Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
blood vessels
front 1 blood vessels | back 1 the delivery system of dynamic structures that begins and ends at the heart |
front 2 ateries | back 2 carry blood away from the heart - the blood is oxygenated except for pulmonary circulation and umbilical vessels of a fetus |
front 3 capillaries | back 3 contact tissue cells and directly serve cellular needs - endothelium with sparse lamina |
front 4 veins | back 4 carry blood towards the heart |
front 5 venous system | back 5 heart - large veins (capacitance vessels) - small veins (capacitance vessels) - postcapillary venule - thoroughfare channel - capillaries |
front 6 arterial system | back 6 - elastic arteries (conducting vessles) - muscular arteries (distributing vessels)- |
front 7 layers of the blood vessel wall are in order from the inside out | back 7 lumen
|
front 8 lumen | back 8 central blood containing space, which is surrounded by three distinct layers or tunics. |
front 9 tunica intima | back 9 the innermost tunic - it is in intimate contact with the blood in the lumen
|
front 10 tunica media | back 10 smooth muscle and sheets of elastin, sympathetic vasometer nerve fibers control vasoconstriction and vasodialation of vessels |
front 11 vasoconsctriction | back 11 reduction in lumen diameter as the smooth muscle contracts |
front 12 vasodialation | back 12 increase in lumen diameter as the snooth muscle relaxes |
front 13 tunica externa (also known as tunica adventitia) | back 13 collagen fibers protect and reinforce, large vessels contain vasa vasorum to nourish the external layer |
front 14 vasa vasorum | back 14 a system of tiny blood vessels theat nourish the more external tissues of the blood vessel wall -its own blood supply |
front 15 Arteries: | back 15 •Arteries have three layers: a smooth inner layer, a muscular layer, and a thin outer layer.
|
front 16 Veins: | back 16 •Veins, like arteries, have three layers: a smooth inner layer, a muscular layer, and a thin outer layer.
|
front 17 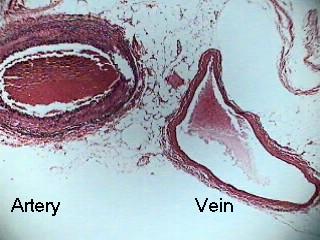 | back 17 atery and vein |
front 18 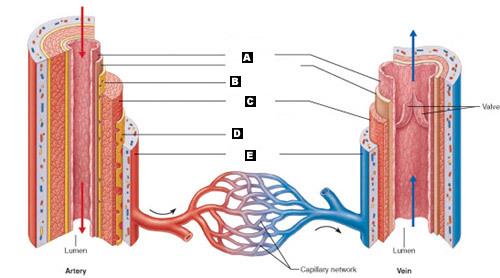 label | back 18 A. Tunica intima
|
front 19 elastic ateries | back 19 large thick walled arteries with elastin in all three tunics, near the heart the aorta and its major branches, large lumen offers low resistance sometimes referred to as conducting arteries, act as pressure resevoirs - expand and recoil as blood is ejected from the heart
|
front 20 lumen | back 20 central blood containing space |
front 21 capillaries | back 21 endothelium with sparse basal lamina |
front 22 tunica intima | back 22 simple squamous endothelium, lines the lumen of all vessels in vessels larger than 1 mm a subendothelial connective tissue basement membrane is present |
front 23 tunica media | back 23 smooth muscle and sheets of elastin, sympathetic vasomotor nerve fibers control vasoconstriction and vasodialation of vessels |
front 24 tunica externa (tunica adventitia) | back 24 collagen fibers protect and reinforce, larger vessels contain vasa vasorum to nourish the external layer |
front 25 elastic conducting ateries | back 25 large thick walled arteries with elastin in all three tunics, the aorta and its major branches, large lumen offers low resistance, acts as pressure reservoirs - expand and recoil as blood is ejected from the heart |
front 26 lumen | back 26 internak hollow space |
front 27 muscular(distributing) arteries and arterioles | back 27 distal to elastic arteries, deliver blood to body organs, have a thick tunica media with more smotth muscle, active in vasocontriction, controls blood flow through tissues |
front 28 arterioles | back 28 smallest arteries, lead to capillary beds, control flow into capillary beds via vasodialation and vasoconstriction |
front 29 vasodialation | back 29 relaxation of the smooth muscles of the blood vessels, producing dialation |
front 30 vasoconstriction | back 30 narrowing of blood vessels |
front 31 capillaries | back 31 microscopic blood vessels, walls of thin tunica intima, one cell thick, pericytes help stablize their walls and control permeability, size allows only a single RBC to pass at a time, inall tissues except for cartilage, epithelia, cornea and lens of eye. |
front 32 capillaries - function | back 32 exchange gases, nutrients, wastes, hormones, etc. |
front 33 the three structural types of capillaries | back 33 continuous capillaries
|
front 34 continuous capillaries are abundant where | back 34 in the skin and muscles
|
front 35 continuous capillaries of the brain - junctions | back 35 tight junctions are complete, forming the *blood brain barrier* |
front 36 fenestrated capillaries | back 36 some endothelial cells contain pores (fenestrations) more permeable then continuous capillaries - function in absorption or filtrate formation (small intestines, endocrine glands, and kidneys) |
front 37 sinusoidal capillaries | back 37 fewer tight junctions, larger intercellular clefts, large lumen, usually fenestrated, allow large molecules and blood cells to pass between the blood abd surrounding tissues |
front 38 where are sinusoidal capillaries found | back 38 in the liver, bone marrow and spleen |
front 39 where do the clefts sit | back 39 in between the cells |
front 40 capillary beds | back 40 are interwoven networks of capillaries form the microcirculation between arterioles and venules |
front 41 capillary beds consist of two types of vessels what are they | back 41 1. vascular shunt (metarteroile - thoroughfare channel) directly connects the terminal arteriole and a postcapillary venule
|
front 42 precapillary sphincters do what | back 42 regulate blood flow into true capillaries; regulated by local chemical conditions and vasomotor nerves |
front 43 when are venules formed | back 43 when capillary beds unite, they are very porous and allow fluids and WBC's into tissues - post capillary venules consist of endothelium and a few pericytes, larger venules have on or two layers of smooth muscle cells |
front 44 which are bigger veins or capillaries | back 44 veins |
front 45 When are veins formed | back 45 when venules converge, have thinner walls, larger lumens compared with corresponding arteries, blood pressure is lower than in arteries, thin tunica media and a thick externa consisting of collagen fibers and elastic networks - called capacitance vessels (blood reservoirs) contain up to 65% of the blood supply, are adaptations that ensure return of blood to the heart |
front 46 pericyte | back 46 adventitial cell or mural cell, is a connective tissue cell that occurs about small blood vessels.[ |
front 47 what purpose do large diameter lumens offer in the veins | back 47 they offer little resistance |
front 48 what purpose do valves offer in the veins | back 48 prevent the backflow of blood - most abundant in veins of the limbs |
front 49 what are venous sinuses | back 49 they are flattened veins with extremely thin walls (coronary sinus of the heart and dural sinuses of the brain) |
front 50 vascular anastomoses are | back 50 interconnections of blood vessels - arterial anastomoses provide alternate pathways (collateral channels) to a given body region - they are common at joints, in abdominal organs, brain and heart
|
front 51 blood flow - | back 51 volume of blood flowing through a vessel, an organ, or the entire circulation in a given period
|
front 52 blood pressure | back 52 force per unit area exerted on the wall of a blood vessel by the blood, expressed in mm Hg
|
front 53 resistance (peripheral resistance) | back 53 opposition of flow
|
front 54 three important sources of resistance are | back 54 blood viscosity - thickness of the blood
|
front 55 factors that remain relatively constant in regards to resistance are | back 55 blood viscosity - the stickiness of the blood due to formed elements and plasma proteins
|
front 56 frequent changes that alter peripheral resistance are | back 56 blood vessel diameter - it is always changing
|
front 57 blood flow (F) is directly proportional to what | back 57 the blood (hydrostatic) pressure gradient (delta P) if the pressure gradient increases then the blood flow speeds up |
front 58 blood flow is inversely proportional to what | back 58 peripheral resistance (R)
|
front 59 flow = | back 59 pressure gradient divided by peripheral resistance |
front 60 peripheral resitance is more important in influencing local blood flow because of what | back 60 it is easily changed by altering blood vessel diameter |
front 61 what generates blood flow | back 61 the pumping action of the heart |
front 62 pressure results when what | back 62 when flow is opposed by resistance |
front 63 systemic pressure is | back 63 highest in the aorta
|
front 64 the steepest drop occurs where | back 64 in the arterioles |
front 65 arterial blood pressure reflects what | back 65 two factors of the arteries close to the heart - elasticity (compliance or distensibility) volume of blood forced into them at any time
|
front 66 pulse near the heart is what | back 66 pulsatle |
front 67 systolic pressure | back 67 pressure exerted during ventricular contraction |
front 68 diastolic pressure | back 68 lowest level of arterial pressure |
front 69 pulse pressure | back 69 difference between systolic and diastolic pressure |
front 70 mean arterial pressure | back 70 pressure that propels the blood to the tissues |
front 71 MAP = | back 71 diastolic pressure = 1/3 pilse pressure |
front 72 when do pulse pressure and MAP both decline | back 72 with increasing distance from the heart |
front 73 what is the range of capillary blood pressure | back 73 ranges from 15 to 35 mm Hg, low capillary pressure is desirable - high blood pressure would rupture fragile, thin- walled capillaries, most are very permemable, so low pressure forces filtrate into interstitial spaces |
front 74 when pressure is low how does the blood move | back 74 more slowly |
front 75 does venous pressure change during the cardiac cycle | back 75 very little
|
front 76 one of the factors aiding venous return is the respiratory pump - explain | back 76 pressure changes created during breathing move blood toward the heart by squeezing abdominal veins as thoracic veins expand |
front 77 one of the factors aiding venous return is the muscular pump - explain | back 77 contraction of skeletal muscles "milk" blood toward the heart and valves prevent backflow |
front 78 one of the factors aiding venous return is the vasoconstriction - explain | back 78 vasoconstiction of veins under sympathetic control - because of the smooth muscle |
front 79 maintaining blood pressure requires what | back 79 cooperation of the heart blood vessels and kidneys
|
front 80 what are the main factors influencing blood pressure | back 80 cardiac output (CO)
|
front 81 Blood pressure = | back 81 = CO x PR (and CO depends on blood volume)
|
front 82 how is the cardiac output determined | back 82 by venous return and neural and hormonal controls |
front 83 resting heartrate is maintinaed by what | back 83 the cardioinhibitory center via the parasympathetic vagus nerve |
front 84 stroke volume is controled by what | back 84 venous return (EDV) |
front 85 during stress the heart cardioaccelertory center increases heart rate and stroke volum via what | back 85 sympathetic stimulation |
front 86 if the ESV decreases what happens to MAP | back 86 it increases |
front 87 what are the short term controls of blood pressure | back 87 neural and hormonal controls
|
front 88 what are the long term controls of blood pressure | back 88 long term renal regulation
|
front 89 neural controls of peripheral resistance do what | back 89 maintain MAP by altering blood vessel diameter
|
front 90 neural controls operate via reflex arcs tha tinvolve what | back 90 baroreceptors
|
front 91 the vasomotor center is what | back 91 a cluster of sympathetic neurons in the medula that oversee changes in blood vessel diameter
|
front 92 the vasomotor center does what | back 92 maintains vasomotor tone (moderate constriction of the arterioles)
|
front 93 where are barorecptors located | back 93 in carotid sinuses, aortic arch, walls of large arteries of the neck and thorax |
front 94 what happens to the baroreceptors when blood pressure increases | back 94 increased blood pressure stimulates the baroreceptors to increase input to the vasomotor center
|
front 95 what protects the blood supply to the brain | back 95 Baroreceptors taking part in the carotid sinus reflex protect the blood supply to the brain |
front 96 what helps maintain adequate blood pressure in the systemic circuit | back 96 Baroreceptors taking part in the aortic reflex help maintain adequate blood pressure in the systemic circuit |
front 97 what happens if the blood pressure rises above a normal range | back 97 1. blood pressure (arterial blood pressure rises above normal range)
|
front 98 what happens if the blood pressure drops below a normal range | back 98 1. blood pressure decreases (arterial blood pressure falls below a normal range)
|
front 99 Short-Term Mechanisms: Chemoreceptor-Initiated Reflexes where are the Chemoreceptors located | back 99 in the Carotid sinus, aortic arch, large arteries of the neck
|
front 100 what do the chemoreceptor sin the carotid sinus respond to | back 100 to rise in CO2, drop in pH or O2
|
front 101 where are the relexes that regulate blood pressure integrated from | back 101 the medulla
|
front 102 which hormone causes blood pressure to decline | back 102 ANP atrial natriuretic peptide
|
front 103 influence of selected hormones on variables affecting blood pressure: epinepherine and norepinephrine | back 103 cause generalized vasoconstriction and increase cardiac output |
front 104 influence of selected hormones on variables affecting blood pressure: angiotensin II | back 104 generated by kidney release of renin causes vasoconstriction |
front 105 influence of selected hormones on variables affecting blood pressure: ADH (antidiurectic hormone - vasopressin) | back 105 causes intense vasoconstriction in cases of extremely low BP |
front 106 influence of selected hormones on variables affecting blood pressure: aldosterone | back 106 increase in blood volume, decrease in water loss - occurs in the kidneys |
front 107 influence of selected hormones on variables affecting blood pressure: cortisol | back 107 increase in blood volume, decrease in water loss - occurs in the kidneys |
front 108 kidneys act directly to regulate arterial blood pressure by doing what | back 108 direct renal mechanism
|
front 109 kidneys act indirectly to regulate arterial blood pressure by doing what | back 109 indirect renal (renin- angiotensin) mechanism
|
front 110 Angitensin II stimultes the release of what | back 110 ADH |
front 111 what are vital signs | back 111 pulse and blood pressure along with rsepiratory rate and body temperature |
front 112 pulse | back 112 pressure wave caused by the expansion and recoil of ateries - rarial pulse Taken at the wrist) routinely used |
front 113 how do you measure blood pressure | back 113 with a sphygmomanometer
|
front 114 what are some variations in blood pressure | back 114 blood pressure cuclye over a 24 hour period
|
front 115 hypotension | back 115 low blood pressure
|
front 116 orthostatic hypotension | back 116 temporary low blood pressure and dizziness when suddenly rising from a sitting or reclining position |
front 117 chronic hypotension | back 117 hint of poor nutrition and warning signs for addisons disease (hyposecretion of aldosterone) or hypothyroidism |
front 118 acute hypotension | back 118 important sign of circulatory shock |
front 119 hypertension | back 119 high blood pressure
|
front 120 Primary or essential hypertension | back 120 90% of hypertensive conditions (no underlying cause), Due to several risk factors including heredity, diet, obesity, age, stress, diabetes mellitus, and smoking |
front 121 Secondary hypertension | back 121 less common
|
front 122 how many pulse points are there and where are they | back 122 nine
|
front 123 blood flow tissue perfusion is involved in what | back 123 delivery of oxygen and nutrients to and removal of wastes from tissue cells
|
front 124 properties of the velocity of blood flow | back 124 changes as it travels through the systemic circulation
|
front 125 what does slow capillary flow allow for | back 125 allows for adequate time for exchange between blood and tissues |
front 126 autoregulation | back 126 automatic adjustment of blood flow to each tissue in proportion to its requirements at any given point in time |
front 127 how is autoregulation controlled | back 127 intrinsically by modifying the diameter of local arterioles feeding the capillaries i ti is independant of MAP , which is controlled as needed to maintain constant pressure |
front 128 what are the two types of autoregulation | back 128 1. metabolic
|
front 129 describe metabolic autoregulation | back 129 •Vasodilation of arterioles and relaxation of precapillary sphincters occur in response to
|
front 130 describe myogenic autoregulation | back 130 •Myogenic responses of vascular smooth muscle keep tissue perfusion constant despite most fluctuations in systemic pressure |
front 131 what is passive stretch | back 131 (increased intravascular pressure) promotes increased tone and vasoconstriction |
front 132 what is reduced stretch | back 132 promotes vasodilation and increases blood flow to the tissue |
front 133 Intrinsic mechanisms (autoregulation) | back 133 Distribute blood flow to individual organs and tissues as needed |
front 134 what are the Metabolic controls involved in Intrinsic mechanisms (autoregulation) | back 134 decrease amounts of: pH and oxygen
|
front 135 what are the Myogenic controls (muscular responses) involved in Intrinsic mechanisms (autoregulation) | back 135 Stretch |
front 136 Extrinsic mechanisms | back 136 Maintain mean arterial pressure (MAP) Redistribute blood during exercise and thermoregulation |
front 137 nerves involved in extrinsic control of anterior smooth muscle in the systemic circulation | back 137 sympathetic (constriction) |
front 138 hormones involved in extrinsic control of anterior smooth muscle in the systemic circulation | back 138 epinephrine and norepinephrine (alpha receptors - constrict) (beta receptors - dilate)
|
front 139 angiogenesis | back 139 occurs when short term autoregulation cannot meet tissue nutrient requirements
|
front 140 when does angiogenesis occur | back 140 common in the heart when a coronary vessel is occluded, or throughout the body in people in high aaltitude areas |
front 141 what happens to blood flow to the skeletal muscles during rest | back 141 at rest myogenic and general neural mechanisms predominate |
front 142 what happens with blood flow to muscles during activity | back 142 Blood flow increases in direct proportion to the metabolic activity (active or exercise hyperemia)
|
front 143 blood flow to the brain | back 143 Blood flow to the brain is constant, as neurons are intolerant of ischemia |
front 144 what are the metabolic controls involved in blood flow to the brain | back 144 Declines in pH, and increased carbon dioxide cause marked vasodilation |
front 145 what are the Myogenic controls involved in blood flow to the brain | back 145 Decreases in MAP cause cerebral vessels to dilate
|
front 146 syncope | back 146 fainting |
front 147 cerebral edema | back 147 an excess accumulation of water in the intracellular and/or extracellular spaces of the brain. |
front 148 blood flow to the skin does what (through the skin) | back 148 Blood flow through the skin
|
front 149 blood flow to the skin does what (below the skin surface) | back 149 Blood flow to venous plexuses below the skin surface
|
front 150 as temperature rises what occurs
| back 150 Hypothalamic signals reduce vasomotor stimulation of the skin vessels thus producing vasodilation
|
front 151 Bradykinin | back 151 Bradykinin is a peptide that causes blood vessels to dilate (enlarge), and therefore causes blood pressure to lower |
front 152 NO | back 152 nitric oxide |
front 153 as temperature decreases what occurs | back 153 As temperature decreases, blood is shunted to deeper, more vital organs |
front 154 blood flow to the lungs | back 154 Pulmonary circuit is unusual in that
|
front 155 blood flow to the heart - during ventricular systole | back 155 Coronary vessels are compressed
|
front 156 blood flow to the heart - during ventricular diastole | back 156 At rest, control is probably myogenic |
front 157 blood flow to the heart during the strenuous exercise | back 157 Coronary vessels dilate in response to local accumulation of vasodilators
|
front 158 blood flow through the capillaries vasomotion | back 158 slow and intermittent flow
|
front 159 capillary exchange of respiratory gases and nutrients | back 159 Diffusion of
|
front 160 what are the four possible pathways or routes of transport across the endothelial cell wall of a fenestrated capillary | back 160 1 Diffusion through membrane (lipid-soluble substances)
|
front 161 Fluid Movements: Bulk Flow | back 161 •Extremely important in determining relative fluid volumes in the blood and interstitial space
|
front 162 Net Filtration Pressure (NFP) | back 162 •NFP—comprises all the forces acting on a capillary bed
|
front 163 Circulatory Shock | back 163 Any condition in which Blood vessels are inadequately filled, Blood cannot circulate normally and Results in inadequate blood flow to meet tissue needs |
front 164 Hypovolemic shock: | back 164 results from large-scale blood loss |
front 165 Vascular shock: | back 165 results from extreme vasodilation and decreased peripheral resistance |
front 166 Cardiogenic shock | back 166 results when an inefficient heart cannot sustain adequate circulation |
front 167 artery side (arteriole) | back 167 fluid goes out - pushes out |
front 168 vein side (venule) | back 168 fluid goes in - pulls in |