Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM Module 16
front 1  Can you tell which is a VLU, arterial ulcer, mixed venous-arterial ulcer, and DFU? | back 1 Arterial ulcers are found on the foot and appear punched out with a dry, pale, or necrotic wound bed. The skin may be shiny and hairless with trophic nail change (thickening) due to a lack of circulation. |
front 2  Can you tell which is a VLU, arterial ulcer, mixed venous-arterial ulcer, and DFU? | back 2 DFUs are found on the bottom of the foot, especially on pressure points (e.g., heels or balls of the feet) (DynaMed, 2024a). They can look round or punched out with varying depths. A callus or dry skin often surrounds the wound. |
front 3  Can you tell which is a VLU, arterial ulcer, mixed venous-arterial ulcer, and DFU? | back 3 Mixed venous-arterial ulcers are a combination of both venous and arterial insufficiencies, meaning the veins and arteries are compromised (Jais, 2023). They are more complex because they involve both venous stasis and ischemia. |
front 4  Can you tell which is a VLU, arterial ulcer, mixed venous-arterial ulcer, and DFU? | back 4 VLUs are usually highly exudative, painful, shallow wounds with irregular edges between the ankle and shin, often in the gaiter area. They may be covered with fibrous slough and/or ruddy granulation tissue. The lower extremity (LE) will be edematous and often has hemosiderin staining around the wound. |
front 5 T I M E R S | back 5 Tissue management Infection control and inflammation Moisture balance Edges of wound Repair/regeneration Social factors
|
front 6  Debriding Eschar The need to debride eschar should be assessed with every dressing change * Remember that: | back 6
|
front 7 Moisture Maintenance: Ensure a moist wound environment for optimal healing. Dressings should align with wound characteristics. Some examples include: | back 7
|
front 8 Debridement should be appropriate to the patient’s condition and consistent with overall management goals. Types of debridement include: | back 8
|
front 9 What is a TCC and what does it do? | back 9 TCCs are the gold standard for offloading most DFUs and can be used for certain arterial ulcers (DynaMed, 2024a). A TCC redistributes pressure across the entire foot and lower leg, which can:
|
front 10 Removable Cast Walkers and Boots Removable cast walkers and boots can be adjusted to the patient’s comfort level. They allow for easier access to inspect the wound and provide wound care, especially in the infected wound or ischemic wound where TCC is not indicated. Types include (Bowers & Franco, 2020): | back 10
|
front 11 These devices are easier to use than TCCs. However, patients may remove them, which ultimately hinders pressure reduction and can minimize healing (DynaMed, 2024a). Therefore, it is important to remind patients to wear their walkers or boots as much as possible. What is it? | back 11 Removable cast walkers and boots |
front 12 What is iTCC | back 12 Instant Total Contact Casting (iTCC) is a modified approach to traditional TCC that offers many of the same benefits but is faster and easier to apply. iTCC involves converting a removable cast walker into an offloading device that mimics the effects of a traditional TCC by making it non-removable—typically by wrapping it with cohesive or casting material |
front 13 Key Takeaways: * Key aspects of wound care | back 13 The TIMERS framework addresses key aspects of wound care: Tissue management, infection control, moisture balance, wound edge care, repair/regeneration, and social factors. |
front 14 Key Takeaways: Moisture | back 14 Maintaining moisture balance is essential for wound healing, using dressings that manage drainage or add moisture depending on the wound's condition, ensuring it never dries out or becomes overly moist. |
front 15 Key Takeaways: Pressure relief | back 15 Offloading provides pressure relief, pain reduction, and protection against further trauma to the ulceration. Total contact casts (TCCs) are considered the “gold standard” for offloading DFUs. |
front 16 Compression is a primary therapy for ___s. | back 16 VLUs While compression alone may not heal every VLU, it is essential for promoting healing and reducing recurrence. The effectiveness of compression therapy depends on the skill of the person applying it and patient adherence to wearing compression garments or bandages, a frequent challenge with patients with VLU. |
front 17 Levels of Compression Therapy | back 17 Compression therapy is available in varying degrees of pressure, measured in millimeters of mercury (mmHg). |
front 18 Level Pressure Amount (mmHg) High | back 18 30 to 40 |
front 19 Level Pressure Amount (mmHg) Medium | back 19 20 to 30 |
front 20 Level Pressure Amount (mmHg) Low | back 20 14 to 17 |
front 21  What condition best describes this image? | back 21 Cellulitis Bacterial infection of deeper skin tissue |
front 22  What condition best describes this image? | back 22 Erysipelas Bacterial infection of the upper dermis, presents as bright red skin with induration and sharply demarked edges |
front 23 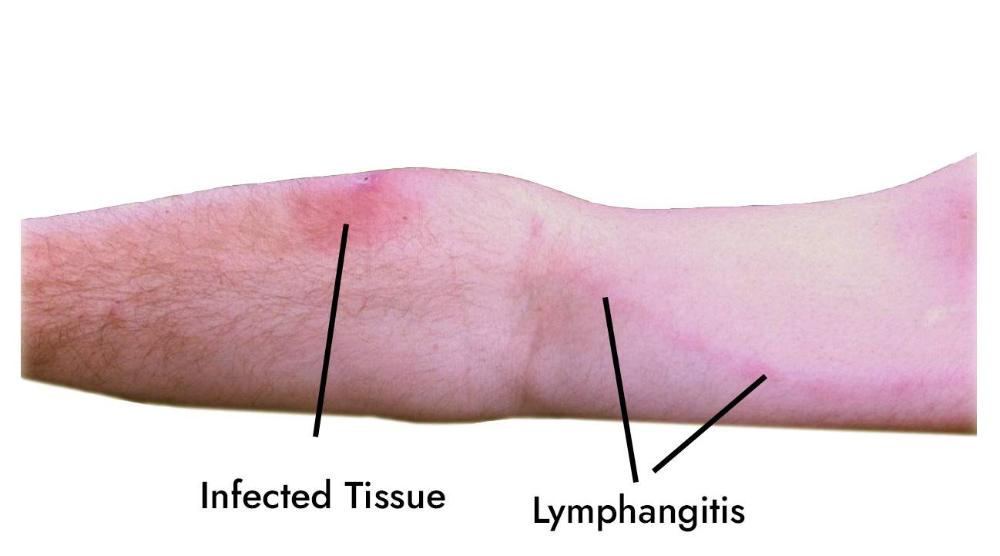 What condition best describes this image? | back 23 Lymphangitis Infected lymph vessels with distinctive red streak traveling along the lymphatic vessels |
front 24  What condition best describes this image? | back 24 Bacterial or Fungal infection & Lymphangitis Infected lymph vessels with distinctive red streak traveling along the lymphatic vessels Deep skin folds from swelling can get infected by bacteria or fungus |
front 25  What condition best describes this image? | back 25 Lymphatic papillomatosis Lumpy, cobblestone-looking, firm, raised projections resulting from dilated surface lymphatic vessels or lymph accumulation |
front 26  What condition best describes this image? | back 26 Lymphorrhea Weeping of light, amber-colored, protein-rich, lymph fluid through the skin |
front 27 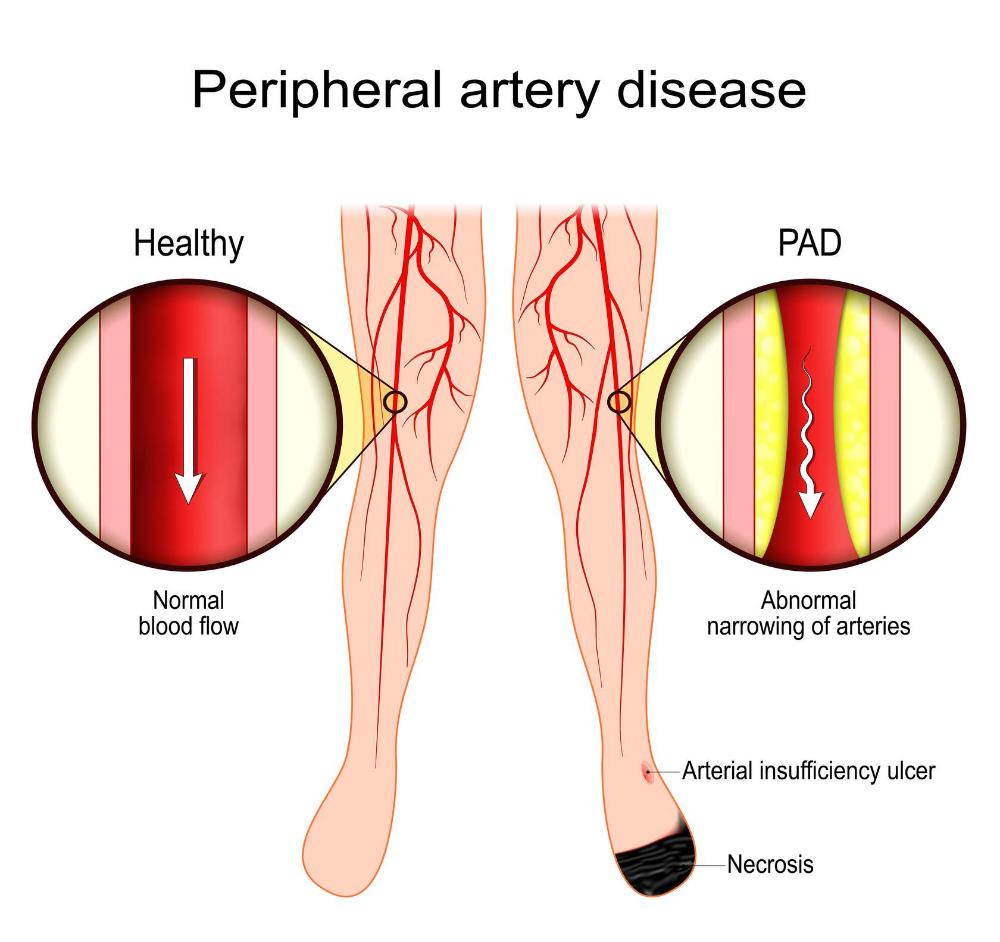 Peripheral artery disease Arterial ulcers develop because there is not enough blood flow to the area. This must be addressed. Otherwise, tissue viability may decrease, and wound healing may be delayed. Multiple strategies are employed to improve the conditions for wound healing. Goals of treatment should include: | back 27
|
front 28 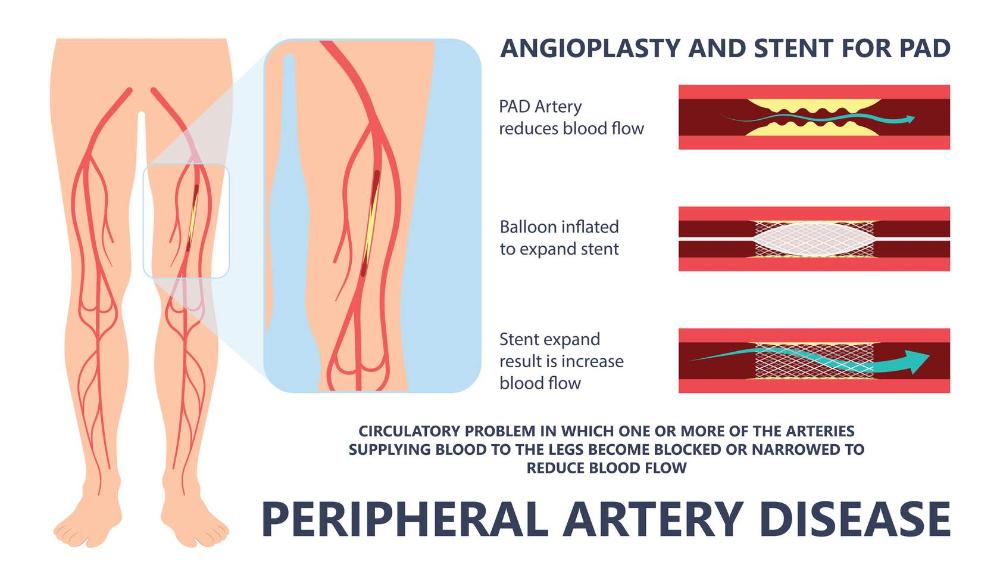 Revascularization Adequate arterial blood flow is required for wound healing in the lower limb. Surgical methods and less invasive measures can improve the vascularization of the affected limb. Endovascular procedures, such as angioplasty or stent placement, open narrowed arteries. Bypass surgery (e.g., femoral-popliteal bypass) helps create a new route for blood flow around blocked arteries. | back 28 Both open surgery and endovascular repair are valid approaches, depending on the disease severity and patient-specific factors (Bryant & Nix, 2024). The decision to pursue surgery must balance the procedure's risks against the potential benefits of improved blood flow and healing. |
front 29 Margaret's revascularization surgery is successful. What is the next best step in managing her arterial ulcer post-surgery? | back 29 Use a non-occlusive, moisture-balancing dressing to promote healing. |
front 30 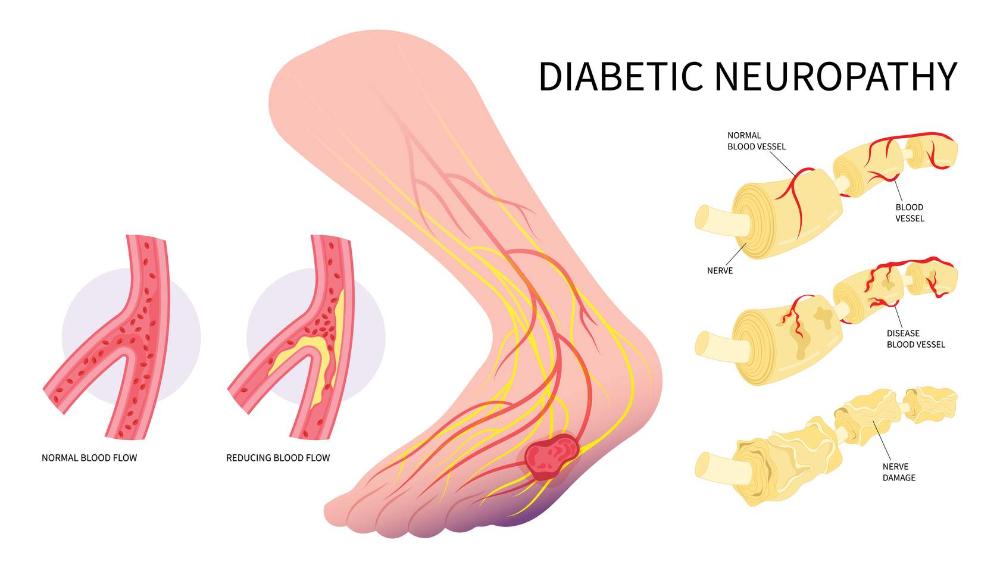 The patient with diabetes and a wound presents a complex situation when it comes to healing. The statistics are sobering (Armstrong et al., 2023): | back 30
DFUs result from biochemical (e.g., glycemic control), peripheral neuropathy, and vascular factors. |
front 31 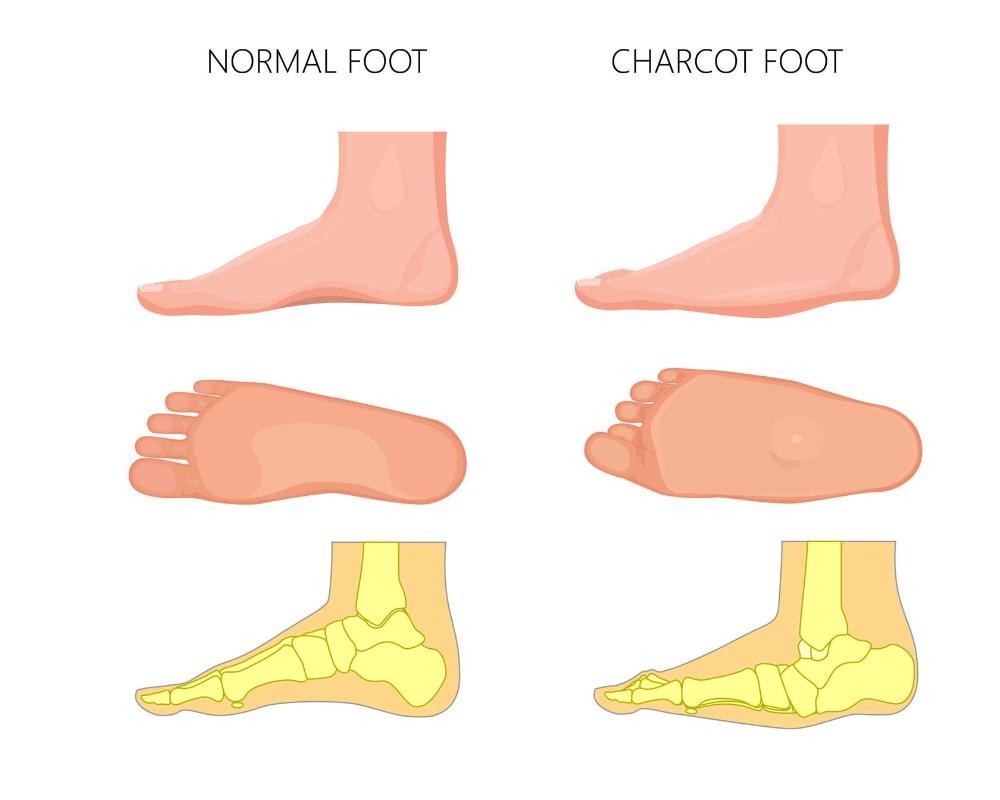 Checking for Charcot Neuroarthropathy (CNO) | back 31 Charcot neuroarthropathy (i.e., Charcot Foot) is a sterile inflammatory condition affecting individuals with diabetes who have neuropathy. This condition leads to damage in bones, joints, and soft tissues in the foot, presenting as a red, hot, swollen foot (Senneville et al., 2023). If left untreated, Charcot foot can progress to fractures and dislocations, resulting in a severely deformed foot. Diagnosis is often delayed, leading to worsened damage and lengthening treatment time. |
front 32 Geraldo, a 60-year-old with CVI and PAD, presents with a mixed venous-arterial ulcer. His ABI is 0.7. What type of compression therapy would be BEST? | back 32 Low-level compression Low-level compression between 23 and 30 mmHg would be BEST for those with an ABI of 0.7 as it helps improve venous return without reducing arterial flow. Complete avoidance of compression would allow venous hypertension to persist, leading to the worsening of the venous component of the ulcer. Therapeutic compression between 30 and 40 mmHg is too high for a patient with an ABI of 0.7 and could worsen ischemia. While IPC is helpful in some cases, it is not typically considered when traditional compression methods are not tolerated or effective, and low-level compression is still needed. |
front 33  A 58-year-old man presents with the wound seen in the image on the heel of his foot. The wound is deep with necrotic tissue, heavy slough, and some areas of exposed tissue. The surrounding skin is inflamed, erythematous, and appears swollen. The patient has a history of uncontrolled diabetes and reports difficulty feeling sensations in his feet. His pulses are diminished, but he denies any rest pain. Upon palpation, the area is warm and tender, and there is moderate purulent drainage. The ABI is 0.85. What is the BEST action you should consider FIRST for managing this DFU? Refer for revascularization to improve blood flow to the foot. Start systemic antibiotics to control the infection and offload with a TCC. Debride, irrigate, apply calcium alginate to open areas and start offloading with TCC. Check CRP and ESR for the presence of infection before next action. | back 33 Check CRP and ESR for the presence of infection before next action. * The image and description suggest there is an infection in this wound. However, signs of infection are often masked in patients with diabetes, making the use of serum biomarkers like CRP, ESR, and PCT useful in identifying the presence of infection. Debridement is appropriate, however, in the presence of infection, a TCC is contraindicated. The patient's ABI is 0.85, indicating mild PAD, not critical limb ischemia requiring revascularization. Systemic antibiotics should not be used for suspected infection and should be culture driven, making the best option checking for infection via chemical biomarkers. |
front 34 Which type of ulcer is typically associated with brownish discoloration, swelling, and shallow wounds with irregular edges? Diabetic foot ulcer Arterial ulcer Venous leg ulcer Mixed venous-arterial ulcer | back 34 Venous Leg Ulcer |
front 35 Which of the following dressings is most appropriate for an exudative venous leg ulcer? Hydrogel Honey-impregnated dressing Transparent film Calcium alginate | back 35 Calcium alginate |
front 36 What is the MAIN reason for using compression therapy in patients with venous leg ulcers? To reduce arterial pressure To debride necrotic tissue To prevent tissue ischemia To promote venous blood return | back 36 To promote venous blood return |
front 37 What advice should a healthcare provider give a patient with venous leg ulcers to prevent recurrence? Avoid walking long distances. Wear compression stockings daily. Keep legs elevated for 30 minutes once a week. Avoid wearing tight-fitting shoes. | back 37 Wear compression stockings daily. |
front 38 Which of the following therapies would be BEST for a deep arterial ulcer that will not heal? Electrical stimulation Negative Pressure Wound Therapy (NPWT) Enzymatic debridement Hyperbaric Oxygen Therapy (HBOT) | back 38 Negative Pressure Wound Therapy (NPWT) Note: * HBOT is beneficial in specific conditions like acute arterial insufficiency related to crush injury, but it is not routinely used as the primary therapy for deep arterial ulcers. NPWT supports wound healing in deep, non-healing ulcers by reducing wound size, improving perfusion, and managing exudate |
front 39 When applying a compression bandage, where should you start to wrap? At the knee At the base of the toes At the mid-calf At the ankle | back 39 At the base of the toes |
front 40 Which condition must be stabilized before applying compression therapy in patients with a mixed venous-arterial ulcer? Neuropathy Diabetes mellitus Peripheral arterial disease (PAD) Hypertension | back 40 Peripheral arterial disease (PAD) |
front 41 What should patients with diabetic foot ulcers do daily to prevent worsening of the condition? Use tight-fitting shoes for support Walk barefoot around the house Apply bandages directly to ulcers Inspect their feet for signs of injury or infection | back 41 Inspect their feet for signs of injury or infection |
front 42 In what situation should dry eschar be left intact rather than debrided? On venous leg ulcers When the wound is infected When the patient is on antibiotics In ischemic limbs | back 42 In ischemic limbs Note: * Infected wounds require eschar removal to prevent further complications. Dry eschar should be left intact in ischemic limbs to prevent further damage and potential infection. |
front 43 Which of the following strategies is recommended to reduce pressure on diabetic foot ulcers and promote healing? Topical antibiotics Footwear modifications Exercise therapy Heat therapy | back 43 Footwear modifications |
front 44 What is a typical characteristic of an arterial ulcer? Punched-out appearance Brownish discoloration Round with callused edges Shallow wounds with irregular edges | back 44 Punched-out appearance zz |
front 45 What is the main benefit of using negative pressure wound therapy (NPWT) for chronic wounds? Provides high moisture balance Promotes granulation tissue formation Reduces bacterial load Removes necrotic tissue | back 45 Promotes granulation tissue formation HOW: The suction creates mechanical forces that stimulate cellular growth, rapidly building new, healthy tissue to fill deep NPWT also reduces bacterial load. It draws out bacteria and creates an optimal moist, closed environment, which reduces the risk of recurrent infections |
front 46 What role does glycemic control play in the management of diabetic foot ulcers (DFUs)? Enhances immune system function Increases vascular resistance Encourages the formation of calluses Reduces oxygen levels in tissues | back 46 Enhances immune system function * Uncontrolled hyperglycemia delays healing by causing nerve damage, impairing circulation, and weakening the body's ability to fight off bacterial infections |
front 47 For patients with venous leg ulcers, how often should compression stockings be replaced to ensure effectiveness? Once a month Every 6 months Every 12 months Every 2 years | back 47 Every 6 months |