SWM Module 15: Assessing the Wound — Lower Extremity Ulcers
What Is a Lower Extremity Ulcer?

Lower extremity ulcers are open sores or ulcers occurring on the lower legs, typically below the knee (DynaMed, 2022).
Frequently encountered types of lower extremity ulcers include:
- Venous leg ulcer (VLU)
- Arterial leg ulcer
- Diabetic foot ulcer (DFU)
- Mixed venous and arterial leg ulcers
Lower extremity ulcers: Primary causes include
- Chronic Venous Insufficiency (CVI) or (lower extremity venous disease - LEVD)
- Arterial Disease (lower extremity arterial disease - LEAD) or (peripheral arterial occlusive disease - PAOD)
- Diabetes (Neuropathic)
Lower extremity ulcers result from-
underlying conditions impairing blood flow
tissue oxygenation
and skin integrity
Other causes of lower extremity wounds can include:

- Pressure injuries
- Infections
- Malignancies
- Trauma
- Insect bites
- Sickle cell anemia
- Pyoderma Gangrenosum
- Vasculitis
Identifying Lower Extremity Ulcers:
Identify the Cause
Accurate diagnosis allows for tailored treatment, addressing issues like poor circulation, arterial disease, or diabetes to promote healing and avoid missteps like inappropriate treatment.
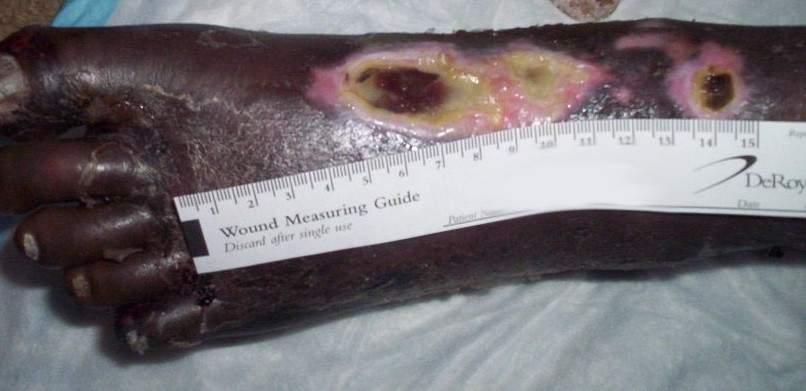
What type of ulcer is this?
Arterial ulcer

What type of ulcer is this?
Diabetic foot ulcer

What type of ulcer is this?
Venous leg ulcer
Review of Past Ulcers
Rate of Recurrence
Many occurrences might indicate chronic issues (e.g., ____ _____).
venous insufficiency
Previous Medical History:
Kidney Disease: Renal failure
is often linked with poor wound healing and increased risk of ulcers.
Review of Past Ulcers: Autoimmune Disorders: Autoimmune diseases
like rheumatoid arthritis or lupus can impact skin integrity and healing. These patients are often on anti-inflammatory/steroid medications which can impair the inflammatory phase of wound healing.
Lifestyle Factors
Certain modifiable lifestyle factors that increase the risk for ulcers and poor healing should be assessed to see if the patient needs to be coached in these areas (McNichol et al., 2021):
- Smoking or Vaping: Nicotine impairs blood flow and increases the risk of blood clots and infection (Troiano et al., 2019).
- Nutrition: Poor nutrition hinders wound healing and immune response.
- Physical Activity: A decreased activity level can lead to poor circulation and increase the risk of ulcers.
Diabetes
Poorly controlled diabetes can lead to neuropathy and impaired healing. Thus, it is important to assess for (Baranoski & Ayello, 2020; McNichol et al., 2021):
- Glycemic Control: Hyperglycemia negatively impacts healing by prolonging the inflammatory phase and decreasing the immune system's efficiency.
- Diabetic Neuropathy: Loss of sensation, tingling, or numbness in the extremities increases the risk of unseen injuries and subsequent ulcers.
- Glycemic Control:
Hyperglycemia negatively impacts healing by prolonging the inflammatory phase and decreasing the immune system's efficiency.
- Diabetic Neuropathy:
Loss of sensation, tingling, or numbness in the extremities increases the risk of unseen injuries and subsequent ulcers.
Hypertension
Poorly controlled blood pressure (BP) can contribute to poor circulation and delayed healing (WOCN, 2024).
Peripheral Vascular Disease
Assess for the following in patients suspected of having peripheral vascular disease (PVD) (McNichol et al., 2021):
- History of Claudication: Pain, cramping, or complaints of fatigue in the legs during physical activity that is relieved within 10 minutes of rest can indicate PVD. Intermittent claudication is considered the most typical symptom of LEAD, but most patients are asymptomatic.
- Nocturnal or Positional Pain: Occurs in the absence of activity. Sleep is affected by throbbing pain with leg elevation that is relieved by dangling affected leg(s) in a dependent position.
- Previous Vascular Interventions: Record past vascular procedures such as angioplasty, stenting, or bypass surgery.
Pain, cramping, or complaints of fatigue in the legs during physical activity that is relieved within 10 minutes of rest can indicate PVD. Intermittent claudication is considered the most typical symptom of LEAD, but most patients are asymptomatic.
- History of Claudication:
Occurs in the absence of activity. Sleep is affected by throbbing pain with leg elevation that is relieved by dangling affected leg(s) in a dependent position.
- Nocturnal or Positional Pain:
Cardiff Wound Impact Schedule
_____ was designed and validated to specifically assess the HRQoL of subjects with chronic wounds (Granado-Casas, et al., 2021). It helps healthcare providers understand how wounds affect various aspects of a patient’s daily life.
The Cardiff Wound Impact Schedule (CWIS)
- Demographic and clinical characteristics
- Global HRQoL
- Satisfaction with HRQoL
- Impact of the wound on lifestyle
The ____-__quickly evaluates the impacts of various chronic wounds on a person’s HRQoL. Its brevity, ease of use, and availability in multiple languages make it highly suitable for clinical practice. (Janke et al., 2024).
The Wound-QoL
The Wound-QoL quickly evaluates the impacts of various chronic wounds on a person’s HRQoL. Its brevity, ease of use, and availability in multiple languages make it highly suitable for clinical practice. (Janke et al., 2024).
It is comprised of 17 questions covering three domains including-
- Physical symptoms
- Psychological well-being
- Everyday life

Edema:
Assessing whether the edema is in one or both LEs can help determine if the cause is a systemic disease affecting the entire body (e.g., heart failure) or related to a condition that affects part of the body (e.g., venous insufficiency) (DynaMed, 2023).
Edema presents in the lower extremities as non-pitting or pitting.
- Non-Pitting Edema: Often caused by conditions like lymphedema or thyroid disorders
- Pitting Edema: Often associated with venous insufficiency, congestive heart failure, or kidney disease
Often caused by conditions like lymphedema or thyroid disorders
Non-Pitting Edema
Often associated with venous insufficiency, congestive heart failure, or kidney disease
Pitting Edema
Pitting Edema: Grade 1
Indicates mild pitting edema with a slight indentation that is barely noticeable and about 2 mm deep, disappearing almost immediately.
Pitting Edema: Grade 2
Is moderate pitting edema with a deeper indentation, about 3 to 4 mm, disappearing within 15 seconds.
Pitting Edema: Grade 3
Is moderately severe pitting edema with a noticeably deep indentation, about 5 to 6 mm, remaining for more than 15 seconds but less than 1 minute.
Pitting Edema: Grade 4
Grade 4
Grade 4 indicates severe pitting edema with a very deep indentation, about 8 mm or more, remaining for 2 minutes or longer.

Periwound assessment:
Hyperpigmentation, shiny taught skin, no hair growth, thickend, evidence of scaling, and ulceration present
Sensory Testing- purpose
Sensory testing is important to determine if patients can detect pain, pressure, and temperature changes, especially for those with diabetes (McNichol et al., 2021). Tests include:
Semmes-Weinstein Monofilament Test
This checks for protective sensation in the feet using a 10G monofilament (McNichol et al., 2021). The monofilament is pressed against the bottom of the foot until it bends. Ask the patient to close their eyes while you perform the test and have them say “yes” each time they feel the pressure from the monofilament.
Tuning Fork Test and Temperature Assessment
The following is the procedure for performing the assessment:
- Instruct the patient to close their eyes to eliminate visual input.
- Strike the tuning fork firmly against the palm of your hand to initiate vibration (it should vibrate for approximately 30–40 seconds).
- Apply the vibrating fork to a familiar bony area—such as the forehead, sternum, or arm—to ensure the patient understands what the vibration sensation feels like (as distinct from touch).
- Place the vibrating tuning fork on the bony prominence of the great toe, just below the nail bed.
- Ask the patient if they feel the vibration.
- Stop the vibration (e.g., by touching the tines) and immediately ask the patient if they feel the loss of vibration.
- If the patient does not feel vibration at the toe, repeat the test on more proximal sites, such as the mid dorsum of the foot and the lateral malleolus.
Tuning Fork Test and Temperature Assessment
A 128 Hz tuning fork is used to test for vibratory sensation loss, which indicates large fiber nerve damage (McNichol et al., 2021).
Achilles Tendon Reflex
Test the Achilles tendon reflex by gently tapping the Achilles tendon with a reflex hammer while the patient’s foot is dorsiflexed (WOCN, 2024). The procedure is:
- With the patient seated, place one hand on the plantar foot and passively dorsiflex the ankle to a right angle.
- Tap the Achilles tendon gently with a reflex hammer.
- A normal response is plantar flexion of the foot (like pressing a gas pedal).
A diminished or absent Achilles reflex may suggest peripheral neuropathy. While this reflex is typically present in healthy individuals, it often decreases with age. Bilateral absence in older adults may not be clinically significant.
Test the Achilles tendon reflex by gently tapping the Achilles tendon with a reflex hammer while the patient’s foot is dorsiflexed (WOCN, 2024).
Achilles Tendon Reflex
The procedure is:
- With the patient seated, place one hand on the plantar foot and passively dorsiflex the ankle to a right angle.
- Tap the Achilles tendon gently with a reflex hammer.
- A normal response is plantar flexion of the foot (like pressing a gas pedal).
A diminished or absent Achilles reflex may suggest peripheral neuropathy. While this reflex is typically present in healthy individuals, it often decreases with age. Bilateral absence in older adults may not be clinically significant.
Pulse Check: Dorsalis pedis:
Located on the top of the foot, between the first and second metatarsal bones.
Pulse Check: Posterior tibial:
Located behind the medial malleolus.
PULSE INTESITY RECORD
0
1
2
3
0 = ABSENT
1 = DECREASED
2 = NORMAL
3 = BOUNDING
* A strong pulse indicates good blood flow
Normal capillary refill should be less than _____.
2 seconds.
A delayed refill time of over ___ may indicate poor perfusion (WOCN, 2024).
3 seconds
TRUE / FALSE
Capillary refill can be affected by temperature and should not be used exclusively to determine blood flow to the LEs.
True

What does this image display
Dependent Rubor
Patients with ___ or ____ _____ will exhibit pallor and dependent rubor after returning to an upright position with their legs dangling.
PAD ; limb ischemia
If there is critical limb ischemia (CLI), the limb will become pale at or before __ elevation
20°
Elevation Phase:
With the patient lying supine, raise their legs to about ___. If pallor is noticeable within 30 seconds, it indicates relevant ischemia
45-60°
What is reactive hyperemia?
After assessing pallor, have the patient sit up with their legs in a dependent position. If their legs slowly revert to their normal color, followed immediately by an intensely red coloration when dependent, this is known as reactive hyperemia, and the leg will eventually return to its normal color after a few minutes
The development of dependent rubor indicates that there is some ___ present that requires further diagnostic testing.
ischemia
* Vascular referral may be necessary
Common noninvasive diagnostic tests for the lower extremities include (Bryant & Nix, 2024):
- Transcutaneous Oxygen Measurement (TCPO2)
- Skin Perfusion Pressure (SPP)
- Near Infrared Light (NIR)
- Ankle-Brachial Index (ABI)
- Toe-Brachial Pressure Index (TBPI)
- Doppler Waveform Analysis
- Segmental Limb Pressure
- Pulse Volume Recording (PVR)
- Color Duplex Imaging
What is TCPO2?
Assesses blood flow by measuring the partial pressure of oxygen at the periwound skin surface using special sensors
TCP02 Range
> 40 mmHg = Normal
30 to < 40 mmHg = Borderline ischemia
< 30 mmHg = Critical limb ischemia
Memory :
___ Normal
___ Borderline ischemia
___ Critical limb ischemia
TCP02 Interpretation
Parameters for Normal?
> 40 mmHg
TCP02 Interpretation
Parameters for Borderline ischemia?
30 to < 40 mmHg
TCP02 Interpretation
Critical Limb Ischemia?
< 30 mmHg
This test is often done with an oxygen challenge to determine if the patient may benefit from hyperbaric oxygen therapy.
Echo
Pedal Pulse
TCPO2
SPP
Abbreviations:
TCPO2 is
Transcutaneous Oxygen Measurement
Abbreviations:
SPP
Skin Perfusion Pressure
Abbreviations:
NIR
Near Infrared Light
Abbreviations:
ABI
Ankle-Brachial Index
Abbreviations:
PVR
Pulse Volume Recording
Abbreviations:
TBPI
Toe-Brachial Pressure Index
Skin Perfusion Pressure:
It can be used on ____ __ and is helpful for predicting ulcer healing or planning amputation level to maintain maximal functioning and mobility
noncompressible arteries
The ____ uses a cuff with a laser Doppler sensor to identify the point at which blood flow resumes when the cuff is deflated.
The skin perfusion pressure (SPP)
SPP Range are:
1.
2.
3.
1. > 50 mmHg
2. 30 to < 50 mmHg
3. < 30 mmHg
SPP Ranges: Interpretations
> 50 mmHg =
30 to < 50 mmHg =
< 30 mmHg =
Normal , PAD , Severe PAD
SPP Range
A pressure exceeding __ mmHg is required for healing
30 mmHg
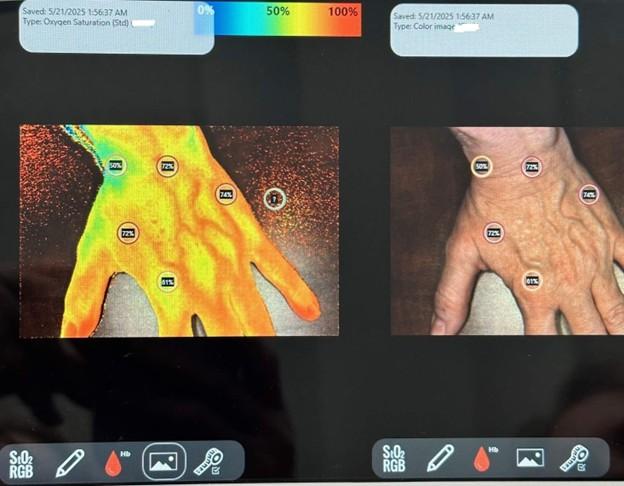
Near-Infrared Light, or NIR
It is a noninvasive method that quantifies microcirculation and healing potential, photographs the wound, and measures the wound surface area.
Technology incorporating ______ assists with detecting oxygenated and deoxygenated blood, conveying a comprehensive picture of the health of the tissues and healing capacities.
NIR
What is Ankle-Brachial Index (ABI)?
It is standard of care to check the perfusion of a leg before applying any compression.
How is ABI calculated?
It is calculated by dividing the ankle's systolic blood pressure (SBP) measurement by the arm's SBP measurement (Stanford Medicine 25, n.d.).
ABI Procedure: Noninvasive
Testing requires a blood pressure cuff and handheld Doppler. It takes about 10 minutes to complete.
Before starting the ABI test make sure
Patient is comfortable in a supine position and allow them to rest for 10 minutes. Socks and shoes must be removed for the test.
ABI procedure: Measuring the Brachial Pressure
Systolic brachial pressures will be taken on both arms unless contraindicated (e.g., dialysis shunt). To obtain the brachial SBP:
- Place the blood pressure cuff on the arm, keeping the limb at heart level.
- Apply ultrasound gel over the brachial pulse in the antecubital fossa.
- Place the Doppler transducer on the gel, adjusting to maximize signal intensity.
- Inflate the cuff to about 20 mmHg above the expected systolic blood pressure.
- Confirm that the Doppler signal disappears.
- Slowly deflate the cuff at about 1 mmHg per second.
- The brachial systolic pressure is noted when the Doppler signal reappears.
- Record the brachial systolic pressure.
ABI procedure: Measuring the Ankle Pressure
The ankle SBP will be obtained from both the dorsalis pedis (DP) and posterior tibialis (PT) on both limbs.
- Place the blood pressure cuff just above the malleoli.
- Apply ultrasound gel over the dorsalis pedis (DP) and posterior tibial (PT) artery areas on the foot.
- Locate the DP artery Doppler signal.
- Inflate the cuff at least 20 mmHg above the point the Doppler signal disappears.
- Slowly deflate the cuff until the signal reappears, then record the pressure.
- Next, find the PT Doppler signal posterior to the medial malleolus.
- Follow the same inflation and deflation technique as for the DP artery.
- Repeat the DP and PT measurements on the opposite leg.
Calculating ABI TRUE / FALSO
To calculate the ABI, the higher pressure of the two ankle arteries is divided by the highest arm (brachial) pressure.
TRUE
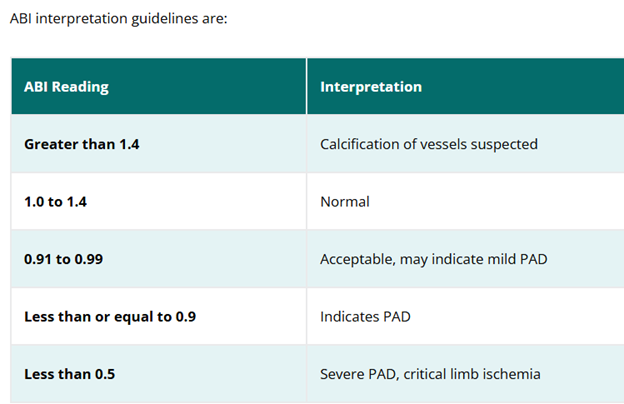
ABI interpretation guidelines are:
- Greater than 1.4
- 1.0 to 1.
- 0.91 to 0.99
- Less than or equal to 0.9
- Less than 0.5
- Calcification of vessels suspected
- Normal
- Acceptable, may indicate mild PAD
- Indicates PAD
- Severe PAD, critical limb ischemia
ABI interpretation reading of >1.4 is
Calcification of vessels suspected
ABI interpretation reading of 0.91 to 0.99
Acceptable, may indicate mild PAD
ABI interpretation reading of <0.5
Severe PAD, critical limb ischemia
An ABI of less than 0.5 indicates severe arterial disease, meaning....
there may not be sufficient blood flow to heal a chronic wound. This can be limb-threatening, and these patients will need prompt referral to a vascular specialist for further workup and potential interventions to improve blood flow necessary for healing.
Remember an ABI of LESS THAN 0.5 indicates ____ ___ ___, meaning ________
severe arterial disease ; there may not be sufficient blood flow to heal a chronic wound. This can be limb-threatening,
Toe-Brachial Pressure Index
It is calculated the same way as an ABI, with the SBP of the great toe (hallux) divided by the highest brachial SBP
Toe-Brachial Pressure Index
A toe-brachial pressure index (TBPI) is useful to determine the presence or lack of perfusion in the toes.
A result greater than 0.7 is normal, while less than 0.64 indicates PAD for what pressure index?
Toe-Brachial Pressure Index (TBI)
Dopper Waveform Analysis
Uses a Doppler probe to assess the shape and quality of arterial waveforms. It helps evaluate blood flow and detect defects in arterial supply
What test is this?
It is often the first step in assessing arterial blood flow in patients with suspected PAD. It helps discern between normal, monophasic, biphasic, and triphasic waveforms, which indicate varying degrees of arterial health.
Doppler Waveform Analysis
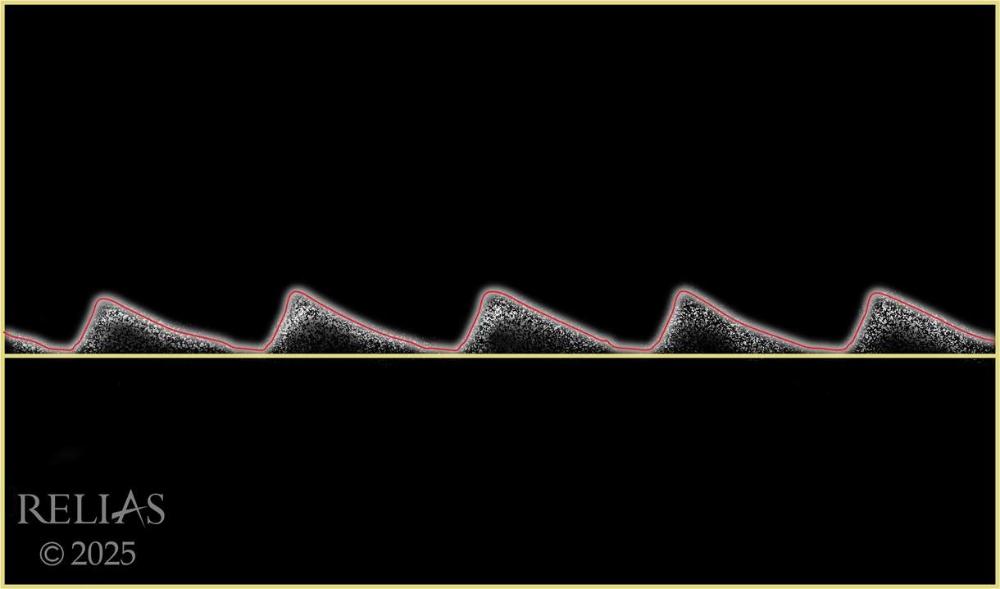
Normal arterial flow is triphasic and has three distinct phases; what are they?
- Forward flow
- Flow reversal
- Second forward component
___ or _____ waveforms suggest reduced vascular resistance or flow restriction.
Biphasic ; monophasic
Biphasic waveforms have two phases, what are they?
- Forward flow
- Reverse flow
Monophasic waveforms have a single phase, typically ___ ____ ____.
continuous forward flow
A transition from triphasic to monophasic helps ___ the level of the ____
localize ; disease
Name the waveform
Monophasic
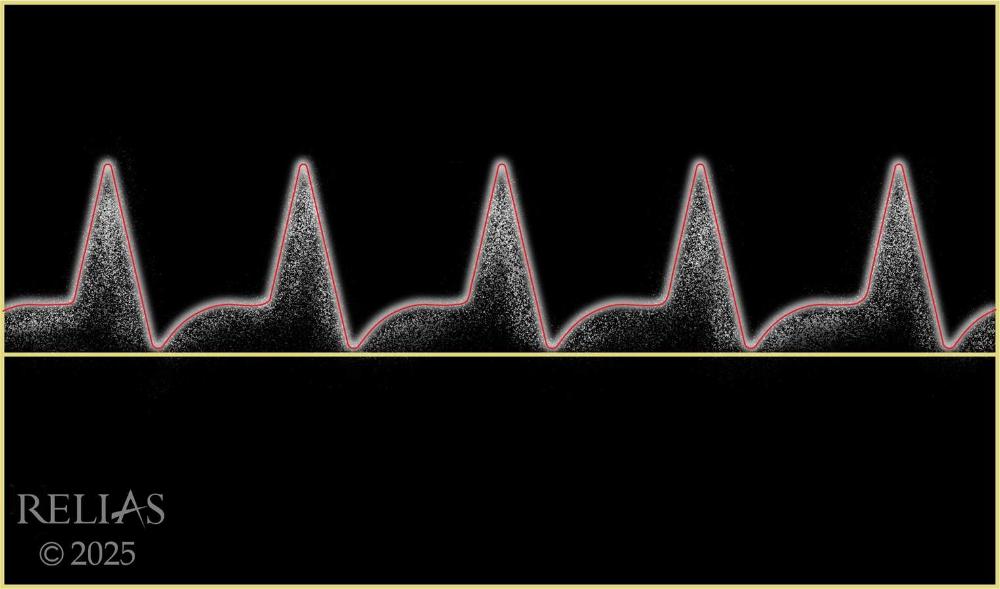
Name the waveform
Biphasic
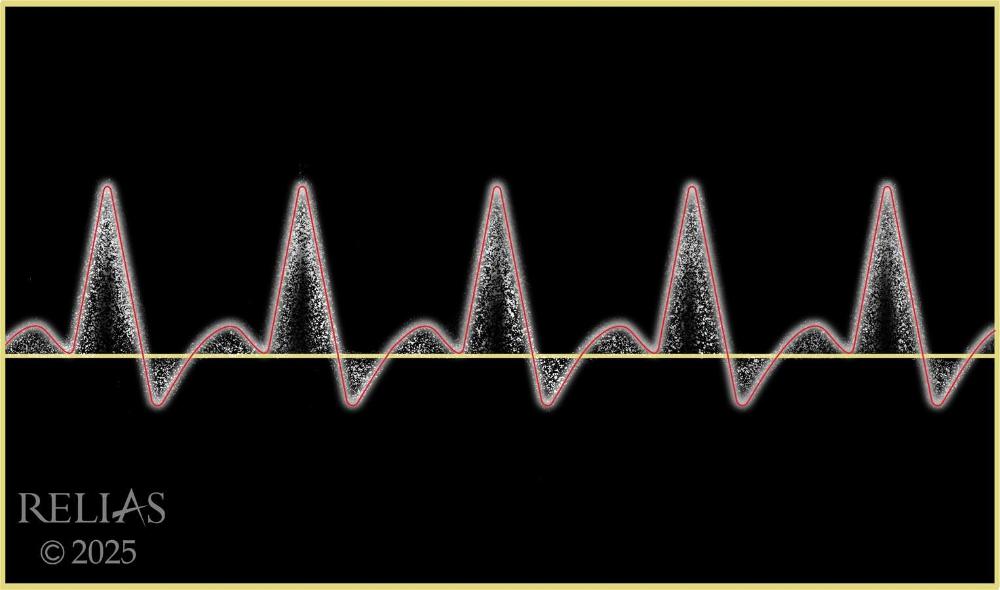
Name the waveform
Triphasic
Pulse Volume Recording
The pulse volume recording (PVR) graphs limb volume changes with blood flow.
Pulse Volume Recording process
Special cuffs that incorporate pneumoplethysmography (detects volume changes in the arteries) capability are placed around the limb at multiple points along the limb and inflated to standard pressure
Pulse Volume Recording (PVR) uses
PVR is useful for locating areas of blockage in limb segments, especially in patients with non-compressible vessels.
PVR
A ____ ___ shows a quick rise and sharp peak, with a noticeable dip (dicrotic notch) followed by a rounded curve.
normal PVR
PVR
An abnormal PVR, which might have ____ ___ or miss this dip, can signal blocked or reduced blood flow.
flattened peaks
PVR
Sudden changes in the ___ or ___ of the wave between different areas suggest a blockage in the blood vessels
size or shape
Using BP cuffs and a Doppler device, the segmental limb pressure test measures BP at multiple points along the limb. The purpose is
It helps identify a general location of arterial blockages or stenoses but is not exact.
Segmental Limb Pressure: process
This test is performed on both legs to compare the arterial flow from the left and right limbs. A difference of 30 mm Hg at the same level between the left and right legs could suggest an occlusion or blockage in blood flow
Segmental Limb Pressure
Additionally, if there is a ______ ___ __ from one segment to the other on the same limb, it signals occlusive disease and can help pinpoint its general location (McNichol et al., 2021; Sibley et al., 2017). For example, a decrease in pressure at the thigh level may indicate an aortoiliac or femoral artery issue, whereas pressure drops closer to the ankle suggest distal disease
significant pressure drop (e.g., greater than 20 mmHg)
Venous Duplex
Ultrasound checks blood flow in the veins, looking for signs of reflux lasting more than 0.5 seconds after muscle contraction or applying pressure (Baranoski & Ayello, 2020).
Color Duplex Ultrasound
This advanced ultrasound technique combines traditional ultrasound imaging with Doppler flow studies. It provides detailed images of blood vessels and flow properties in color. It is ideal for a comprehensive evaluation of both arterial and venous systems. It helps detect precise locations of stenosis, occlusions, aneurysms in arteries.
What test helps detect precise locations of stenosis, occlusions, aneurysms in arteries
Color Duplex Ultrasound
What two invasive tests are used to diagnose vessel disease and sometimes involve a procedure (e.g., balloon angioplasty) to fix diseased vessels or serve as an initial step before a complex operation to repair blood vessels
Angiography and Arteriography.
Angiography and Arteriography.
What Invasive LE Diagnositc tests are usually completed with a vascular specialist in an interventional radiology suite.
This uses contrast dye to assess blood flow and check for blockages or narrowing in the arteries. It can precisely identify and measure disease in the arteries, allowing for a clear diagnosis.
Contrast Angiogram (Arteriogram)
The ____ must be checked before the application of compression therapy. The ___ is a noninvasive test that assesses arterial disease by measuring the ratio of BP in the ankle to that in the arm to assess for arterial blockages
ABI / ABI
An ABI over 1.4 suggests ___ ___, common with diabetes, making the ABI unreliable. The next step is referring to a vascular specialist for additional tests.
calcification of vessels
* No compression, it's not recommend until we know there is adequate blood flow present in the limb.
The ____ ___ is a network of veins that fight gravity to return deoxygenated blood to the heart and lungs for reoxygenation.
venous system
There are three types of lower extremity veins, including:
1. Superficial
2. Deep
3. Perforator
Superficial Veins:
- Found in subcutaneous tissue
Deep Veins
- Found in the muscular fascia
- Accompany major arteries
Perforator Vein
- Connect superficial to deep veins
- Equipped with one-way bicuspid valves to prevent blood reflux
Steps of normal venous flow include:
- Blood drains from skin and subcutaneous tissue to superficial veins under low pressure
- This blood flows through perforator vein to the deep veins.
- Deep veins push blood
upward using muscle contraction under high pressure
- The deep vein system is responsible for pushing blood upwards using surrounding muscle contraction to the inferior vena cava of the heart and central veins for reoxygenation.
___ ___ __ originates from the dysfunction of the venous valves. Valve dysfunction occurs when the one-way valves become damaged or weakened. This valve failure leads to blood pooling in the lower extremities, which increases venous pressure, a condition known as venous hypertension.
Chronic venous insufficiency (CVI)
Persistent venous hypertension and pooling lead to various skin changes, including _____ and _____, as well as the ___ ___ ___ __, predisposing the skin to ulcerations
hyperpigmentation ; thickening ; breakdown of tissue integrity
What conditions are the below factors a risk for?
- Advanced age
- Obesity
- History of deep vein thrombosis (DVT)
- Thrombophilic (hypercoagulability) conditions
- Congestive heart failure
- Immobility or sedentary lifestyle
- Impaired calf pump
- Family history of PVD
Risk factors for CVI and VLUs include

What condition is this image of?
Venous Dermatitis: Also known as “stasis dermatitis,” this dermatitis is a chronic, non-contagious skin inflammation in patients with CVI. It is often confused with cellulitis but is uniquely different, as it is not infectious.
Management of Venous Dermatitis
Prompt detection and early intervention
- Routine cleansing with mild non soap cleanser with no artificial colors or fragrances to remove scales, crusts, bacteria
- Apply emollients to damp peri wound skin to prevent excessive drying of the skin
- Avoid products with known sensitizing agents such as Lanolin as VLU patients have higher risk for allergic contact dermatitis
- If heavy wound exudate, provide high-level peri wound protectio
If the patient has dermatitis/eczema, evidenced by increased pruritus, erythema and scaling
- 2-week use of a mild potency topical corticosteroid ointment may be used (i.e., Triamcinolone ointment 0.1%)
- After 2 weeks, switch to an emollient
- If there is no improvement, may refer to dermatology
Cellulitis
- Cause: Bacterial infection, most commonly Staphylococcus or Streptococcus, entering through a break in the skin.
- Symptoms May Include: Local heat and tenderness, increasing erythema, red streaks up the limb (lymphangitis), rapid increase in wound size, and fever
- Diagnostic Testing: ESR, CBC, WBC are usually high
- Appearance: Skin may feel tight, glossy, and stretched.
- Location: Can occur anywhere, but common in the lower legs. Presents unilaterally
- Treatment: Typically
involves oral or IV antibiotics.
- Wound cultures should be performed when there are clinical signs and symptoms of significant infection to guide antibiotic therapy
The following traits it exhibits are consistent with VLUs: WOUND EDGES
have irregular and poorly defined edges.
The following traits it exhibits are consistent with VLUs: DEPTH
These ulcers are shallow and rarely invade deep into the muscle or bone.
The following traits it exhibits are consistent with VLUs: WOUND BED
This can appear as ruddy, red granular tissue and/or yellow slough.
The following traits it exhibits are consistent with VLUs: EXUDATE
often produce a large amount of exudate. This exudate can be clear or yellowish and may become purulent if infected. Exudate needs to be managed to prevent maceration of the surrounding skin.
The following traits it exhibits are consistent with VLUs: PERIWOUND
Skin may appear crusty, scaling, or wet and weepy. There may also be hemosiderin staining, edema, scarring, and fibrosis.
Associated signs and symptoms that may indicate a wound is a VLU include: Wound Pain
The pain is variable and often described as dull, aching, itchy, sharp, or throbbing in the affected leg. It worsens with prolonged standing or walking and is often relieved by elevating the leg.
Associated signs and symptoms that may indicate a wound is a VLU include: Edema
Lower leg swelling is a hallmark of venous insufficiency. The edema is often pitting and can be mild to severe.
Associated signs and symptoms that may indicate a wound is a VLU include: Warmth
The skin around the ulcer may feel warm to the touch due to inflammation and increased blood flow. However, warmth without infection is often found in venous leg ulcers.
A common hallmark of venous insufficiency is the _____ ______, known as ____ _____.
discoloration of the limb ;
TRUE / FALSE
VLU have Irregular wound margins
TRUE
TRUE / FALSE
VLU - classic location of gaiter area
TRUE
TRUE / FALSE
VLU appearance of Round, punched-out appearance
FALSE
* Round punched out appearance is Arterial Ulcer
TRUE / FALSE
VLU has - Wound base with red, granular, and/or slough
TRUE
TRUE / FALSE
VLU'S are often found on toes
FALSE
* DFU - Diabetic foot ulcer
TRUE / FALSE
VLU has a pale wound base with necrosis
FALSE
TRUE / FALSE
Warm feet, pulses present - describe VLU
TRUE
TRUE / FALSE
Cool/Cold feet, diminished to absent pulses also described VLUs
FALSE
TRUE / FALSE
VLUs commonly have moderate to heavy exudate
TRUE
TRUE / FALSE
VLU has minimal to no exudate
FALSE
What do the below stages are represent?
- C0: No visible or palpable signs of venous disease
- C1: Telangiectasias or reticular veins
- C2: Varicose
veins
- C2r: Recurrent varicose veins
Clinical Classification
HCPs may only use this section to document the severity of venous leg ulcers. The clinical classification component categorizes venous disease based on observable clinical signs, ranging from no visible signs to the most severe manifestations.
C0:
No visible or palpable signs of venous disease
C1:
Telangiectasias or reticular veins
C2:
Varicose veins
- C2r: Recurrent varicose veins
C2r:
Recurrent varicose veins
Note that __ to __ indicates chronic venous insufficiency (McNichol et al., 2021).
C4 to C6
Etiological Classification : Purpose
A component that identifies the underlying cause of the venous disorder (Lurie et al., 2020):
Etiological Classifications:
- Ep (Primary): Primary venous disease without secondary or congenital factors
- Es (Secondary): Venous disease secondary
to intravenous or extravenous factors (use subcategories to
identify)
- Esi (Secondary--Intravenous): Intravenous damage from conditions like DVT, arteriovenous fistulas, or vein tumors
- Ese (Secondary—Extravenous): Symptoms are present without direct vein damage, caused by problems with blood flow such as central venous hypertension (from obesity, heart failure, or pelvic congestion), pressure from outside the vein (like tumors or fibrosis), or poor muscle pump function due to conditions like paralysis, arthritis, or long-term immobility.
- Ec (Congenital): Congenital conditions like missing veins, venous malformations (such as Klippel-Trenaunay syndrome), or arteriovenous malformations that cause venous disease symptoms. These may be present at birth or appear later in life.
- En (No cause identified): No clear venous cause can be found, but has signs and symptoms of venous disease, considered a diagnosis of exclusion
- Ep
(Primary): Primary venous disease without secondary or congenital factors
Es (Secondary):
Venous disease secondary to intravenous or extravenous factors (use subcategories to identify).
- Esi (Secondary--Intravenous): Intravenous damage from conditions like DVT, arteriovenous fistulas, or vein tumors
- Ese (Secondary—Extravenous): Symptoms are present without direct vein damage, caused by problems with blood flow such as central venous hypertension (from obesity, heart failure, or pelvic congestion), pressure from outside the vein (like tumors or fibrosis), or poor muscle pump function due to conditions like paralysis, arthritis, or long-term immobility.
- Esi
(Secondary--Intravenous): Intravenous damage from conditions like DVT, arteriovenous fistulas, or vein tumors
-
- Ese
(Secondary—Extravenous): Symptoms are present without direct vein damage, caused by problems with blood flow such as central venous hypertension (from obesity, heart failure, or pelvic congestion), pressure from outside the vein (like tumors or fibrosis), or poor muscle pump function due to conditions like paralysis, arthritis, or long-term immobility.
- Ec (Congenital):
Congenital conditions like missing veins, venous malformations (such as Klippel-Trenaunay syndrome), or arteriovenous malformations that cause venous disease symptoms. These may be present at birth or appear later in life.
- En
(No cause identified): No clear venous cause can be found, but has signs and symptoms of venous disease, considered a diagnosis of exclusion
Anatomical Classification
This component specifies the location of the venous disorder within the venous system (Lurie et al., 2020):
- As (superficial veins): Involves superficial veins, use subcategories to identify:
- Tel: Telangiectasia
- Ret: Reticular veins
- GVS: Great saphenous vein above knee
- GSVb: Great saphenous vein below knee
- SSV: Small saphenous vein
- AASV: Anterior accessory saphenous vein
- NSV: Nonsaphenous vein
- Ad (deep veins): Involves deep veins, use subcategories to identify:
- IVC: Inferior vena cava
- CIV: Common iliac vein
- IIV: Internal iliac vein
- EIV: External iliac vein
- PELV: Pelvic veins
- CFV: Common femoral vein
- DFV: Deep femoral vein
- FV: Femoral vein
- POPV: Popliteal vein
- TIBV: Tibial vein
- PRV: Peroneal vein
- ATV: Anterior tibial vein
- PTV: Posterior tibial vein
- MUSV: Muscular veins
- GAV: Gastrocnemius vein
- SOL: Soleal vein
- Tel:
Telangiectasia
- Ret:
Reticular veins
- NSV:
Nonsaphenous vein
- AASV:
Anterior accessory saphenous vein
- SSV:
Small saphenous vein
- GSVb:
Great saphenous vein below knee
- GVS:
Great saphenous vein above knee
Ad
(deep veins): Involves deep veins, use subcategories to identify
- IVC:
Inferior vena cava
- CIV:
Common iliac vein
- IIV:
Internal iliac vein
- EIV:
External iliac vein
- PELV:
Pelvic veins
- CFV:
Common femoral vein
- DFV:
Deep femoral vein
- FV:
Femoral vein
- POPV:
Popliteal vein
- TIBV:
Tibial vein
- PRV:
Peroneal vein
- ATV:
Anterior tibial vein
- PTV:
Posterior tibial vein
- MUSV:
Muscular veins
- GAV:
Gastrocnemius vein
- SOL:
Soleal vein
- Ap (perforator veins): Involves perforator veins that connect the superficial veins to the deep veins, use subcategories:
- TPV: Thigh perforator vein
- CPV: Calf perforator vein
- An
(no identifiable venous location): When no specific vein can be found
Pathophysiologic Classification
This describes the underlying pathophysiological mechanisms causing the venous disorder:
- PR: Reflux of the venous valves, leading to backward flow of blood
- PO: Obstruction of venous flow due to thrombosis or other blockages
- PR,O: Combination of reflux and obstruction
- PN: No identifiable pathophysiology
- PR:
Reflux of the venous valves, leading to backward flow of blood
- PO:
Obstruction of venous flow due to thrombosis or other blockages
- PR,O:
Combination of reflux and obstruction
- PN:
No identifiable pathophysiology
Which characteristic is consistent with a venous leg ulcer?
Round, punched-out wound borders
Deep wound with irregular edges
Found in the gaiter area
Pallor at a 15° angle
Found in the gaiter area
*VLUs are usually shallow with irregular wound edges classically found in the gaiter area. Arterial ulcers present with round, punched-out borders, and pallor at a 15° angle are indicative of limb ischemia, not venous ulcerations.
- ___________ cause blood pooling, venous hypertension, and chronic venous insufficiency. It is difficult to heal wounds under these circumstances.
Incompetent valves in the veins
- VLUs have____ margins, shallow depth, and moderate to heavy exudate. They are commonly found on the medial lower extremity between the patella and malleolus (gaiter area).
irregular
True / False
Advanced age, obesity, pregnancy, and sedentary lifestyle increase the risk of venous leg ulcers.
TRUE