Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM Module 14: Wound Care - Pressure Injuries
front 1 What management goal should be a PRIORITY, if you have a patient that is high risk for a pressure injury (PI)? - Educate them and their caregivers on the importance of proper nutrition. - Apply a moisture barrier cream daily to protect their skin from incontinence. - - Use foam cushions to support their body in her current position. | back 1 Est. a repositioning schedule to relieve pressure on vulnerable areas every 1-2 hrs. For patients at high risk of PIs, repositioning should be the PRIORITY because it helps redistribute pressure and prevents prolonged pressure on the same areas, which is the primary cause of PIs. While nutrition is important, it is secondary to the immediate need to offload pressure. Moisture management is important but does not directly address the key risk of pressure, which is the main cause of injury in high-risk patients. Foam cushions may help with pressure distribution, but without regular repositioning, they are insufficient to prevent PIs on their own. |
front 2
| back 2 Limited mobility, poor nutrition, moisture, and comorbidities elevate PI risk. High-risk patients require frequent repositioning, advanced support surfaces, and nutritional monitoring. |
front 3
| back 3 Adjust care plans for high-, moderate-, and low-risk patients with strategies ranging from proactive skin care to basic prevention routines. |
front 4
| back 4 Interdisciplinary collaboration is integral to providing effective patient-centered care |
front 5 Support Surface Goals: When caring for pt.'s at risk for PI's it's important to use appropiate support surfaces for PI prevention. | back 5
|
front 6 Guidelines for Using Support Surfaces: Support surfaces alone cannot prevent or heal PIs; they must be part of a comprehensive prevention and treatment plan. Key considerations include | back 6
|
front 7 Alternating Pressure (AP) Mattresses /Overlays | back 7 Mattresses and overlays that are designed to reduce the risk of PIs by periodically redistributing pressure across different areas of the body (Baranoski & Ayello, 2020). These surfaces use air cells that inflate and deflate cyclically, creating alternating high and low-pressure zones. The alternating inflation and deflation of air cells shift pressure from one area of the body to another. |
front 8 Air Fluidized Beds | back 8 These beds are filled with tiny beads suspended in warm air, creating a fluid-like effect. When a patient lies on the bed, their body is partially immersed in the beads, which contour around them, distributing their weight evenly. The fluid-like environment allows the patient’s body to float, minimizes shear and pressure, boosts immersion and envelopment, significantly reducing the risk of PIs. |
front 9 Air Fluidized Beds | back 9 These beds also help manage the microclimate by wicking away moisture and maintaining a consistent temperature. This helps keep the skin dry and reduces the risk of maceration and moisture-associated skin damage (MASD). |
front 10 Air Fluidized Beds: Contraindication | back 10 For use with patients who have an unstable spinal cord injury. |
front 11 Air Fluidized Beds are best for what stage PIs | back 11 Consider an air-fluidized bed for patients with stage 3 or 4 PIs (EPUAP et al., 2019). |
front 12 Mattress Considerations When choosing a mattress, you want to factor in the patient’s weight and how the mattress can distribute that weight, as follows (Baranoski & Ayello, 2020; EPUAP et al., 2019): For At-Risk Patients | back 12 Use reactive air or high-specification reactive single-layer foam mattresses or overlays. |
front 13 Mattress Considerations When choosing a mattress, you want to factor in the patient’s weight and how the mattress can distribute that weight, as follows (Baranoski & Ayello, 2020; EPUAP et al., 2019): For Patients with Existing PIs | back 13 Choose a support surface that offers better pressure redistribution, shear reduction, and microclimate control. This is especially important if:
|
front 14 Mattress Considerations When choosing a mattress, you want to factor in the patient’s weight and how the mattress can distribute that weight, as follows (Baranoski & Ayello, 2020; EPUAP et al., 2019): Advanced Surfaces for Severe Injuries | back 14 Consider alternating pressure, low air loss beds, or air-fluidized surfaces, particularly for patients with stage 3 or 4 PIs. However, be cautious with air-fluidized beds as they can increase the risk of dehydration due to high airflow. |
front 15 Sarah develops a Stage 1 PI on her heel. Which support surface intervention is MOST appropriate to prevent the PI from worsening? Place a pillow under the knees to elevate the legs. Use a heel suspension device to offload pressure completely from the heels. Apply a soft foam dressing directly to the heel and avoid further interventions. Increase the frequency of turning to every 3 hours. | back 15 Use a heel suspension device to offload pressure completely from the heels. *A heel suspension device is MOST appropriate to promote healing because it effectively offloads all pressure from the heel. Placing a pillow under the knees to elevate the legs may inadvertently increase pressure on the heels rather than relieve it. While a dressing may protect the skin, it does not adequately offload pressure from the heel. While more frequent turning is beneficial, it may not fully address the need for targeted offloading of the heel. |
front 16
| back 16 Redistribute pressure, enhance immersion, and conform to the body’s shape to minimize concentrated pressure points and improve comfort. |
front 17
| back 17 Use foam overlays or reactive mattresses; for those with existing PIs or severe injuries, consider high-tech solutions like alternating pressure or low air loss beds to manage microclimates and prevent worsening. |
front 18
| back 18 ift high-risk areas entirely off surfaces, reducing pressure on bony prominences such as heels or elbows. |
front 19
| back 19 wear, ensure proper fit and positioning, and avoid excessive bedding that can hinder pressure redistribution. Perform hand checks or use pressure mapping to detect "bottoming out." |
front 20 Positioning for Critically Ill considerations | back 20 These patients may require careful repositioning strategies that account for hemodynamic and oxygen stabilization. These strategies include frequent, small, gradual shifts in body positions. |
front 21 Tips for effective positioning: Many strategies can be used to position a patient effectively. These strategies should (Gould et al., 2023) | back 21
|
front 22 The Rule of 30 | back 22 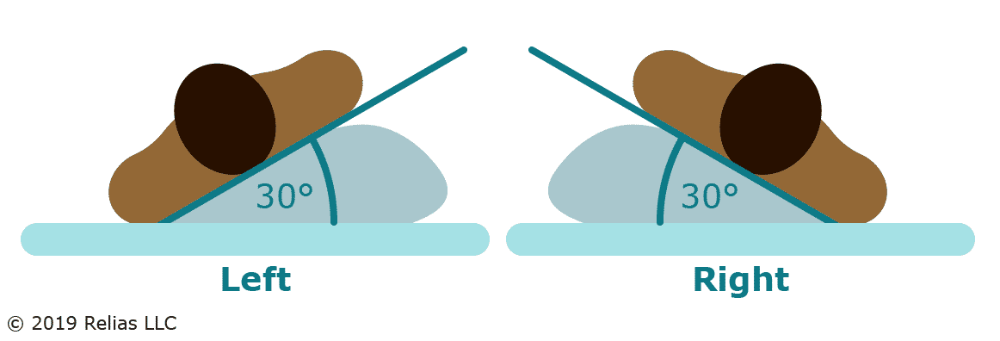 Keep the head of the bed elevated no more than 30° to reduce pressure (EPUAP et al., 2019). Rotate patients 30° on their side in a lateral motion to offload pressure from the greater trochanters and distribute weight on fattier tissue areas. The semi-Fowler's position is preferred when elevation above 30° is medically necessary. |
front 23 The Five Pillow Rule The “5 Pillow Rule” is a positioning technique used to prevent pressure injuries by using five pillows placed strategically to support various parts of the body when the patient is lateral in bed: | back 23
|
front 24 Heel Positioning: | back 24 Heels are one of the most common areas on which a PI can develop in bedbound patients. |
front 25 Heel Positioning: Thus, it is important to position the heel in such a way to keep pressure off them, as follows: At-Risk or Stage 1 and 2 PIs | back 25 Ensure heels are free of the bed surface, using a pillow or foam cushion under the calves for short-term relief (stage 1 or 2 PIs) (EPUAP et al., 2019). Some facilities may have specially designed suspension devices for heels. |
front 26 Heel Positioning: Thus, it is important to position the heel in such a way to keep pressure off them, as follows: | back 26 Long-Term Support Consider heel suspension devices for long-term use, especially in patients with stage 3 or greater PIs (EPUAP et al., 2019). When positioning heels, ensure the pressure is taken off completely so that the patient's leg weight spreads out over the lower part of the leg. Be careful not to put pressure on the Achilles tendon and the popliteal vein behind. |
front 27 Heel Positioning: For those who spend most of their time seated, consider the following recommendations (EPUAP et al., 2019). | back 27 Dynamic Weight Shifting This means leaning the chair back and lifting the legs to decrease stress on the lower back. Ensure the feet are well supported and angle the seat from 25° to 30°. This helps avoid sliding down and reduces stress on the lower back, sitting bones, and tailbone. |
front 28 Heel Positioning: For Seated patients- | back 28 Repositioning should occur every hour for seated patients (National Pressure Injury Advisory Panel [NPIAP], 2023). Encourage pressure relief maneuvers such as:
Micro shifts (5° to 10° or a 5 to 10 second lift) with a return to the same position may not be sufficient for pressure relief |
front 29 Sarah is still having difficulty mobilizing and cannot sit out of bed. What is the MOST appropriate positioning strategy? Position Sarah prone for prolonged periods to relieve pressure on her back. Use continuous lateral rotation therapy and maintain the patient in a 30° lateral position. Elevate the head of the bed to 45° and place a pillow under the knees. Reposition the Sarah once per shift and use foam padding for support. | back 29 Use continuous lateral rotation therapy and maintain the patient in a 30° lateral position. Continuous lateral rotation therapy combined with the 30° lateral position helps redistribute pressure and reduce the risk of PIs, particularly when unable to mobilize or sit out of bed. Prone positioning can increase the risk of PIs on the face and chest if not carefully managed. Elevating the head of the bed to 45° and placing a pillow under the knees may increase pressure on the sacrum and heels, leading to a higher risk of PIs. Repositioning once per shift is insufficient for preventing pressure injuries in a high-risk, immobile patient. |
front 30
| back 30 Tailor repositioning plans to the patient’s condition, mobility, and risk level. Use strategies like the 30° lateral position or continuous lateral rotation therapy to offload pressure for immobile patients. |
front 31
| back 31 Use tools such as the “5 Pillow Rule” for proper alignment, heel suspension devices to protect vulnerable areas, and friction-reducing sheets to minimize shear forces. |
front 32
| back 32 Facilitate early movement, including sitting and ambulation, as soon as medically feasible. Gradually increase sitting duration while monitoring tissue tolerance. |
front 33
| back 33 For chair-bound patients, implement dynamic weight-shifting techniques like leaning, standing, or arm push-ups to relieve pressure on the sacrum, sitting bones, and heels. |
front 34 PIs in darker skin tones PIs in patients with darker skin tones, potentially missing early signs. To mitigate these biases when examining a darker skin tone, practice the following: | back 34
|
front 35  What is this rash called | back 35 ITD appears as a mirror image in skin folds, as linear and partial-thickness wounds (Baranoski & Ayello, 2020). These may progress from mild redness to intense inflammation, with erosion, oozing, exudate, maceration, and crusting. |
front 36 ITD | back 36 ITD, or intertrigo , is an inflammatory condition that occurs in opposing skin surfaces due to moisture buildup (Baranoski & Ayello, 2020). It commonly affects skin folds under the breasts, in the axillae, or the inguinal and abdominal regions, especially in those with obesity. |
front 37 ITD treatment | back 37
|
front 38 Candida Infections Candida infections, or yeast infections- | back 38 Thrive in warm, moist environments (Flowers, 2020). Candidiasis is one of the most common skin diseases in the elderly due to alterations in the skin barrier function of the skin. Diagnosis is usually made on basis of clinical presentation but can be confirmed by skin scrapings under a microscope. |
front 39 ITD caused by candida will look like | back 39  Consolidated or patchy areas with small round red papules, pustules, and satellite lesions. The area is typically tender and pruritic. They may also appear as partial-thickness wounds with a beefy pink base, although not all skin rashes are caused by Candida; some may be due to dermatophytes or bacteria. |
front 40 Common locations for ITD caused by Candida | back 40 You will often see them in areas, such as:
|
front 41 Candida Risk Factors | back 41
|
front 42 Light Versus Dark Skin- Candida | back 42 Candida presents as a bright red central area with satellite lesions in light-skinned patients. In darker-skinned patients, it may appear as a lighter or darker skin tone or develop into a darker red or purplish hue. |
front 43 To manage Candida infections (Baranoski & Ayello, 2020; Flowers, 2020) | back 43 
|
front 44 Antifungal Practice Tips: | back 44
|
front 45 Antimicrobial textiles specifically designed for wicking moisture away from body folds are effective but can be expensive. Examples of such textiles include: | back 45 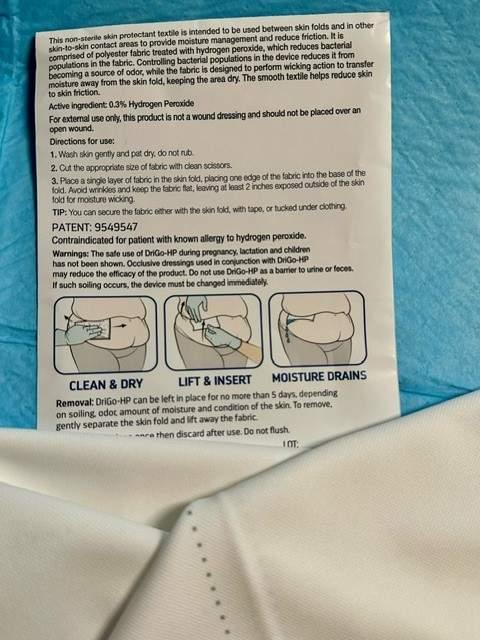
Severe or non-responsive cases may require systemic treatment. |
front 46 Moisture Barrier Creams and Ointments | back 46 Applied to the skin after drying helps keep the skin intact and reduce the risk of PIs. Barrier creams form a protective layer on the skin, preventing moisture from urine or feces causing irritation or breakdown. They are essential for patients with frequent incontinence to protect the skin from MASD. |
front 47 Moisture Barrier Creams and Ointments Petroleum-Based Ointments: | back 47
|
front 48 Moisture Barrier Creams and Ointments Zinc Oxide-Based: | back 48
|
front 49 Moisture Barrier Creams and Ointments Silicone-Based: (e.g., dimethicone) | back 49
|
front 50 Moisture-Associated Skin Damage (MASD) | back 50 MASD results from prolonged exposure to moisture rather than pressure (Baranoski & Ayello, 2020). |
front 51 MASD has been subdivided into key areas with specific best practice statements around prevention and management for each area (Flecther et al., 2020): | back 51
|
front 52 Incontinence-Associated Dermatitis (IAD) | back 52 A subset of MASD, IAD occurs due to prolonged exposure to urine or stool. It commonly affects the buttocks, perineum, inner thighs, or groin (Baranoski & Ayello, 2020). IAD presents as consolidated or patchy areas of skin damage or partial-thickness wounds without necrosis, which is associated with pressure-related ischemia. |
front 53 Blisters Under Incontinence Briefs | back 53 Blisters caused by pressure from leg bands or waistbands of incontinence briefs are classified as PIs. However, blisters or skin tears resulting from adhesive tabs are categorized as medical adhesive-related skin injuries (MARSI). |
front 54 What does (MARSI) stand for? | back 54 Medical adhesive-related skin injuries |
front 55 Sarah has started to show early signs of incontinence-associated skin breakdown in the sacral area. What would be the BEST skincare approach in this situation? Apply a petrolatum-based ointment as needed. Use a pH-balanced no-rinse cleanser and moisture barrier cream. Thoroughly wash all the zinc oxide barrier from the area with every reapplication. Cover the area with a hydrocolloid dressing and change it daily. | back 55 Use a pH-balanced no-rinse cleanser and moisture barrier cream.Using a pH-balance no-rinse cleanser and moisture barrier cream would be BEST because they protect it from further moisture-related damage and skin breakdown. Applying a petrolatum-based ointment may offer some protection but does not address the need for regular cleansing and immediate intervention. Zinc oxide barriers should not be scrubbed off with every cleansing and reapplication. Hydrocolloid dressings are not the best first-line intervention for early skin breakdown due to moisture; managing incontinence directly is more important. |
front 56
| back 56 Use pH-balanced cleansers and barrier products to protect the skin from breakdown. Avoid over-cleaning, hot water, or harsh rubbing to maintain skin integrity, especially after incontinence episodes. |
front 57
| back 57 Monitor for moisture buildup, redness, or signs of Candida infections, especially in skin folds. Treat intertriginous dermatitis (ITD) with gentle drying and antifungal creams as needed. |
front 58
| back 58 Differentiate between pressure injuries, MASD, and IAD (incontinence-associated dermatitis) for appropriate intervention. MASD results from prolonged moisture exposure and may require targeted hygiene and barrier protection. |
front 59
| back 59 Use no-rinse cleansers, pre-moistened wipes, and moisture barrier creams to protect sacral and perineal skin from irritation. Incorporate absorbent pads, briefs, or fecal control systems to reduce moisture exposure. |
front 60 The TIMERS principle used for wound care management stands for (Bowers & Franco, 2020): | back 60 T Tissue management I Infection control and inflammation M Moisture balance E Edges of wound R Repair/regeneration S Social factors |
front 61 Debridement | back 61 Debridement promotes healing by removing devitalized tissue and biofilm and should align with the patient’s condition and management goals. |
front 62 TRUE / FALSE Multiple debridement sessions may be needed until only healthy granulation tissue remains | back 62 True |
front 63 Wound Cleansing | back 63 Cleanse the wound and peri-wound with every dressing change unless contraindicated. Choose a noncytotoxic cleanser for uninfected wounds or a cytotoxic one for infected wounds. Irrigate at appropriate pressure and address tunneling and undermining. |
front 64 Debridement Guidelines | back 64 Remove necrotic tissue or biofilm to promote healing. Methods include surgical (sharp), autolytic, bio-surgical (maggots), enzymatic, and mechanical debridement. Select the method based on the patient's condition, pain tolerance, and management goals. B Biosurgical (maggots) E Enzymatic A Autolytic M Mechanical debridement S Sharps (conservative, surgical) |
front 65 Moisture Balance | back 65 Maintain a moist wound environment. Match dressing type to wound characteristics (e.g., alginates for drainage, hydrogels for dry wounds). Use silicone-based dressings for fragile skin to minimize trauma. |
front 66 B E A M S | back 66 Bio surgical - maggots Enzymatic Autolytic Mechanical debridement Sharps (conservative, surgical) |
front 67 Infection Management | back 67 Monitor for signs of infection, including delayed healing, redness, or exudate. Address biofilm based on clinical signs or tissue biopsy if available. Use systemic antibiotics only for systemic infection (e.g., sepsis, cellulitis). |
front 68  When to Debride: * Image of unstageable sacral PI | back 68 Mechanical, autolytic, enzymatic, and/or biological methods may be considered if there is no urgent need for sharp debridement (EPUAP et al., 2019). |
front 69 In general, debridement can be considered when there is evidence of: | back 69
|
front 70  Eschar The need to debride eschar should be assessed with every ___ ___ (EPUAP et al., 2019). | back 70 dressing change |
front 71 Dry, stable eschar | back 71 Should NOT be disturbed in ischemic limbs and heels. * However, removal of eschar may be considered if wound infection is suspected. |
front 72 Signs / Symptoms of Unstable Eschar include: | back 72
|
front 73 fluctuance | back 73 Is a wave-like or boggy, soft, "squishy" sensation felt when palpating a swelling or lump |
front 74 Alert the patient’s primary healthcare provider if unstable eschar is present, as the patient may require immediate ___ ____ (EPUAP et al., 2019). | back 74 surgical debridement |
front 75 WOUND TYPE: Draining/exudative | back 75 DRESSING: To control drainage while keeping it off the peri-wound:
|
front 76 WOUND TYPE: Infected/inflamed | back 76 DRESSING:
|
front 77 WOUND TYPE: Necrotic To debride dead tissue | back 77 DRESSING:
|
front 78 WOUND TYPE: Dry (nondraining) | back 78 DRESSING: To add moisture-
|
front 79 ___-___ dressings (e.g., foam) can minimize pain or trauma during dressing changes, especially for fragile skin (EPUAP et al., 2019). | back 79 Silicone-based |
front 80
Biofilm, often resistant to antimicrobials, may require management based on clinical signs or tissue biopsy (EPUAP et al., 2019). | back 80 Characteristics that indicate the presence of infection |
front 81 Antiseptics Antiseptics used to manage the bioburden of wounds include (Norman et al., 2016): | back 81
The choice of antiseptic depends on the patient and the wound's condition. |
front 82 ____ ____ are reserved for confirmed systemic infections, like cellulitis or sepsis, and abscesses that require drainage to prevent further spread (EPUAP et al., 2019). | back 82 Systemic antibiotics |
front 83 __________ may need surgical interventions and treatment with IV antibiotics under the guidance of an infectious disease specialist. Sepsis, gas gangrene, and necrotizing fasciitis are all examples of such infections. | back 83 Severe, limb- or life-threatening infections |
front 84  What type of dressing can be used to manage the exudate of this wound? Hydrogel dressing Transparent film dressing Calcium alginate dressing Collagenase dressing | back 84 Calcium alginate dressing Calcium alginate dressings are highly absorbent, making them ideal for wounds with moderate to heavy exudate. They help manage wound drainage while also promoting autolytic debridement, which assists in removing slough and necrotic tissue. Hydrogel dressings are more appropriate for dry wounds, as they add moisture to the wound bed. Transparent film dressings are best used for superficial wounds or wounds with minimal exudate, as they do not absorb exudate and are not suited for wounds with necrotic tissue. While collagenase dressings are useful for enzymatic debridement, they are not the best choice for wounds with high exudate because they do not manage moisture as effectively as calcium alginate. |
front 85 ___ ___ dressings are highly absorbent, making them ideal for wounds with moderate to heavy exudate. | back 85 Calcium alginate |
front 86 Nutritional Guidelines- Consider the following recommendations for patients with PIs (EPUAP et al., 2019): Protein | back 86 1.2 to 1.5 g/kg/day or adjust based on patient needs |
front 87 Nutritional Guidelines- Consider the following recommendations for patients with PIs (EPUAP et al., 2019): Calories | back 87 30-35 kcal/kg/day |
front 88 Nutritional Guidelines- Consider the following recommendations for patients with PIs (EPUAP et al., 2019): Fortified Foods | back 88 Add to diet if nutritional needs are unmet |
front 89 Nutritional Guidelines- Consider the following recommendations for patients with PIs (EPUAP et al., 2019): Nutritional Supplements | back 89 Add to diet if nutritional needs are unmet |
front 90 Fortified Foods | back 90 Products that have nutrients—specifically vitamins, minerals, or fiber—added to them that are not naturally present or are present in small amounts |
front 91 Role Nutrition and Hydration:
| back 91
|
front 92
| back 92 for draining wounds |
front 93 Select dressings based on wound type: Use Hyrogels | back 93 dry wounds |
front 94 Select dressings based on wound type: Use Silver-Impregnated dressings for | back 94 Infected wounds |
front 95
| back 95 Monitor for infection signs like delayed healing or exudate, using antiseptics like silver or medical honey as needed. Debride unstable eschar carefully to remove biofilm or necrotic tissue but avoid disturbing dry eschar on ischemic areas like heels. |
front 96
| back 96 Patients with Stage 2 or higher PIs require 1.2 to 1.5 g/kg/day of protein and 30 to 35 kcal/kg/day. Add supplements like arginine, zinc, and antioxidants to support healing in malnourished or at-risk patients. |