Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM Module 20: Wound Care - Pain Management
front 1 Types of Pain Wound pain can be classified as nociceptive or neuropathic: Nociceptive | back 1 Activation of sensory neurons responding to harmful stimuli; it further breaks down into somatic and visceral.
|
front 2 Types of Pain Wound pain can be classified as nociceptive or neuropathic: Neuropathic (Chronic) | back 2 Dysfunction in the nervous system, often felt as burning or shooting (e.g., shingles pain) |
front 3 ____ pain can become chronic if it persists for longer than six months or continues to worsen over time (Physician Partners of America, 2022). | back 3 Nociceptive |
front 4 Physiological Effects of Pain _________ reduces blood flow to the wound site, limiting oxygen and nutrient delivery. | back 4 Pain-induced vasoconstriction |
front 5 Physiological Effects of Pain Persistent pain elevates cortisol and adrenaline, which can suppress the immune system and tissue repair (Woo, 2012). | back 5 Stress Hormone Release |
front 6 Physiological Effects of Pain Chronic pain sustains inflammation, leading to the prolonged presence of inflammatory cytokines and enzymes that can damage tissue and delay healing (Woo, 2012). | back 6 Inflammatory Response |
front 7 Psychological Effects of Pain Stress, Anxiety, and Depression | back 7
|
front 8 Psychological Effects of Pain Feelings of Helplessness and Frustration | back 8
|
front 9 Psychological Effects of Pain Depression | back 9
|
front 10 Pain Assessment: Standardized Tools: Scales- PQRST, Numeric Pain, Wong-bakers (faces), FLACC, Visual Analog Scale (VAS), Numeric Rating Scale (NRS), and McGill Pain Questionnaire | back 10 Use scales like the PQRST, Numeric Pain Scale (NPS), Wong-Baker FACES™ Scale, FLACC, Visual Analog Scale (VAS), Numeric Rating Scale (NRS), and McGill Pain Questionnaire for consistent pain measurement (Kirkcaldy et al., 2023). |
front 11 Pain Assessment: PQRST A standardized, easy-to-use mnemonic framework healthcare providers and patients use to systematically evaluate the nature, severity, and history of a patient's pain | back 11 P- provocation / Palliation: What triggers the pain, or makes it worse or better? Q- quality: How does the pain fell? (e.g., is it sharp, dull, burning, etc) R- region / radiation: Where exactly is the pain located, and does it spread or move to other parts of the body? S- severity: How bad is the pain? Pt. are normally asked to rate their pain from 0 to 10. T- timing: When did the pain start, how long does it last |
front 12 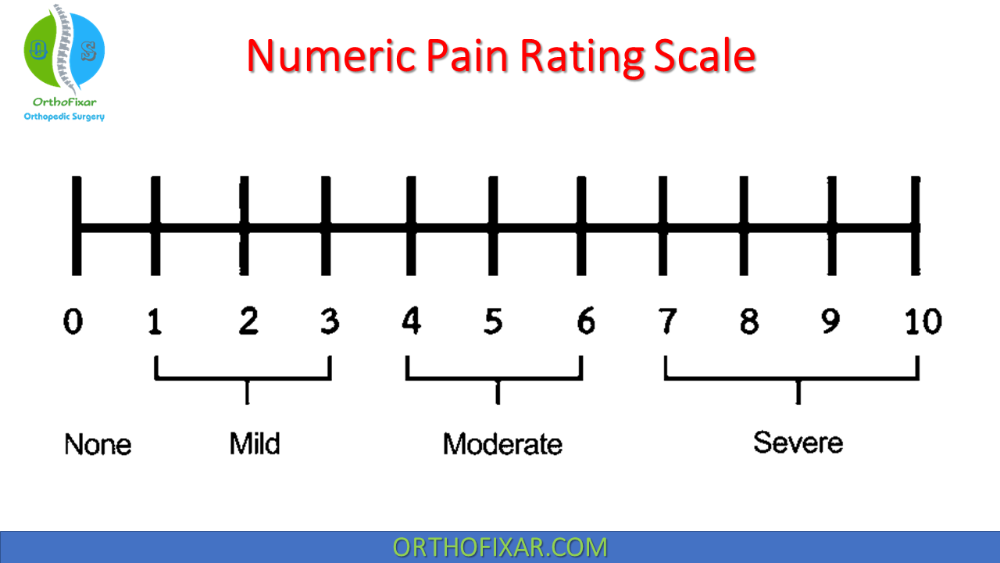 Pain Assessment: Numeric Pain Rating Scale | back 12 An 11-point scale (0–10) designed to measure pain intensity. Patients verbally state or circle a number that best reflects their pain level, with 0 meaning "no pain" and 10 meaning "the worst pain imaginable". |
front 13 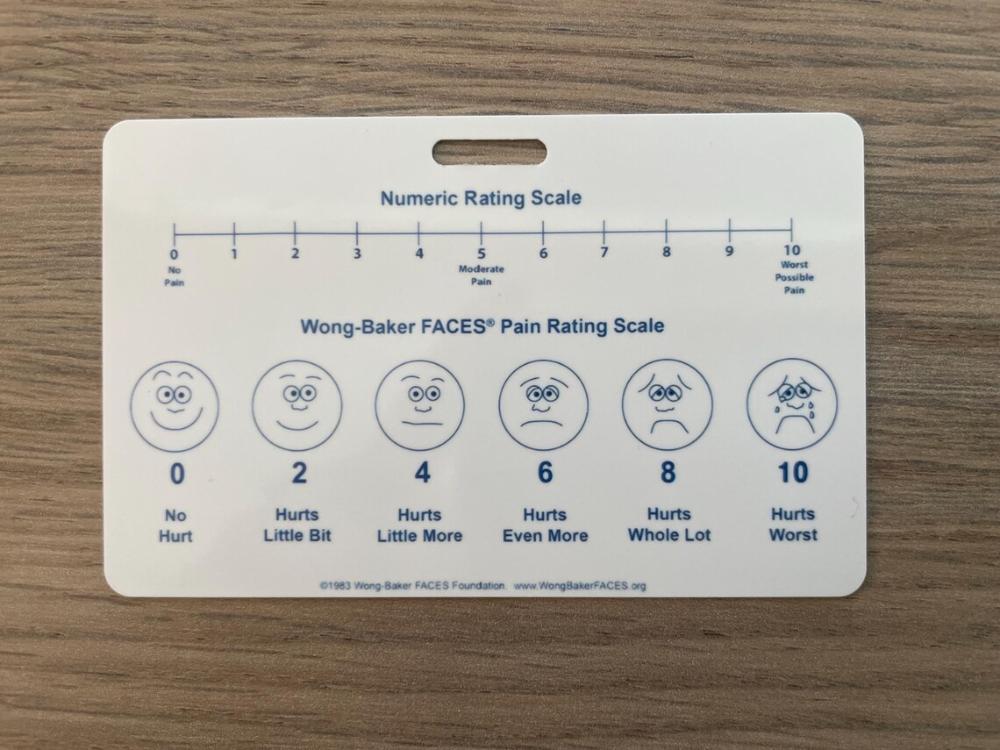 Pain Assessment: Wong baker faces pain rating scale | back 13 A visual self-assessment tool used by healthcare professionals to help individuals especially children ages 3 and older—communicate and rate their level of physical pain. Patients choose the face that best matches how much they hurt |
front 14 Pain Assessment: McGill Pain Questionnaire | back 14 A multidimensional self-report scale that helps clinicians measure the subjective quality, location, and intensity of a patient's pain. * It translates a patient's specific word choices into quantifiable data to track pain patterns and treatment effectiveness |
front 15 True / False There is no clinical difference between the Numeric Pain Scale and the Numeric Pain Rating Scale (NPRS) | back 15 True * They are two names for the exact same standardized 0-11 point assessment tool used by healthcare providers to measure pain severity. |
front 16 The Transdisciplinary Approach. Key team members include: | back 16
|
front 17 Which BEST describes how pain can impede wound healing? Pain increases the release of stress hormones, suppressing the immune system and reducing the body's ability to heal wounds. Pain reduces the release of stress hormones, enhancing the immune system and improving the body's ability to heal wounds. Pain increases inflammation and collagen production to improve wound healing. Pain enhances blood flow to the wound area through vasoconstriction to improve healing. | back 17 Pain increases the release of stress hormones, suppressing the immune system and reducing the body's ability to heal wounds. * Pain increases the release of stress hormones like cortisol and adrenaline, which can suppress the immune system, reducing the body's ability to heal wounds. Pain does not reduce the release of stress hormones; increased inflammation does not increase collagen production or enhance blood flow to improve healing. |
front 18 Non-Pharmaceutical; Offloading | back 18
|
front 19 A wound care clinician can ease patient anxiety through reflective listening. Attentively hearing the patient’s concerns, followed by repeating those concerns back to the patient, is a powerful tool that | back 19
|
front 20 Factors that impact pain during dressing changes include: | back 20
|
front 21 Often recommended as a non-irritating, isotonic option, saline gently cleanses without causing pain or tissue injury (Kirkcaldy et al., 2023). | back 21 Saline Solution |
front 22
| back 22
|
front 23
| back 23 Betaine/polyhexanide cleansers (e.g., Prontosan®) help lift debris gently, minimizing the need for scrubbing. |
front 24
| back 24 Certain hydrogel-based cleansers retain moisture in the wound bed, reducing pain and promoting faster healing (Firlar et al., 2022). |
front 25
| back 25 Mild antimicrobial agents reduce infection risk without harming wound tissue. |
front 26
| back 26 Oral: ~45 minutes – 1 hour |
front 27 Pre-medicate and schedule dressing changes during peak effects of medication. Some typical times for peak effects include:
| back 27 ~30 minutes |
front 28 Pre-medicate and schedule dressing changes during peak effects of medication. Some typical times for peak effects include:
| back 28 ~2-5 minutes |
front 29 Pre-medicate and schedule dressing changes during peak effects of medication. Some typical times for peak effects include: Parental (IV) opioids: | back 29 ~5-15 minutes |
front 30 Frequency and Technique | back 30 Fewer dressing changes and gentle techniques reduce trauma and discomfort. |
front 31 Frequency and Technique Comfort measures include: 1 | back 31 Adjust the frequency of changes based on wound needs. |
front 32 Frequency and Technique Comfort measures include: 2 | back 32 Soak adhered dressings with saline for nontraumatic removal. |
front 33 Frequency and Technique Comfort measures include: 3 | back 33 Avoid over-packing wounds. |
front 34 Frequency and Technique Comfort measures include: 4 | back 34 Use skin sealants to protect periwound skin from epidermal stripping. |
front 35 Frequency and Technique Comfort measures include: 5 | back 35 Use skin barriers to protect periwound skin from maceration. |
front 36 Frequency and Technique Comfort measures include: 6 | back 36 Use a contact layer over the wound bed to avoid trauma during removal. |
front 37 Frequency and Technique Comfort measures include: 7 | back 37 Warm topical products to room temperature before use. |
front 38 Oral Analgesics: | back 38 Oral analgesics should be based on pain characteristics and patient factors. PRN medications can be used before episodic/incidental pain, while routine administration is more beneficial for continual pain. |
front 39
| back 39
|
front 40
| back 40
|
front 41 Adjuvant Medications | back 41 enhance pain relief alongside primary treatments, especially for chronic and neuropathic pain. They help address multiple pain pathways and reduce primary analgesic doses, thus minimizing side effects (Kirkcaldy et al., 2023). |
front 42 Types of Adjuvant Medications Adjuvant medications, though intended for other conditions, can help manage wound-related pain: | back 42 Antidepressants ; Anticonvulsants ; Muscle Relaxants ; Baclofen (Lioresal®) and Cyclobenzaprine (Flexeril®) |
front 43 Adjuvant Medications Baclofen (Lioresal®) and Cyclobenzaprine (Flexeril®): | back 43 Alleviate spasms and chronic wound pain but may lead to drowsiness, dizziness, or dependency. |
front 44 Adjuvant Medications Anticonvulsants
| back 44 Reduce excitatory neurotransmitter release to manage neuropathic pain. Side effects are drowsiness and dizziness. |
front 45 Adjuvant Medications Serotonin-Norepinephrine Reuptake Inhibitors (SNRIs): | back 45 Duloxetine (Cymbalta®) and venlafaxine (Effexor®) relieve neuropathic and musculoskeletal pain but may cause nausea, dizziness, and insomnia. |
front 46 Adjuvant Medications Antidepressants
| back 46 Amitriptyline (Elavil®) and nortriptyline (Pamelor®) increase serotonin and norepinephrine, helping ease neuropathic pain (e.g., diabetic neuropathy). Side effects include dry mouth, constipation, and drowsiness. |
front 47 Adjuvant Medications Benefits and Considerations | back 47 The use of adjuvant medications allows for combining different medication types for a synergistic effect, enhancing pain relief with reduced dosage and side effects. |
front 48 Adjuvant Medications: Benefits | back 48
|
front 49 Adjuvant Medications: Considerations | back 49
|
front 50 Which strategies would provide the most comprehensive approach to managing wound pain? Using only NSAIDs and opioids for all pain relief Only using a topical analgesic like lidocaine Combining pharmaceutical and non-pharmaceutical strategies Elevating the limb and using an adherent dressing | back 50 Combining pharmaceutical and non-pharmaceutical strategies |
front 51
| back 51 topical lidocaine |
front 52
| back 52 chronic or neuropathic pain. |
front 53 Which is a non-pharmaceutical method for relieving wound pain? Using nonsteroidal anti-inflammatory drugs (NSAIDs) to reduce inflammation and pain Applying lidocaine (Lidoderm) gel to the wound Elevating the affected limb Using opioid medications like morphine (Oramorph) | back 53 Elevating the affected limb |
front 54 How does pain impact the wound healing process? Pain increases blood flow to the wound area, speeding healing. Pain increases the release of stress hormones that suppress the immune system. Pain reduces inflammation, helping the wound heal faster. Pain enhances oxygen supply to the wound, promoting healing. | back 54 Pain increases the release of stress hormones that suppress the immune system |
front 55 Which type of pain is often described as burning, stabbing, or shooting in nature? Nociceptive pain Visceral pain Neuropathic pain Somatic pain | back 55 Neuropathic pain * Neuropathic Pain is caused by damage, lesions, or disease affecting the somatosensory nervous system. Because the nerves themselves are misfiring or injured, patients classically describe this sensation as burning, stabbing, shooting, tingling, or like an "electric shock". Common examples include diabetic neuropathy and sciatica. [1, 2, 3, 4] |
front 56 What is the primary advantage of using topical analgesics for wound pain management? They provide systemic pain relief. They reduce the risk of systemic side effects. They work faster than oral analgesics. They enhance the immune response. | back 56 They reduce the risk of systemic side effects. |
front 57 Which is a key consideration when selecting a dressing to minimize wound pain? The dressing should adhere tightly to the wound bed. The dressing should promote a dry wound environment. The dressing should be non-adherent. The dressing should be opaque. | back 57 The dressing should be non-adherent. * Adherent dressings can stick to the wound bed, causing pain and damaging the tissue when the dressing is removed. |