Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Path 17
front 1 Gastric ulcers present with pain that is _____ by meals (eating stimulates _____ secretion in the stomach). Duodenal ulcers characteristically present with pain that _____ with meals (eating stimulates _____ secretion in the duodenum). | back 1 exacerbated, acid improves, bicarb |
front 2 What hereditary disease is characterized by an inherited mutation in one copy of the APC gene? _____ _____ _____ - inherited APC mutation (chromosome _____) | back 2 Familial Adenomatous Polyposis 5 |
front 3 Familial Adenomatous Polyposis: Thousands of _____ develop in _____ - high risk for _____
transformation | back 3 polyps, colon, malignant |
front 4 What is the most common cause of Vitamin B12 deficiency? _____ _____ gastritis | back 4 Chronic autoimmune gastritis |
front 5 Chronic autoimmune gastritis leads to destruction of parietal cells which secrete _____ _____ (_____ anemia) | back 5 intrinsic factor, pernicious |
front 6 Achalasia represents damage to the _____ cells of the _____ plexus. | back 6 ganglion myenteric |
front 7 Which type of hypersensitivity is responsible for chronic autoimmune
gastritis? | back 7 D. Type IV (T-cell mediated) |
front 8 Intrinsic factor deficiency in chronic autoimmune gastritis is best
explained by: | back 8 B. Loss of parietal cells due to T-cell–mediated damage |
front 9 Why are anti-intrinsic factor antibodies detected in chronic
autoimmune gastritis? | back 9 B. They are produced secondary to parietal cell destruction |
front 10 In chronic autoimmune gastritis, what is the role of anti-parietal
cell antibodies? | back 10 C. Are a consequence of parietal cell damage |
front 11 inner layers of the tract protrude through the muscular layer, meckel or zenker? | back 11 zenker |
front 12 A 70-year-old man presents with dysphagia, regurgitation of
undigested food, and chronic cough. Imaging reveals a
posterior pharyngeal outpouching. Which muscle is
primarily responsible for forming a sphincter and contributing to the
pathophysiology? | back 12 C. Cricopharyngeus this is Zenker's diverticulum |
front 13 In achalasia, LES tone is typically: | back 13 C. Increased |
front 14 A patient with Zenker diverticulum undergoes surgical treatment.
Which of the following interventions directly addresses the underlying
cause of this condition? | back 14 C. Cricopharyngeal myotomy |
front 15 Zenker: Herniation of ____ through a muscular defect due to increased ____ pressure | back 15 mucosa intraluminal |
front 16 An elderly patient presents with dysphagia,
regurgitation of undigested food, halitosis, and
recurrent aspiration pneumonia. What
is the most appropriate diagnostic test to confirm this
condition? | back 16 A. Barium contrast esophagogram Zenker diverticulum is suspected. |
front 17 Primary achalasia causes inability to relax the LES because
of: | back 17 C. Ganglion cell degeneration |
front 18 In Chagas disease, secondary achalasia is caused by destruction of
the: | back 18 C. Myenteric plexus |
front 19 What demographic is most commonly affected by Zenker diverticulum? _____ _____ | back 19 elderly males |
front 20 Between Mallory-Weiss syndrome and esophageal varices, which presents with painful hematemesis and which presents with painless hematemesis? | back 20 Painful hematemesis: mallory-weiss syndrome Painless hematemesis: esophageal varices |
front 21 Secondary achalasia in Chagas disease leads to failure of peristalsis
and: | back 21 A. Esophageal dilatation |
front 22 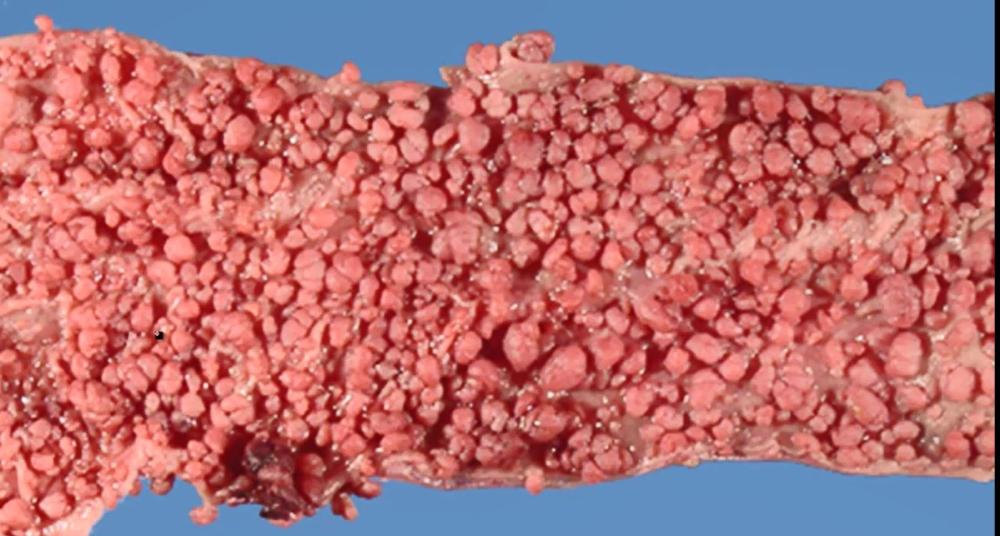 what is this? | back 22 FAP |
front 23 A patient has achalasia, alacrima, and ACTH-resistant adrenal
insufficiency. This syndrome is: | back 23 A. Allgrove syndrome |
front 24 The most feared complication of Boerhaave syndrome is: | back 24 Boerhaave syndrome |
front 25 What type hernias are found in about half of patients with Mallory-Weiss syndrome and are considered a strong predisposing factor? | back 25 hiatal hernias |
front 26 What test/imaging study is used to diagnose a Mallory-Weiss tear? _____ | back 26 Endoscopy |
front 27 Proximal esophageal atresia with the distal esophagus arising from the trachea. | back 27 TE fistula |
front 28 What is the likely diagnosis in a patient with alcohol use disorder who presents with epigastric pain and hematemesis following multiple episodes of vomiting (normal X-ray)? | back 28 Mallory-Weiss tear |
front 29 What are dilated submucosal veins in the lower 1/3rd of the esophagus | back 29 esophageal varices |
front 30 esophageal varices rise secondary to _____ hypertension | back 30 portal |
front 31 _____ is characterized by disordered esophageal motility due to inability to relax the _____ esophageal sphincter | back 31 Achalasia lower |
front 32 Dysphagia for both solids and liquids Putrid breath High LES pressure on esophageal manometry Bird-beak sign on barium swallow study | back 32 achalasia |
front 33 A 45-year-old man presents after repeated episodes of forceful
vomiting with hematemesis. He is hemodynamically stable, and the
bleeding stops spontaneously. Which of the following best describes
the underlying lesion? | back 33 B. Linear mucosal tear at the gastroesophageal junction mallory-weiss |
front 34 A patient presents with chest pain and subcutaneous emphysema after
severe vomiting. Imaging reveals pneumomediastinum. Which of the
following best describes the underlying lesion? | back 34 A. Transmural rupture of the distal esophagus Boerhaave syndrome |
front 35 A patient presents with hematemesis following excessive alcohol
intake and vomiting. The bleeding is bright red and resolves without
intervention. Which diagnosis is most likely? | back 35 C. Mallory-Weiss tear |
front 36 delete | back 36 delete |
front 37 What is management of tracheoesophageal fistula? | back 37 surgery |
front 38 Baby is born with respiratory distress and excess drooling _____ _____ | back 38 TE fistula |
front 39 GERD: Reflux of acid from the stomach due to ____ ____ in the ____ esophageal sphincter | back 39 reduced tone lower |
front 40 A newborn presents with excessive drooling, choking during
feeds, and inability to pass a nasogastric tube into the
stomach. Imaging reveals air in the stomach and intestines.
Which of the following is the most likely anatomical
abnormality? | back 40 C. Proximal esophageal atresia with distal tracheoesophageal fistula |
front 41 A 58-year-old man with a long history of GERD presents with worsening
reflux symptoms and intermittent dysphagia. A hiatal hernia is
suspected. What is the most appropriate initial diagnostic test? | back 41 C. Barium swallow study |
front 42 A patient with chronic GERD is found to have a hiatal hernia on
imaging. After initial evaluation, which test is most appropriate to
assess for complications such as Barrett esophagus? | back 42 C. Upper endoscopy (EGD) |
front 43 Gastroesophageal reflux disease (GERD) may damage the ____ of teeth | back 43 enamel |
front 44 Gastroesophageal reflux disease (GERD) may present with chronic cough and adult-onset _____ | back 44 asthma |
front 45 Gastroesophageal reflux disease (GERD) often presents with _____, which can mimic cardiac chest pain | back 45 heartburn |
front 46 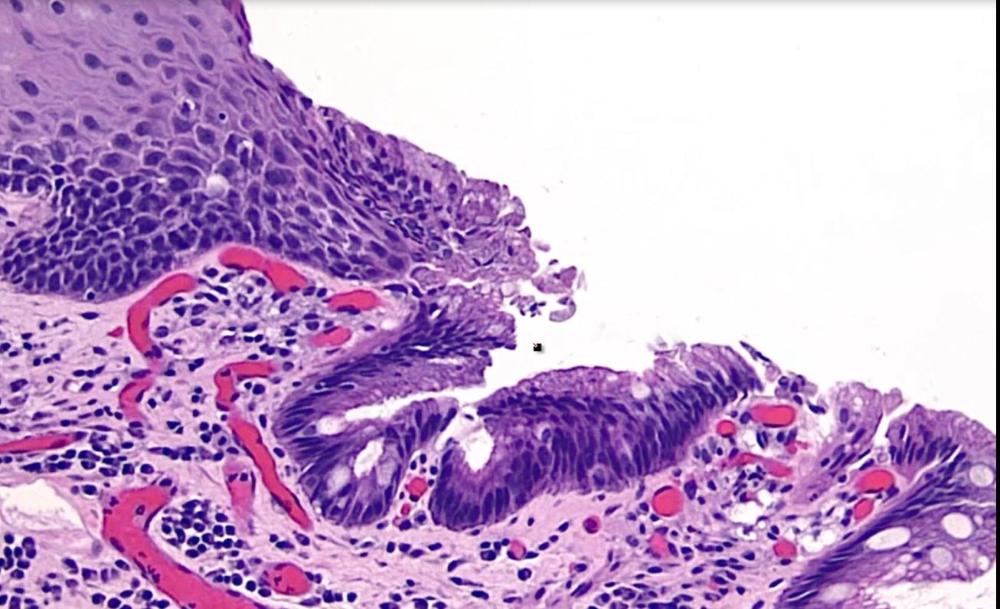 what is this? | back 46 barrett's esophagus |
front 47 A huge risk factor for esophageal adenocarcinoma involves ____ ____ | back 47 barrett's esophagus |
front 48 _____ of the esophagus is a malignant proliferation of glands | back 48 adenocarcinoma |
front 49 acidic damage to stomach mucosa: ____ gastristis | back 49 acute gastristis |
front 50 Dysphagia, Iron Deficiency Anemia, and Esophageal webs are the triad characteristic of which syndrome? | back 50 Plummer-Vinson Syndrome (Plumbers DIE) |
front 51 Neonate with extra-abdominal intestines; to the
right of the umbilicus and not
contained in a membrane? | back 51 B. Gastroschisis |
front 52 A newborn has a midline defect with organs in a sac. What embryologic
failure occurred? | back 52 A. Failure of lateral fold fusion omphalocele |
front 53 often presents with a palpable olive -like mass in the epigastric region of the abdomen | back 53 pyloric stenosis |
front 54 is a congenital hypertrophy of the pyloric smooth muscle | back 54 pyloric stenosis |
front 55 Which antibiotic used in infants is associated with hypertrophic pyloric stenosis? | back 55 Erythromycin |
front 56 A 3-week-old infant presents with progressive, forceful
vomiting after feeds. The vomitus is
nonbilious, and the parents report increased hunger
after episodes. On exam, visible peristaltic waves
are noted across the abdomen. Which of the following additional
findings is most likely on physical examination? | back 56 B. Palpable olive-like mass in epigastrium this is pyloric stenosis |
front 57 A patient is diagnosed with gastric cancer
characterized by diffuse infiltration of the stomach
wall and desmoplastic reaction causing linitis
plastica. Which of the following risk factor profiles is most
consistent with this condition? | back 57 D. No association with Helicobacter pylori infection diffuse gastritis |
front 58 acidic damage to stomach mucosa | back 58 acute gastristis |
front 59 chronic inflammation of stomach mucosa that leads to intestinal metaplasia | back 59 chronic gastristis |
front 60 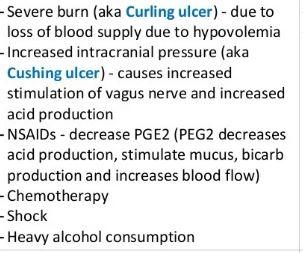 chronic or acute gastritis etiologies? | back 60 acute gastritis |
front 61 A 58-year-old woman has fatigue and
glossitis. Labs show macrocytic
anemia and elevated gastrin. Endoscopy shows
fundic mucosal atrophy. Which mechanism best
explains her condition? | back 61 A. T-cell destruction of parietal cells this is chronic autoimmune gastritis |
front 62 A 49-year-old man has chronic epigastric pain. Gastric biopsy shows
intestinal metaplasia in the
antrum. Urea breath test is
positive. What cancer risk is most increased? | back 62 B. Intestinal-type gastric adenocarcinoma this is chronic h pylori gastritis |
front 63 A patient with chronic gastritis is found to have achlorhydria, high
gastrin, and anti–intrinsic factor antibodies. Which additional
finding is most likely? | back 63 B. Megaloblastic anemia from B12 deficiency |
front 64 A 45-year-old man has recurrent dyspepsia and a positive stool
antigen test. Gastric biopsy shows chronic inflammation involving the
antrum. Which treatment is most appropriate? | back 64 C. PPI plus clarithromycin and amoxicillin this is chronic h pylori gastritis |
front 65 A patient has chronic gastritis with biopsy showing intestinal
metaplasia. Which additional finding would most strongly favor
autoimmune gastritis over chronic H pylori gastritis? | back 65 D. Anti-parietal cell antibodies |
front 66 MALT lymphoma risk, what type of gastritis? | back 66 chronic h pylori gastritis |
front 67 A 32-year-old man has recurrent epigastric pain that
improves shortly after meals. Endoscopy shows an
ulcer in the proximal duodenum. Which cause is most
likely? | back 67 A. Helicobacter pylori infection duodenal ulcer |
front 68 A 61-year-old woman has epigastric pain that becomes worse
with meals. Endoscopy shows an ulcer along the
lesser curvature of the stomach. Which factor most
likely caused this ulcer? | back 68 C. Long-term NSAID use gastric ulcer- remember that this one becomes worse with meals |
front 69 What ulcer? diagnostic endoscopic biopsy shows ulcer with hypertrophy of Brunner glands! | back 69 duodenal ulcer |
front 70 A patient with a posterior duodenal ulcer suddenly
develops hematemesis and signs of
shock. Which structure was most likely eroded? | back 70 C. Gastroduodenal artery |
front 71 A patient is diagnosed with a gastric ulcer. Which feature most
strongly distinguishes it from a typical duodenal ulcer? | back 71 C. Higher malignant potential |
front 72 duodenal ulcer is more present in anterior or posterior? | back 72 anterior |
front 73 which ulcer is more likely to cause pancreatitis? | back 73 duodenal |
front 74 A 64-year-old man presents with weight loss and early
satiety. Endoscopy reveals a large, irregular gastric
ulcer with heaped-up margins along the
lesser curvature of the antrum. Which type of
gastric carcinoma is most likely? | back 74 B. Intestinal-type carcinoma forming glandular structures |
front 75 A patient is diagnosed with gastric adenocarcinoma located along the
lesser curvature of the antrum. Which of the following risk factors is
most strongly associated with this subtype? | back 75 B. Intestinal metaplasia and nitrosamine exposure |
front 76 A 55-year-old patient presents with early satiety and weight loss.
Endoscopy shows a diffusely thickened, rigid stomach
wall without a discrete mass. Biopsy reveals
malignant cells with mucin pushing the nucleus to the periphery. What
is the most likely diagnosis? | back 76 B. Diffuse-type gastric carcinoma with signet ring cells this is diffuse type of gastric carcinoma |
front 77 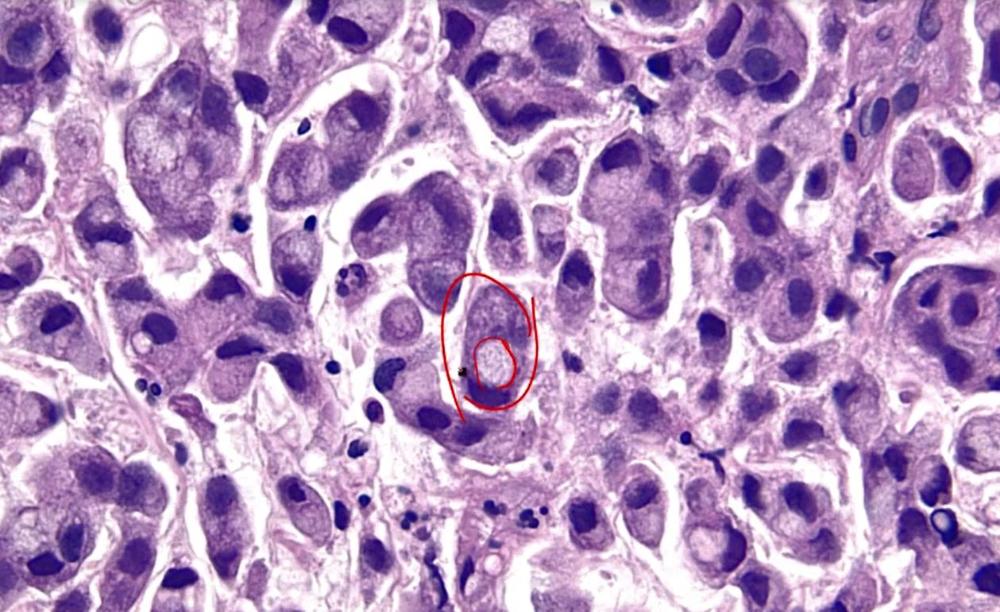 what is this? | back 77 signet ring cell |
front 78 A patient is diagnosed with gastric cancer
characterized by diffuse infiltration of the stomach
wall and desmoplastic reaction causing linitis
plastica. Which of the following risk factor profiles is most
consistent with this condition? | back 78 D. No association with Helicobacter pylori infection |
front 79 _____ carcinoma presents late with weight loss, abdominal pain, anemia, _____ satiety | back 79 gastric early |
front 80 gastric carcinoma can spread to lymph nodes, such as the _____ supraclavicular node (_____ node) | back 80 left supraclavicular node (Virchow node) |
front 81 Which type of gastric carcinoma is associated with a Sister Mary Joseph nodule? Kruckenburg? Intestinal or Diffuse | back 81 Intestinal Diffuse |
front 82  | back 82 duodenal atresia |
front 83  | back 83 duodenal atresia |
front 84  | back 84 meckel diverticulum |
front 85 Meckel diverticulum most commonly occurs in the: | back 85 D. Ileum |
front 86 The most common site of acquired diverticula (Pseudodiverticula) is
the: | back 86 D. Sigmoid colon |
front 87 Congenital hypertrophic pyloric stenosis is more common in: | back 87 A. Males |
front 88 Which syndrome increases risk of hypertrophic pyloric
stenosis? | back 88 A. Marfan syndrome |
front 89 Which trisomy is linked to hypertrophic pyloric stenosis? | back 89 C. Trisomy 18 |
front 90 Which antibiotic exposure in the first 2 weeks increases pyloric
stenosis risk? | back 90 B. Azithromycin |
front 91 Another antibiotic linked to pyloric stenosis risk is: | back 91 A. Erythromycin |
front 92 intussusception: _____ of the bowel | back 92 telescoping |
front 93 A 2-year-old child develops episodic abdominal pain and vomiting. Imaging suggests that one bowel segment has invaginated into the immediately distal segment after a wave of peristalsis. Which diagnosis is most likely? A. Volvulus | back 93 B. Intussusception |
front 94 A 70-year-old patient presents with acute abdominal distention, obstipation, severe pain, and signs of bowel ischemia. Imaging suggests twisting of bowel around its mesenteric attachment. Which diagnosis is most likely? A. Intussusception | back 94 B. Volvulus |
front 95 The pathophysiology of volvulus most directly causes: A. Secretory and osmotic loss | back 95 C. Luminal and vascular compromise |
front 96  | back 96 volvulus |
front 97 Once the bowel segment becomes trapped in intussusception, ongoing peristalsis typically causes it to: A. Retract spontaneously | back 97 B. Pull mesentery along |
front 98  | back 98 intussusception |
front 99 A pathology specimen shows necrosis limited to the mucosa and not extending beyond the muscularis mucosae. This is best classified as: A. Mural infarction | back 99 C. Mucosal infarction |
front 100 Infarction involving the mucosa and submucosa is best termed: A. Mural infarction | back 100 A. Mural infarction |
front 101 Necrosis involving all layers of the intestinal wall, from the mucosa to the serosa. A. Mucosal infarction | back 101 C. Transmural infarction |
front 102 If untreated, intussusception may progress to: A. Fistula and pseudomembranes | back 102 C. Obstruction, vessel compression, infarction |
front 103 Lactose intolerance is caused by decreased function of the _____ enzyme found in brush border enterocytes | back 103 lactase |
front 104  | back 104 celiac disease |
front 105  | back 105 celiac disease |
front 106 A 28-year-old man presents with chronic diarrhea, weight
loss, and fatigue. He also reports an intensely
pruritic, blistering rash on his elbows and knees.
Skin biopsy shows granular IgA deposition at the
tips of dermal papillae. Which of the following is
the most likely associated condition? | back 106 B. Dermatitis herpetiformis associated with celiac disease |
front 107  | back 107 celiac disease |
front 108 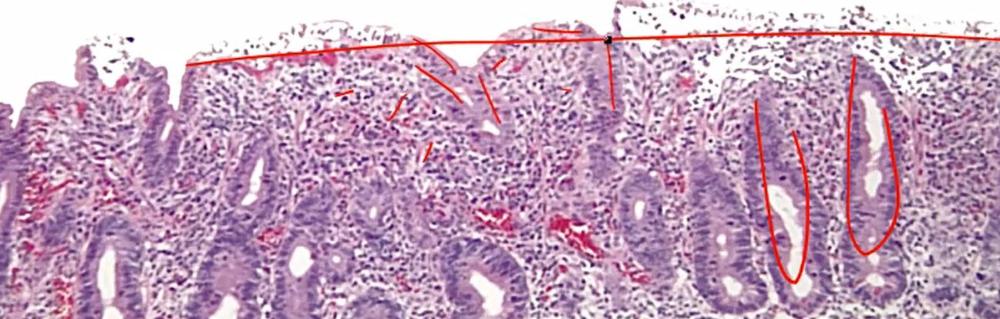 | back 108 celiac disease |
front 109 A 24-year-old woman develops chronic diarrhea, bloating, and weight loss after eating wheat-containing foods. Small-bowel biopsy suggests immune-mediated enteropathy. Which diagnosis is most likely? A. Environmental enteropathy | back 109 B. Celiac disease |
front 110 In celiac disease, gliadin peptides presented by HLA-DQ2/DQ8 primarily activate which immune cell? A. CD8+ T cells | back 110 C. CD4+ T cells |
front 111 Celiac disease most commonly involves which regions of the GI tract? A. Duodenum and jejunum | back 111 A. Duodenum and jejunum |
front 112 The malabsorption in celiac disease is most directly caused by: A. Pancreatic enzyme deficiency | back 112 D. Loss of brush border |
front 113 The most sensitive serologic test for celiac disease is measurement of IgA antibodies against: A. Endomysium | back 113 B. Tissue transglutaminase |
front 114 The most common malignancy associated with celiac disease is: A. Colonic adenocarcinoma | back 114 C. Enteropathy-associated T-cell lymphoma |
front 115  | back 115 tropical sprue |
front 116 A 35-year-old man returns from the Caribbean with chronic
diarrhea, weight loss, and fatigue following an episode of
infectious gastroenteritis. Biopsy shows mucosal
damage predominantly in the jejunum and ileum. Which
of the following is the most likely diagnosis? | back 116 B. Tropical sprue responding to antibiotics |
front 117 A 52-year-old man presents with chronic diarrhea, weight
loss, and bulky, foul-smelling stools. He also reports
migratory joint pain. Small-bowel biopsy shows foamy
macrophages in the lamina propria that stain positive with
periodic acid–Schiff. Which of the following best
explains his steatorrhea? | back 117 A. Macrophages compress lacteals and impair chylomicron transport whipple disease |
front 118 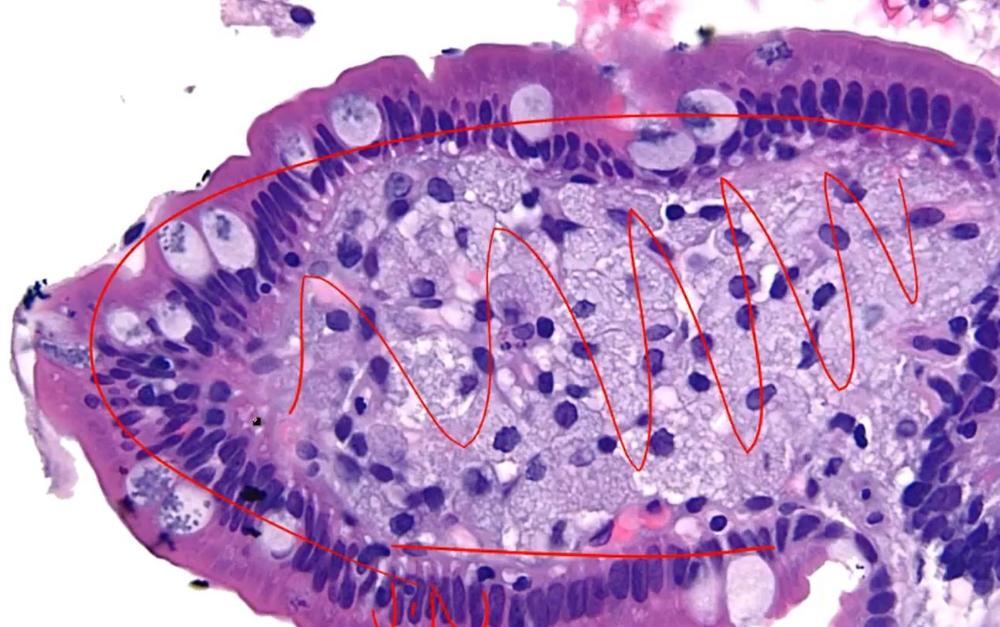 | back 118 foamy macrophages |
front 119 A patient with chronic malabsorption is found to
have PAS-positive foamy macrophages in the lamina
propria of the small intestine. Which infectious organism is most
likely responsible for this finding? | back 119 A. Tropheryma whipplei within macrophage lysosomes |
front 120 A 6-month-old infant presents with failure to thrive, chronic
diarrhea, and steatorrhea. Laboratory studies show extremely low
levels of LDL and VLDL. Which of the following is the most likely
underlying defect? | back 120 A. Impaired synthesis of apolipoprotein B-48 and B-100 apolipoproteinemia |
front 121 A child is diagnosed with a genetic disorder causing fat
malabsorption due to defective chylomicron
formation. Which of the following mechanisms best explains
this finding? | back 121 A. Lack of apolipoprotein B prevents chylomicron assembly apolipoproteinemia |
front 122 A patient with abetalipoproteinemia is found to have absent
circulating LDL and VLDL particles. Which of the following best
explains this laboratory finding? | back 122 A. Failure of apolipoprotein B-100 production in liver |
front 123 A peripheral smear in a patient with abetalipoproteinemia would most likely show: A. Schistocytes | back 123 B. Acanthocytes |
front 124 Abetalipoproteinemia is best described as an inherited inability to: A. Absorb gluten peptides | back 124 D. Secrete triglyceride-rich lipoproteins |
front 125 A 56-year-old patient is found to have a submucosal,
polyp-like lesion in the small intestine during evaluation
for vague abdominal discomfort. Biopsy reveals a low-grade malignant
tumor composed of neuroendocrine cells. Which of the
following is the most likely diagnosis? | back 125 B. Carcinoid tumor from neuroendocrine cell proliferation |
front 126 A patient with a small bowel tumor develops flushing,
diarrhea, and wheezing. Laboratory testing shows elevated
urinary 5-HIAA levels. Why are these symptoms
typically absent in early disease? | back 126 A. Serotonin is degraded by hepatic monoamine oxidase carcinoid tumor |
front 127 A patient with a neuroendocrine tumor of the gut is asymptomatic
until liver metastases develop. Which of the following best explains
the onset of carcinoid syndrome at that stage? | back 127 B. Metastases bypass hepatic metabolism of serotonin carcinoid syndrome |
front 128 A 60-year-old patient with a known small bowel neuroendocrine
tumor develops flushing, diarrhea, and
wheezing. Imaging reveals liver metastases.
What is the most likely explanation for the onset of these
symptoms? | back 128 B. Serotonin release bypasses hepatic metabolism via metastases carcinoid syndrome |
front 129 Gastric carcinoid tumors may be associated with autoimmune
chronic: | back 129 D. viral gastritis |
front 130 A syndrome associated with gastric neuroendocrine tumors is: | back 130 B. Zollinger-Ellison syndrome |
front 131 Neuroendocrine tumors within the stomach and duodenum ______ metastasize and are generally cured by resection. | back 131 rarely |
front 132 Neuroendocrine tumors that arise in the ____ and ____ are often multiple and tend to be aggressive. | back 132 jejunum, ileum |
front 133 Rectal neuroendocrine tumors tend to produce: | back 133 C. polypeptide hormones |
front 134 Symptomatic rectal neuroendocrine tumors may present with: | back 134 A. abdominal pain and weight loss |
front 135  | back 135 Hirschsprung disease |
front 136 In Hirschsprung disease, which segment is always involved? | back 136 D. rectum |
front 137 Hirschsprung disease is also called: | back 137 C. Congenital aganglionic megacolon |
front 138 Hirschsprung disease results from abnormal migration or loss
of: | back 138 B. Neural crest-derived ganglion cells |
front 139 Definitive diagnosis of Hirschsprung disease requires absence
of: | back 139 C. Ganglion cells |
front 140 Ganglion cells in Hirschsprung evaluation may be identified using
stains for: | back 140 B. Acetylcholinesterase |
front 141 A large Zenker diverticulum commonly causes: | back 141 A. Regurgitation and halitosis |
front 142 Nutcracker esophagus reflects loss of coordination between
the: | back 142 B. Circular and longitudinal muscle |
front 143 Nutcracker esophagus is characterized by: | back 143 C. High-amplitude distal contractions |
front 144 A newborn fails to pass meconium within the first 48
hours and develops abdominal distension. Rectal
biopsy shows absence of ganglion cells in the distal
colon. Which of the following is the most appropriate
definitive treatment? | back 144 A. Resection of aganglionic bowel segment Hirschsprung |
front 145  | back 145 colonic diverticula |
front 146 outpounchings of mucosa and submucosa through muscularis propria: ______ diverticula | back 146 colonic |
front 147 A 68-year-old man with chronic constipation presents
with left lower quadrant pain and fever. CT scan shows
inflamed outpouchings in the sigmoid
colon. What is the underlying structural abnormality? | back 147 A. Herniation of mucosa through muscularis propria |
front 148 An elderly patient presents with painless
hematochezia. Colonoscopy reveals multiple
diverticula in the sigmoid colon. Which anatomic feature
explains where these lesions most commonly form? | back 148 B. Sites where vasa recta penetrate bowel wall |
front 149 A patient develops a fistula connecting the
colon to the bladder. What is the
most likely preceding condition? | back 149 C. Diverticulitis with localized inflammation |
front 150 Which of the following best distinguishes colonic diverticulosis from
a true diverticulum such as Meckel diverticulum? | back 150 D. Only mucosa and submucosa herniate |
front 151 A 72-year-old patient has long-standing constipation and is diagnosed
with colonic diverticulosis. Which factor most
contributed to the development of this condition? | back 151 B. Increased intraluminal pressure from straining |
front 152 An older adult presents with intermittent lower GI bleeding. Colonoscopy shows malformed mucosal and submucosal vessels in the cecum. Which diagnosis best fits? A. Volvulus | back 152 Angiodysplasia |
front 153  | back 153 Angiodysplasia |
front 154 A 34-year-old woman presents with recurrent nosebleeds and
episodes of gastrointestinal bleeding. Physical exam reveals
multiple small red lesions on the lips and oral
mucosa. Which of the following is the most likely underlying
condition? | back 154 A. Autosomal dominant disorder causing fragile blood vessels hereditary hemorrhagic telangiectasia |
front 155 A patient with hereditary hemorrhagic telangiectasia
develops chronic iron deficiency anemia. Which of the
following best explains the source of bleeding? | back 155 B. Rupture of thin-walled mucosal blood vessels |
front 156 A 40-year-old man has a history of recurrent
epistaxis and visible telangiectasias on his
tongue. Which inheritance pattern is most consistent with this
condition? | back 156 C. Autosomal dominant with vascular malformations |
front 157 A 72-year-old man with a history of atherosclerosis
presents with sudden left lower quadrant abdominal
pain followed by bloody diarrhea. Which area
of the colon is most likely affected? | back 157 C. Splenic flexure watershed region ischemic colitis |
front 158 A patient with severe atherosclerosis develops
postprandial abdominal pain and weight loss. Which
mechanism best explains progression to ischemic colitis? | back 158 A. Reduced blood flow through superior mesenteric artery ischemic colitis |
front 159 A hospitalized patient develops acute abdominal pain and later passes
bloody stools. Imaging suggests colonic ischemia. Which sequence best
explains this presentation? | back 159 B. Ischemia progresses to infarction causing bleeding ischemic colitis |
front 160 A 35-year-old woman presents with recurrent
abdominal pain, bloating, and alternating diarrhea and
constipation. She notes that her pain improves after
bowel movements. Which of the following is the most likely
diagnosis? | back 160 A. Irritable bowel syndrome with functional bowel disorder |
front 161 A patient reports chronic abdominal discomfort associated
with changes in bowel habits. Extensive workup including
colonoscopy is normal. Which feature most strongly supports
irritable bowel syndrome? | back 161 A. Pain improves after defecation |
front 162 A 60-year-old patient undergoes routine colonoscopy, which reveals
multiple small polyps in the rectosigmoid
colon. Biopsy shows serrated architecture with
hyperplasia of glands but no dysplasia. What is the most
likely diagnosis? | back 162 A. Hyperplastic polyp |
front 163 A patient is found to have a colonic polyp with serrated
histologic appearance and polyclonal glandular
hyperplasia. Which of the following best describes its
malignant potential? | back 163 C. No risk of malignant transformation |
front 164 Which of the following features most strongly supports a diagnosis of
hyperplastic polyp rather than an
adenomatous polyp? | back 164 B. Serrated glands without cytologic atypia |
front 165 A 58-year-old patient undergoes colonoscopy and is found to have a
polyp. Biopsy reveals monoclonal proliferation of
dysplastic glandular epithelium. Which of the
following is the most likely diagnosis? | back 165 B. Adenomatous polyp with neoplastic gland prolifera |
front 166 A patient is diagnosed with a colonic polyp that is benign but has
potential to progress to malignancy. Which pathway best describes this
progression? | back 166 B. Adenoma to carcinoma sequence |
front 167 Which dietary pattern most promotes progression of diverticular disease? A. High-protein diet | back 167 D. Low-fiber diet |
front 168 Which statement about diverticular disease is most accurate? A. Usually presents with obstruction | back 168 B. Most patients are asymptomatic |
front 169 The pathogenesis of diverticular disease is most closely related to: A. Elevated intraluminal pressure | back 169 A. Elevated intraluminal pressure |
front 170 Colorectal adenocarcinoma develops in ____% of untreated FAP patients | back 170 100 |
front 171 Which finding is required for diagnosis of classic familial adenomatous polyposis? A. At least 10 polyps | back 171 D. At least 100 polyps |
front 172 Familial adenomatous polyposis is best described as which syndrome? A. APC-associated adenomatous polyposis | back 172 A. APC-associated adenomatous polyposis |
front 173 The standard preventive treatment for classic familial adenomatous polyposis is: A. Annual polypectomy | back 173 C. Prophylactic colectomy |
front 174 After colectomy for FAP, which medication class can reduce polyps in the residual rectum? A. NSAIDs | back 174 A. NSAIDs |
front 175 A 3-year-old child presents with painless rectal
bleeding. Parents report a small mass that
occasionally protrudes from the rectum during defecation.
Which of the following is the most likely diagnosis? | back 175 A. Juvenile polyp with benign hamartomatous growth |
front 176 A 16-year-old girl presents with multiple dark pigmented
spots on her lips and oral mucosa. She has a history of
recurrent abdominal pain, and imaging reveals
multiple polyps throughout the gastrointestinal
tract. Which of the following is the most likely diagnosis? | back 176 A. Peutz-Jeghers syndrome with hamartomatous polyps |
front 177 A 4-year-old child presents with intermittent painless rectal bleeding. Colonoscopy reveals a solitary rectal polyp composed of disorganized but mature tissue elements. Which diagnosis is most likely? A. Hyperplastic polyp | back 177 C. Juvenile polyp |
front 178 Juvenile polyps are best classified as: A. Hamartomatous polyps | back 178 A. Hamartomatous polyps |
front 179 Which presentation is most typical of a juvenile polyp? A. Watery secretory diarrhea | back 179 D. Rectal bleeding |
front 180 A child has multiple hamartomatous colorectal polyps and a family history of similar lesions. Which syndrome should raise concern for future colonic adenocarcinoma? A. Lynch syndrome | back 180 C. Juvenile polyposis syndrome |
front 181 Juvenile polyposis syndrome is often associated with mutation in: A. SMAD4 | back 181 A. SMAD4 |
front 182 The major long-term malignancy risk in juvenile polyposis syndrome is: A. Gastric lymphoma | back 182 D. Colonic adenocarcinoma |
front 183 In Peutz-Jeghers syndrome, hamartomatous polyps most often involve the: A. Small intestine | back 183 A. Small intestine |
front 184 Which gene is characteristically mutated in Peutz-Jeghers syndrome? A. SMAD4 | back 184 C. STK11 |
front 185 A 10-year-old boy presents with acute abdominal pain
that began periumbilically and migrated to the right lower
quadrant. Imaging confirms appendicitis.
Which of the following is the most likely underlying cause in this
patient? | back 185 A. Lymphoid hyperplasia causing luminal obstruction |
front 186 A 35-year-old man presents with right lower quadrant
abdominal pain, fever, and leukocytosis. Which of the
following mechanisms most likely initiated this condition? | back 186 A. Obstruction by fecalith leading to bacterial overgrowth appendicitis |
front 187 A 29-year-old patient has chronic abdominal pain and diarrhea. Endoscopy shows inflamed bowel separated by normal intervening mucosa. Which diagnosis is most likely? A. Ulcerative colitis | back 187 C. Crohn disease |
front 188 Which feature best distinguishes Crohn disease from ulcerative colitis? A. Transmural inflammation | back 188 A. Transmural inflammation |
front 189 A patient with inflammatory bowel disease develops enteroenteric fistulas and bowel wall fibrosis. Which diagnosis best fits? A. Ulcerative colitis | back 189 D. Crohn disease |
front 190 Which distribution is most typical of ulcerative colitis? A. Any GI segment | back 190 B. Colon and rectum |
front 191 Histology from an inflamed bowel segment shows noncaseating granulomas and transmural inflammation. Which disorder is most likely? A. Crohn disease | back 191 A. Crohn disease |
front 192 A patient with longstanding inflammatory bowel disease develops severe colonic dilation and systemic toxicity. Which disease is classically associated with this complication? A. Crohn disease | back 192 D. Ulcerative colitis |
front 193 Which gross feature is classically associated with Crohn disease? A. Continuous rectosigmoid disease | back 193 C. Creeping fat |
front 194 Ulcerative colitis is typically confined to which bowel layers? A. Muscularis and serosa | back 194 B. Mucosa and superficial submucosa |
front 195 A patient with Crohn disease develops recurrent obstructive symptoms from fibrosing bowel narrowing. Which treatment is often required? A. Surgical resection | back 195 A. Surgical resection |
front 196 A patient with severe ulcerative colitis undergoes total colectomy. What is the expected effect on the intestinal disease? A. Disease shifts to ileum | back 196 D. Intestinal disease is cured |
front 197 A 29-year-old man with chronic inflammatory bowel disease presents
with fatigue and pruritus. Laboratory testing reveals a
cholestatic pattern, and imaging shows
multifocal stricturing of the bile ducts. Which of
the following associated conditions is most likely present? | back 197 A. Primary sclerosing cholangitis with p-ANCA positivity this is UC |
front 198  what is this associated with? | back 198 crohn's |
front 199 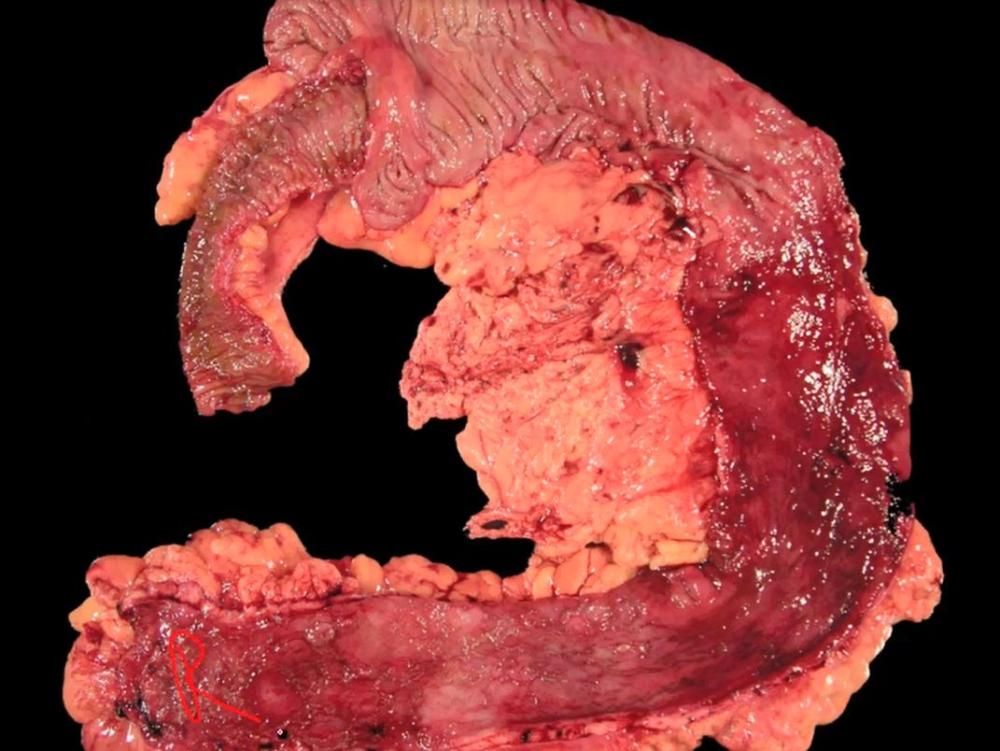 UC or Crohns? | back 199 UC |
front 200 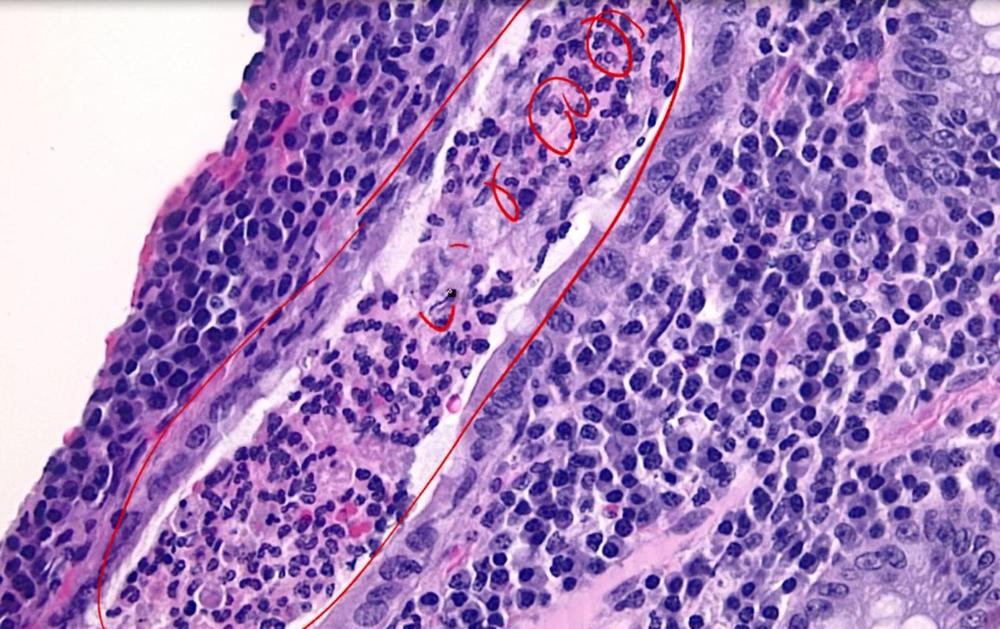 UC or Crohns? | back 200 UC crypt abcess, neutrophils |
front 201 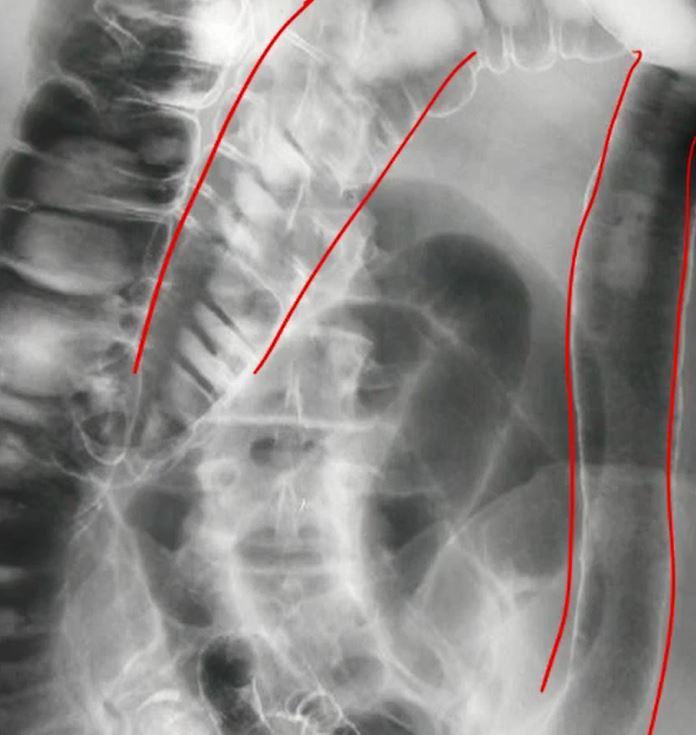 what is happening here? | back 201 lead pipe sign- loss of haustra, UC |
front 202 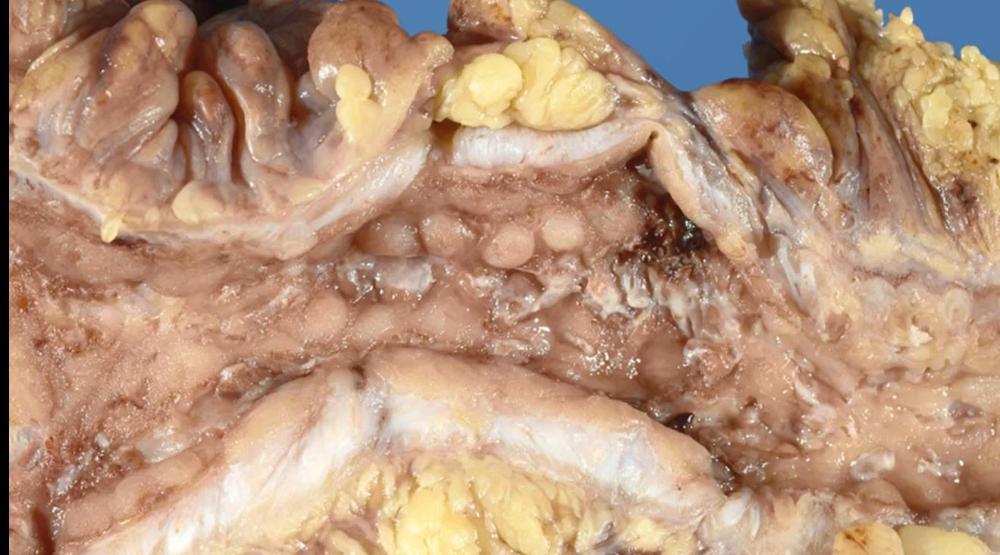 UC or Crohns? | back 202 Crohns |
front 203 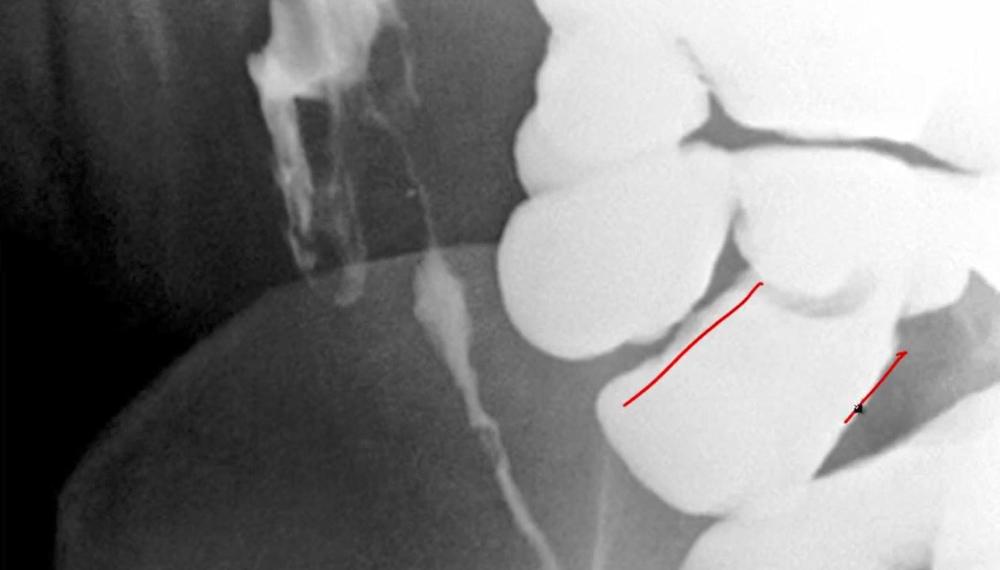 UC or Crohns? | back 203 Crohns string sign |
front 204 A neonate with polyhydramnios has excessive salivation, choking with feeds, and failure to pass an NG tube. Esophageal atresia most commonly occurs near which anatomic level? A. Upper esophageal sphincter | back 204 B. Tracheal bifurcation |
front 205 Prenatal imaging shows abdominal viscera in the thorax. After delivery, the infant develops severe respiratory distress. Which paired finding is most characteristic of congenital diaphragmatic hernia? A. Right-sided defect; pulmonary hypoplasia | back 205 D. Left-sided defect; pulmonary hypoplasia |
front 206 A newborn has a midline abdominal wall defect covered by a membranous sac. Which genetic association is classically linked to this lesion? A. Down syndrome | back 206 A. Down syndrome |
front 207 Endoscopy identifies an “inlet patch” of ectopic gastric mucosa in the esophagus. Where is this finding most commonly located? A. Distal third | back 207 C. Upper third |
front 208 A child presents with painless lower GI bleeding from a congenital true diverticulum containing ectopic tissue. This lesion most commonly arises in the: A. Ileum | back 208 A. Ileum The clinical presentation describes a Meckel's diverticulum |
front 209 Meckel diverticulum results from failure of involution of a structure that normally connects the: A. Foregut to allantois | back 209 C. Developing gut to yolk sac |
front 210 A neonate with abdominal distention and empty rectum is suspected of having Hirschsprung disease. Which gene is most classically implicated by loss-of-function mutation? A. APC | back 210 D. RET |
front 211 What is the earliest classic postnatal clue to Hirschsprung disease? A. Bilious emesis | back 211 B. Failure to pass meconium |
front 212 A patient with intermittent chest pain and dysphagia has a barium swallow showing a corkscrew esophagus. Which manometric feature best fits this disorder? A. Normal amplitude contractions | back 212 A. Normal amplitude contractions |
front 213 A patient has recurrent chest pain with hypertensive but coordinated peristaltic waves on manometry. Which description would argue against nutcracker esophagus? A. Low-amplitude coordinated waves | back 213 C. High-amplitude uncoordinated waves |
front 214 In Plummer-Vinson syndrome, esophageal webs classically occur with glossitis, cheilosis, and: A. Hemolytic anemia | back 214 B. Iron deficiency anemia |
front 215 A patient with dysphagia to solids and liquids has incomplete lower esophageal sphincter relaxation. Which additional pair completes the classic achalasia triad? A. Increased tone with aperistalsis | back 215 A. Increased tone with aperistalsis |
front 216 After repeated retching, a patient develops hematemesis. Endoscopy shows longitudinal mucosal lacerations near the gastroesophageal junction. These lesions are called: A. Boerhaave rupture | back 216 B. Mallory-Weiss tears |
front 217 Which precipitating event most classically causes Mallory-Weiss tears? A. Portal venous congestion | back 217 D. Repetitive forceful vomiting |
front 218 Candidiasis of the esophagus is characterized by: A. Linear mucosal furrows | back 218 C. Gray-white pseudomembranes |
front 219 Which mechanism is a major driver of GERD pathogenesis? A. Transient LES relaxation | back 219 A. Transient LES relaxation |
front 220 Biopsy of distal esophageal mucosa in chronic reflux disease most classically shows: A. Goblet cell metaplasia | back 220 B. Basal zone hyperplasia |
front 221 A patient with chronic heartburn and acid regurgitation has uncomplicated GERD. Which drug class is standard therapy? A. Sucralfate | back 221 D. Proton pump inhibitors |
front 222 A young adult with asthma and multiple food allergies has recurrent solid-food dysphagia. Which underlying process best fits eosinophilic esophagitis? A. Atopic disease | back 222 A. Atopic disease |
front 223 A cirrhotic patient presents with massive hematemesis from dilated submucosal veins in the distal esophagus. The most likely underlying cause is: A. Diffuse esophageal spasm | back 223 C. Portal hypertension |
front 224 Barrett esophagus represents which metaplastic transition? A. Columnar to squamous | back 224 D. Squamous to columnar |
front 225 Which cell type is required for the diagnosis of Barrett esophagus? A. Paneth cells | back 225 B. Goblet cells |
front 226 Which epidemiologic pattern for esophageal cancer is correct? A. West squamous, world adenocarcinoma | back 226 C. West adenocarcinoma, world squamous |
front 227 Which condition is a major risk factor for esophageal adenocarcinoma? A. Barrett esophagus | back 227 A. Barrett esophagus |
front 228 Esophageal adenocarcinoma most often arises in which location? A. Proximal third | back 228 B. Distal third |
front 229 Which exposure pattern is most strongly associated with esophageal squamous cell carcinoma? A. Chronic iron deficiency | back 229 D. Alcohol and tobacco |
front 230 Which esophageal malignancy is more likely to spread to lymph nodes and carry a poorer prognosis? A. Esophageal squamous carcinoma | back 230 A. Esophageal squamous carcinoma |
front 231 Acute gastritis is defined histologically by the presence of: A. Neutrophils | back 231 A. Neutrophils |
front 232 chronic use of what can cause gastritis by inhibiting production of vasodilation products? | back 232 NSAIDs |
front 233 A critically ill patient with extensive full-thickness burns develops hematemesis several days after admission. Which ulcer type is most classically associated with this setting? A. Cushing ulcer | back 233 C. Curling ulcer |
front 234 Ulcers occurring in the context of intracranial disease is termed: A. Curling ulcer | back 234 B. Cushing ulcer |
front 235 Chronic gastritis worldwide is most commonly caused by: A. Autoimmune injury | back 235 D. Helicobacter pylori |
front 236 H. pylori occurs mostly in which part of the stomach? A. Body | back 236 D. Antrum |
front 237 A urease breath test is positive in a patient with dyspepsia. H. pylori uses urease primarily to generate which compound that promotes survival? A. Nitric oxide | back 237 C. Ammonia |
front 238 Expression of CagA by H. pylori has what effect on gastric cancer risk? A. Eliminates malignant potential | back 238 D. Increases cancer risk |
front 239 A patient with chronic H. pylori gastritis develops dense lymphoid aggregates in the stomach. This infection is a risk factor for formation of: A. GIST | back 239 C. MALT lymphoma |
front 240 Which feature best distinguishes autoimmune gastritis from H. pylori gastritis? A. Antral predominance | back 240 B. Hypergastrinemia with antral sparing |
front 241 Autoimmune gastritis is primarily associated with immune-mediated loss of which gastric cell type? A. Mucous neck cells | back 241 D. Parietal cells |
front 242 A patient with autoimmune atrophic gastritis develops fatigue, glossitis, and macrocytosis. Which associated manifestation is most expected? A. Iron deficiency anemia | back 242 C. Megaloblastic anemia |
front 243 Histology from autoimmune atrophic gastritis most characteristically shows injury involving which anatomic regions? A. Cardia and pylorus | back 243 B. Body and fundus |
front 244 A patient with peripheral eosinophilia and recurrent gastric symptoms has biopsy-proven eosinophilic gastritis. Which mechanism is most likely responsible? A. Allergic reaction | back 244 A. Allergic reaction |
front 245 In Western populations, the most common cause of granulomatous gastritis is: A. Sarcoidosis | back 245 C. Crohn disease |
front 246 Which trio most completely accounts for the great majority of peptic ulcers involving the stomach or duodenum? A. Alcohol, steroids, CMV | back 246 B. H. pylori, NSAIDs, smoking |
front 247 Peptic ulcer disease most commonly affects which gastric location? A. Greater curvature body | back 247 D. Antrum lesser curvature |
front 248 H. pylori infection that predominantly involves the fundus and body is most associated with which physiologic pattern? A. Increased acid without atrophy | back 248 B. Decreased acid with atrophy |
front 249 Which condition carries the greater association with gastric adenocarcinoma? A. Autoimmune atrophic gastritis | back 249 A. Autoimmune atrophic gastritis |
front 250 A patient with giant rugal folds, edema, and protein-losing gastropathy is found to have overexpression of which cytokine? A. Transforming growth factor beta | back 250 C. Transforming growth factor alpha Menetrier disease |
front 251 Menetrier disease is most classically characterized by which pair of findings? A. Parietal hyperplasia and hypercalcemia | back 251 D. Foveolar hyperplasia and hypoproteinemia |
front 252 A patient has severe recurrent peptic ulcers and markedly increased gastrin levels from a pancreatic neuroendocrine tumor. Which gastric cell type is expected to be especially enlarged? A. Parietal cells | back 252 A. Parietal cells |
front 253 Zollinger-Ellison gastrinomas are classically associated with which inherited syndrome? A. MEN2A | back 253 C. MEN1 |
front 254 Fundic gland polyps and intestinal-type gastric adenocarcinoma are both associated with mutations in which gene? A. RB1 | back 254 B. APC |
front 255 Which set best lists classic metastatic sites of gastric adenocarcinoma? A. Cervical spine, liver, spleen, lung | back 255 C. Virchow, umbilical, ovaries, axilla |
front 256 A family with hereditary diffuse gastric cancer is found to carry a germline mutation in which gene? A. MLH1 | back 256 D. CDH1 |
front 257 Which viral infection is implicated in lymphoproliferation and GI lymphoma formation? A. Epstein-Barr virus | back 257 A. Epstein-Barr virus |
front 258 A patient with episodic flushing develops wheezing, secretory diarrhea, and tricuspid dysfunction. Which syndrome best fits this presentation? A. VIPoma syndrome | back 258 C. Carcinoid syndrome |
front 259 Neuroendocrine tumors from which embryologic region tend to be the most aggressive? A. Foregut | back 259 B. Midgut |
front 260 A submucosal GI spindle-cell tumor is found to arise from the gut’s pacemaker cells. What is its cell of origin? A. Smooth muscle cells | back 260 D. Interstitial cells of Cajal |
front 261 About 75% of gastrointestinal stromal tumors harbor gain-of-function mutations in which gene? A. KIT | back 261 A. KIT |
front 262 Worldwide, the most frequent cause of intestinal obstruction is: A. Hernias | back 262 A. Hernias |
front 263 An elderly patient develops sudden abdominal pain, distention, and bowel ischemia after a segment of colon twists around its mesenteric attachment. This process is termed: A. Intussusception | back 263 B. Volvulus |
front 264 A 14-month-old child develops intermittent colicky pain, vomiting, and drawing up of the legs. Which is the most common cause of intestinal obstruction in children younger than 2 years? A. Hirschsprung disease | back 264 C. Intussusception |
front 265 A patient with profound hypotension develops ischemic colitis at a bowel region supplied by the terminal branches of both the SMA and IMA. Which site is this severe watershed zone? A. Cecum | back 265 B. Splenic flexure |
front 266 A premature, low-birth-weight neonate develops abdominal distention, bloody stools, and pneumatosis intestinalis. Which GI emergency best fits? A. Meconium ileus | back 266 D. Necrotizing enterocolitis |
front 267 Which HLA profile is most strongly associated with celiac disease? A. HLA-B27 and DR4 | back 267 B. HLA-DQ2 and DQ8 |
front 268 Autoimmune enteropathy is classically associated with mutations in which gene? A. APC | back 268 B. FOXP3 |
front 269 An infant with intractable secretory diarrhea is diagnosed with microvillus inclusion disease. Which gene is most likely mutated? A. MTP | back 269 C. MYO5B |
front 270 Abetalipoproteinemia is caused by mutation in which protein? A. MTP | back 270 A. MTP |
front 271 A patient with profuse “rice-water” diarrhea is infected by a comma-shaped gram-negative organism. Which pathogen best fits? A. Shigella dysenteriae | back 271 D. Vibrio cholerae |
front 272 Which cholera toxin component is responsible for the downstream activation leading to CFTR-mediated ion and water efflux? A. B subunit | back 272 C. A subunit |
front 273 Based on the material provided, the most common bacterial cause of traveler’s diarrhea and food poisoning is: A. Salmonella enteritidis | back 273 B. Campylobacter jejuni |
front 274 A patient develops inflammatory diarrhea after undercooked poultry and later presents with asymmetric arthritis. Which HLA type is associated with this postinfectious complication? A. HLA-B27 | back 274 A. HLA-B27 |
front 275 A patient develops ascending weakness several weeks after diarrheal illness due to Campylobacter jejuni. Which neurologic complication is classically associated? A. Multiple sclerosis | back 275 C. Guillain-Barré syndrome |
front 276 Campylobacter jejuni is best described as which of the following? A. Bacillus, gram-positive | back 276 B. Comma-shaped, gram-negative |
front 277 Which statement about Shigella is correct? A. Gram-positive coccus | back 277 C. Gram-negative organism |
front 278 Shigella organisms are classically taken up by which intestinal cells? A. Goblet cells | back 278 B. M cells |
front 279 A foodborne diarrheal illness is caused by a gram-negative bacillus. Which organism best matches this morphology and classification? A. Vibrio cholerae | back 279 C. Salmonella enteritidis |
front 280 Nontyphoidal salmonellosis is most classically caused by: A. Salmonella typhi | back 280 C. Salmonella enteritidis |
front 281 Which organism is the classic cause of typhoid fever? A. Salmonella typhi | back 281 A. Salmonella typhi |
front 282 Typhoid fever disseminates primarily through: A. Bile and pancreatic ducts | back 282 B. Blood and lymphatics |
front 283 A patient with typhoid fever develops abdominal distention and GI bleeding from inflamed lymphoid tissue in the ileum. Which structure is classically enlarged? A. Brunner glands | back 283 C. Peyer patches |
front 284 Which statement about typhoid fever is most accurate? A. It remains confined to colon | back 284 D. It can cause extraintestinal disease |
front 285 A child with iron overload develops enterocolitis from a pathogen that invades M cells and is enhanced by iron availability. Which organism best fits? A. Yersinia enterocolitica | back 285 A. Yersinia enterocolitica |
front 286 Which extraintestinal manifestation is classically associated with Yersinia infection? A. Hemolytic anemia | back 286 B. Erythema nodosum |
front 287 A patient with Yersinia enterocolitica develops symptoms outside the intestine. Which additional finding is characteristic? A. Hemoptysis | back 287 D. Pharyngitis |
front 288 Another patient with Yersinia infection presents with joint pain several days after enterocolitis. Which extraintestinal manifestation best fits? A. Raynaud phenomenon | back 288 C. Arthralgia |
front 289 Which morphology best describes Escherichia coli? A. Gram-negative bacillus | back 289 A. Gram-negative bacillus |
front 290 A child develops hemorrhagic colitis after eating undercooked beef. Antibiotics are avoided because toxin release may precipitate which complication? A. Reactive arthritis | back 290 C. Hemolytic-uremic syndrome |
front 291 A hospitalized patient develops fever, abdominal cramping, and pseudomembranes after broad-spectrum antibiotic use. Which pathogen is most likely responsible? A. Clostridium difficile | back 291 A. Clostridium difficile |
front 292 Which treatment pair is listed as effective first-line therapy for C. difficile infection? A. Ciprofloxacin and rifaximin | back 292 B. Metronidazole and vancomycin |
front 293 In Whipple disease, malabsorptive diarrhea most directly reflects: A. Crypt cell apoptosis | back 293 D. Impaired lymph drainage |
front 294 Which triad is classic for Whipple disease? A. Diarrhea, weight loss, arthralgia | back 294 A. Diarrhea, weight loss, arthralgia |
front 295 About half of viral gastroenteritis cases are attributed to: A. Rotavirus | back 295 C. Norovirus |
front 296 Which statement about rotavirus is correct? A. It is double-stranded RNA | back 296 A. It is double-stranded RNA |
front 297 Which IBD subtype affects both the ileum and colon? | back 297 Crohns |
front 298 Which IBD subtype presents with a diffuse and continuous distribution? | back 298 UC |
front 299 Which IBD subtype presents with difficulties absorbing fats and vitamins? | back 299 Crohn's |
front 300 Which IBS subtype predominates in the colon only? | back 300 UC |
front 301 Which IBD subtype is described as transmural? | back 301 Crohn's |
front 302 Which IBD subtype is limited to only the mucosa and submucosa? | back 302 UC |
front 303 Which IBD subtype is characterized by skip lesions? | back 303 Crohn's |
front 304 Which IBD disorder is limited to the colon and rectum? | back 304 UC |
front 305 Which IBD subtype leads to an increased risk of toxic megacolon, increasing risk of perforation? | back 305 UC |
front 306 Which type of polyp is most often regarded as genetically determined? A. Adenomatous | back 306 D. Hamartomatous |
front 307 In older adults, decreased epithelial shedding can produce mucosal elevations in the gut known as: A. Fissures | back 307 C. Polyps |
front 308 A patient develops colitis after surgical diversion performed during treatment of Hirschsprung disease. Which diagnosis best fits? A. Diversion colitis | back 308 A. Diversion colitis |
front 309 Which gene is implicated in increased risk of Crohn disease, despite accounting for less than half of total disease risk? A. APC | back 309 D. NOD2 |
front 310 A patient with early-onset right-sided colon cancer has few polyps but a strong family history of similar malignancies. Which syndrome best fits? A. Gardner syndrome | back 310 B. Lynch syndrome |
front 311 Lynch syndrome most classically involves mutations in which gene pair? A. APC and KRAS | back 311 D. MSH2 and MLH1 |
front 312 The defective pathway in Lynch syndrome normally mediates: A. Base excision repair | back 312 C. Mismatch repair |
front 313 Most colorectal adenocarcinomas involve mutation of which gene? A. APC | back 313 A. APC |
front 314 A colorectal carcinoma arises in the setting of DNA mismatch repair deficiency. Which molecular phenomenon is most characteristic? A. Chromothripsis | back 314 B. Microsatellite instability |
front 315 Which two features are most important for prognosis in colorectal cancer? A. Tumor grade and mucin | back 315 D. Depth and nodal spread |
front 316 A patient with anal canal cancer is found to have a viral-associated squamous cell carcinoma. Which pathogen is most strongly linked? A. EBV | back 316 C. HPV |
front 317 Which statement about the appendix is correct? A. It is a true diverticulum | back 317 A. It is a true diverticulum |
front 318 The most common appendiceal tumor is: A. Mucinous adenocarcinoma | back 318 D. Neuroendocrine tumor |
front 319 Tumors arising from the peritoneal lining are called: A. Adenomas | back 319 C. Mesotheliomas |
front 320 Which pair correctly describes Shigella? A. Encapsulated and motile | back 320 C. Unencapsulated and nonmotile |