Cholesterol education program?
- Cigarette smoking
- BP ≥140/90
- HDL <40 mg/dL
- Family history of coronary heart disease
- Age ≥45 men ≥55 women
The higher CAD risk, the lower the LDL goal
what are the values to be aware of for this risk category:
High risk: CHD or CHD risk equivalents (10-year risk >20%)
LDL cholesterol goal: <100 mg/dL
Initiate lifestyle changes: >100 mg/dL
Consider drug therapy: >100 mg/dL
what are the values to be aware of for this risk category:
Moderate risk: two or more risk factors (10-year risk <10%)
LDL cholesterol goal: <130 mg/dL
Initiate lifestyle changes: >130 mg/dL
Consider drug therapy: >160 mg/dL
what are the values to be aware of for this risk category:
Low risk ≤1 risk factor
LDL cholesterol goal: <160 mg/dL
Initiate lifestyle changes: >160 mg/dL
Consider drug therapy: >190 mg/dL
What are the Independent Risk Factors for CAD?
HDL-C <40 mg/dL
Age >45(men) >55(women)
Family History of Coronary Artery Disease
Blood Pressure >140/90
Diabetes
Cigarette smoking
What would you expect your blood lipid levels to be in intestinal malabsorption ?
Low
What would you expect the stool lipid levels to be in intestinal malabsorption?
High. Because they’re flowing right through without being absorbed.
How does bile flow effect plasma lipid levels?
Bile acids allow us to emulsify and absorb fats from our food
Remember also, that lipids are removed from the body in the bile
Note: This can tip the balance toward lipid deposition
Excessive elimination of cholesterol can lead to gallstone formation
In pregnancy what happens to lipid levels?
HDL-C, LDL-C, and Triglycerides all increase
However, the HDL-C/LDL-C ratio remains the same
What is Gaucher disease?
Glucocerebrosidase deficiency
Fats collect in the spleen, liver, kidneys, lungs, brain, and bone marrow
It’s a lipid storage disease, so what do you think it does to fat levels? It increases them!
Symptoms are painless splenomegaly, anemia, or thrombocytopenia and occasionally seizures
What is Niemann-Pick Disease?
Sphingomyelinase deficiency (Memory Trick: Pick your nose with your sphinger)
Autosomal recessive disorder caused by accumulation of lipids in the liver, spleen, bone marrow, lungs, and brain
Neurologic complications include ataxia: can’t walk, eye paralysis, brain degeneration, hypersensitivity to touch
Characteristic cherry-red spot develops in the retina
What is Fabry Disease?
Alpha galactosidase A deficiency
Deposits fats in the autonomic nervous system, eyes, kidneys, and cardiovascular system
Fabry disease is the only X-linked lipid storage disease, so it primarily affects only Males, Females can be affected though, usually with a milder form
Renal failure is common, so kidney transplants or dialysis are also frequently used
Enzyme replacement can be an effective therapy
What is Tay-Sachs Disease?
Classified as a GM2 gangliosidosis which is usually a storage of fats in nervous tissues
Memory Trick: Tay-Sa(x) Disease = He(x)oseaminidase deficiency
Symptoms include progressive loss of mentation, dementia, sensorineural hearing loss, blindness, and also a cherry red spot on the macula
Typically occurs in young children and death is usually caused by bronchopneumonia
What are the historic methodologies for HDL?
Dextran sulfate with MgCl2 and the Lieberman-Burchard method using acetic anhydride
What are the modern methodologies for HDL?
Enzymatic methods are commonly performed in today’s laboratories
HDL > 60 mg/dL is desired
HDL < 40 is a risk factor for CAD
What are the important reference ranges to memorize
Total Cholesterol: 140-200 mg/dL (3.6-5.2 mmol/L)
HDL-C: 40-75 mg/dL (1.0-2.0 mmol/L) tip 4 Head, at 75 your Helpless.
LDL-C: 50-130 mg/dL (1.3-3.4 mmol/L) Tip: roman numeral L= 50, 13 in unLucky
Triglycerides: 60-150 mg/dL (0.7-1.7 mmol/L) tip: tri X 20 to 50 times to get right
A 58-year-old obese male presents to the clinic with shortness of
breath upon mild exertion. He is a farmer and has eggs, bacon, cheese,
toast, and milk every day for breakfast. He needs to milk the cows at
5 am, but hasn’t been able to get enough energy to do that for the
last few weeks. He never goes to the physician because his body is
“tough enough to handle anything”. He gets a lot of exercise, doing
farm work all day long, but doesn’t eat the healthiest diet. He has
multiple servings of beef and pork each day and not many vegetables.
What would you
expect his HDL and LDL levels to be?
A. HDL
25 mg/dL LDL 110 mg/dL
B. HDL 35 mg/dL LDL 250 mg/dL
C. HDL
75 mg/dL LDL 275 mg/dL
D. HDL 210 mg/dL LDL 70 mg/dL
The correct answer is B) HDL 35 mg/dL and LDL 250 mg/dL. A poor diet
is the number one influencing factor on cholesterol in our blood. This
is not only mediated by his lack of vegetable consumption, but more
importantly, he is over-consuming beef and pork … just like 90% of
America. He gets adequate exercise, which increases HDL and decreases
LDL. However, his diet overshadows this positive effect on HDL. Answer
A) is rare and would be seen in hypoproteinemia and an inability to
form the
apolipoproteins. Answer C) is commonly seen in pregnant
or recently postpartum females who have a diet rich in saturated fat.
Answer D) is not a common plausible
pathology so you don’t need
to worry about it. Usually, if HDL is greater than LDL, that is a good
thing, but it’s usually pretty close like HDL 60, LDL 40.
A 74-year-old Female presents to her community physician, whom she
has never seen before, and was googling triglycerides. She wants to
know if she is at risk for pancreatitis. The physician agrees to
perform the test for her because it has been years since she last had
her
lipid testing done. Her results come back as:Tchol 201 mg/dL
HDL-C 38 mg/dL LDL-C 123 mg/dL TRIG 198 mg/dL Which one is the
calculated result?
A. Tchol
B. HDL-C
C. LDL-C
D. TRIG
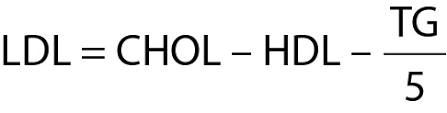
The correct answer is C) LDL-C. This is calculated by the Friedewald
calculation which requires values for all the other components of the
lipid panel. Here is the equation:
LDL-C = Tchol - HDL-C - (TRIG
/ 5) LDL-C = 201 mg/dL - 38 mg/dL - (298 mg/dL /5) = 123.4 mg/dL
What apolipoproteins confer an increased risk to the patient?
A.
Apo A-I B. Apo B-100 C. Apo B-48 D. Apo C-II E. Lp(a)
A. A, C,
D
B. B, E
C. C, D
D. D, E
The correct answer is B) B, E. Apo B-100 and Lp(a) are poor markers
for health. Apo B-100 is the apolipoprotein that tells the body to
take this bag of lipids to the tissues.
Lp(a) is a small particle
associated with Apo B-100. Lp(a) is a particle with higher lipid
content than LDL-C, is slightly larger, and significantly contributes
to the risk for coronary artery disease and strokes.
What is the specimen of choice for HDL-C testing?
Serum from a fasting specimen, this is commonly collected in a serum separator tube
If a child comes into the ER with an icteric sample and the physician
orders a cholesterol assay for some unbeknownst reason, what method
would give you a
false reaction?
Cholesterol oxidase