Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
CE Midterm
front 1 Sunken cheeks, wasting of temporalis muscles, flushing of face indicate ______ ______ | back 1 systemic illness |
front 2 Pale, puffy face = ______ hyperthyroidism Goiter nephritis parkinsonism | back 2 nephritis |
front 3 Startled expression = ______ hyperthyroidism Goiter nephritis parkinsonism | back 3 hyperthyroidism |
front 4 Immobile stare = ______ hyperthyroidism Goiter nephritis parkinsonism | back 4 parkinsonism |
front 5 ______ = enlarged thyroid glands hyperthyroidism Goiter nephritis parkinsonism | back 5 Goiter |
front 6 most common endocrine cancer | back 6 thyroid cancer |
front 7 thyroid cancer seen more in men or women? | back 7 women |
front 8 5-year survival rate all thyroid cancers = ___% | back 8 97 |
front 9 Thryoid Cancer- Decreasing or Increasing # of cases each year? | back 9 Increasing |
front 10 Thryoid cancer: has been ___ death rate in men and ___ in women | back 10 increasing stable |
front 11 ___ and ___ cancer includes cancers of mouth, nose, sinuses, salivary glands, throat, and lymph nodes | back 11 head and neck |
front 12 ___ % of all head and neck cancers linked to tobacco use | back 12 85 |
front 13 Mastoid process - part of ___ (impt in ear disease) | back 13 temporal |
front 14 Mouth principle muscle- ___ ___ it surrounds lips and closes lips | back 14 orbicularis oris |
front 15 Eye principle muscle - ___ ___ (___ eyelid) | back 15 orbicularis oculi closes |
front 16 ___ - thin, superficial muscle of neck, crossing outer | back 16 Platysma |
front 17 Platysma Action- pull mandible ___ and ___ | back 17 downward backwards |
front 18 Which muscle of mastication is described as the strongest and thickest facial muscle responsible for powerful jaw closure? | back 18 Masseter |
front 19 The primary action of the masseter muscle is to: | back 19 B. Elevate and retract mandible |
front 20 A clinician palpates strong tension over the cheek while a patient
clenches their teeth. Which muscle is being assessed? | back 20 C. Masseter |
front 21 Muscles of mastication insert primarily onto which bone to produce chewing movements? | back 21 Mandible |
front 22 Which cranial nerve provides motor innervation to the muscles of
mastication? | back 22 C. Trigeminal nerve (CN V) |
front 23 The trigeminal nerve carries sensory information from which of the
following regions? | back 23 B. Face, oral cavity, and teeth |
front 24 The sternocleidomastoid divides the neck into which two major
anatomical regions? | back 24 C. Anterior and posterior triangles |
front 25 Which muscle elevates the sternum during forced respiration and helps form the boundary between neck triangles? | back 25 SCM |
front 26 The sternocleidomastoid originates from which two structures? | back 26 A. Manubrium and clavicle |
front 27 The insertion of the sternocleidomastoid muscle is located on
the: | back 27 C. Mastoid process |
front 28 Motor innervation of the sternocleidomastoid muscle is primarily
supplied by which cranial nerve? | back 28 B. CN XI |
front 29 The sternocleidomastoid muscle lies superficial to which important
vascular and neural structure bundle? | back 29 B. Carotid sheath |
front 30 Which structure is NOT contained within the carotid sheath? | back 30 D. Phrenic nerve |
front 31 Which boundary helps form the inferior border of the anterior
triangle of the neck? | back 31 A. Clavicle |
front 32 Which of the following structures is located within the anterior
triangle of the neck? | back 32 B. Thyroid gland |
front 33 Which gland found in the anterior triangle contributes to saliva
production? | back 33 C. Submandibular gland |
front 34 Which organ within the anterior triangle is directly involved in voice production? | back 34 Larynx |
front 35 Enlargement of which structures in the anterior triangle most
commonly reflects immune response to infection? | back 35 B. Lymph nodes |
front 36 The thyroid gland consists of two lobes connected by which
structure? | back 36 B. Thyroid isthmus |
front 37 The thyroid gland primarily wraps around which two structures in the
neck? | back 37 B. Larynx and trachea |
front 38 The thyroid isthmus typically lies across the trachea just inferior
to which cartilage? | back 38 C. Cricoid cartilage |
front 39 The primary function of the thyroid gland is to: secrete _____ hormones | back 39 thyroid |
front 40 Which muscles form the posterior boundary of the posterior triangle of the neck? Which structure forms the inferior boundary of the posterior triangle of the neck? | back 40 Trapezius Clavicle |
front 41 A key structure commonly located within the posterior triangle of the
neck is the: | back 41 C. Lymph nodes |
front 42 Approximately how many lymph nodes are typically present on each side
of the neck? | back 42 C. 75 |
front 43 During physical examination, range of motion of the neck is commonly
assessed to evaluate for: | back 43 B. Neck masses or stiffness |
front 44 A painful neck mass most commonly suggests: | back 44 A. Acute infection |
front 45 mass present for months may be _____ | back 45 neoplastic |
front 46 A neck mass present for only a few days most likely indicates: | back 46 A. Inflammation |
front 47 A neck mass present for months to years without change in size is
most consistent with: | back 47 C. Lesion |
front 48 A neck mass that fluctuates in size while eating most likely results
from: | back 48 B. Salivary gland blockage |
front 49 In patients younger than 20 years old, a neck mass is most commonly
due to: | back 49 B. Enlarged tonsillar node or congenital mass |
front 50 A midline neck mass in a young patient most strongly suggests which
condition? | back 50 B. Thyroglossal cyst |
front 51 In patients aged 20–40 years, neck masses are most commonly related
to: | back 51 A. Thyroid disease |
front 52 In patients older than 40 years, a new neck mass should be
considered: | back 52 B. Malignant until proven otherwise |
front 53 A midline neck mass is most commonly associated with: | back 53 B. Congenital or benign lesions |
front 54 A lateral neck mass is most commonly suggestive of: | back 54 C. Neoplastic process |
front 55 Metastatic tumors in the upper neck most commonly originate from
cancers of the: | back 55 B. Head and neck |
front 56 Metastatic tumors in the lower neck most commonly originate from
cancers of the: | back 56 B. Breast and stomach |
front 57 The most common cause of neck stiffness is: | back 57 B. Muscle sprain or strain |
front 58 Neck stiffness caused by muscular injury most commonly involves which
muscle? | back 58 C. Levator scapulae |
front 59 The levator scapulae muscle connects the cervical spine to which
structure? | back 59 B. Shoulders |
front 60 The levator scapulae is primarily located along which region of the
neck? | back 60 B. Back and side of neck |
front 61 The levator scapulae muscle receives motor innervation primarily from which cervical spinal nerves? | back 61 C3–C4 |
front 62 Sudden neck stiffness accompanied by high fever, nausea, vomiting,
and headache should raise concern for: | back 62 B. Meningeal irritation |
front 63 Neck stiffness accompanied by fever should prompt: | back 63 C. Medical evaluation |
front 64 Neck pain may occur as referred pain from which organ system? | back 64 B. Cardiovascular system |
front 65 A patient with angina or myocardial infarction may complain of pain
radiating to which area? | back 65 B. Neck |
front 66 Neck pain associated with myocardial ischemia is best explained
by: | back 66 B. Referred pain |
front 67 The most common psychological reaction to head and neck disease is: | back 67 Depression |
front 68 During inspection of the head and neck, which structure should be examined for lesions and hair characteristics? | back 68 Scalp |
front 69 During embryologic development, the thyroid gland migrates downward
along which structure of the neck? | back 69 B. Midline of the neck |
front 70 Failure of the embryologic thyroid migration tract to close may
result in formation of a: | back 70 C. Thyroglossal duct cyst |
front 71 A thyroglossal duct cyst forms when the persistent tract fills
with: | back 71 B. Fluid or thick mucous-like material |
front 72 A thyroglossal duct cyst most commonly appears as which type of neck
mass? | back 72 B. Midline soft round mass |
front 73 Thyroglossal duct cysts are most commonly detected during which
period of life? | back 73 C. Early childhood |
front 74 The typical size of a thyroglossal duct cyst is approximately
comparable to a: | back 74 B. Ping pong ball |
front 75 Before surgical removal of a thyroglossal duct cyst, clinicians must
confirm the presence of a: | back 75 C. Normal thyroid gland |
front 76 Thyroid tissue within a thyroglossal duct cyst may rarely develop
which condition? | back 76 B. Thyroid cancer |
front 77 Forward displacement or bulging of the eyeball observed during
examination is termed: | back 77 B. Proptosis |
front 78 Bilateral proptosis is classically associated with which
disorder? | back 78 B. Graves disease |
front 79 Enlargement of the thyroid gland commonly results in: | back 79 B. Enlarged neck |
front 80 Prominent superficial veins in the neck may be observed in patients
with: | back 80 A. Goiter |
front 81 Multiple nodular neck masses are most commonly associated with: | back 81 B. Multinodular goiter |
front 82 Auscultation of the neck during physical examination is commonly
performed to detect: | back 82 C. Carotid bruits |
front 83 What approach? Anterior or Posterior? Pt neck flexed and turning chin slightly to right- relax SCM on that side and easier to perform Left hand of doc displace larynx to left and during swallowing, displaced left thyroid lobe palpated between examiner's right thumb and left SCM muscle | back 83 Anterior |
front 84 What approach? Anterior or Posterior? - patient neck slightly extended | back 84 Posterior |
front 85 For thyroid exam: Unusual ____ - cancer or scarring | back 85 hardness Softness |
front 86 When palpating lymph nodes of the head and neck, the examiner should
assess for: | back 86 B. Mobility, consistency, tenderness |
front 87 Tender cervical lymph nodes are most commonly associated with: | back 87 B. Inflammation |
front 88 Fixed, firm lymph nodes on neck palpation are most concerning
for: | back 88 C. Malignancy |
front 89 Tenderness of the thyroid gland is most commonly associated
with: | back 89 B. Acute infection or hemorrhage |
front 90 If the thyroid gland is enlarged, additional examination should
include: | back 90 A. Auscultation |
front 91 Which part of the stethoscope is best used to auscultate an enlarged thyroid gland? | back 91 Bell |
front 92 During thyroid auscultation, the bell of the stethoscope is placed
over the: | back 92 B. Thyroid lobes |
front 93 A bruit heard over the thyroid gland represents: | back 93 B. Turbulent blood flow |
front 94 A systolic bruit heard over the superior pole of the thyroid is
highly suggestive of: | back 94 B. Toxic goiter |
front 95 To palpate the supraclavicular nodes, the examiner is best
positioned: | back 95 B. Behind patient |
front 96 Supraclavicular nodes are palpated by placing the fingers: | back 96 C. In the medial supraclavicular fossae |
front 97 While palpating the supraclavicular nodes, the examiner presses
deeply: | back 97 C. Into and behind clavicles |
front 98 Which adjacent muscle serves as a landmark during palpation of supraclavicular nodes? | back 98 Sternocleidomastoid |
front 99 Supraclavicular lymph nodes are most likely to become palpable when
the patient: | back 99 C. Inspires deeply |
front 100 Iodine deficiency = thyroid ______ | back 100 enlarged |
front 101 Causes of ______ - infection, AI disease, cancer, isolated nodules | back 101 goiter |
front 102 ______ thyroid = hyperthyroidism, hypothyroid, or simple or multinodular goiter of normal function | back 102 Enlarged |
front 103 Pemberton’s sign is primarily used to detect obstruction in which
anatomical region? | back 103 A. Thoracic inlet |
front 104 Pemberton’s sign is tested by asking the patient to: | back 104 B. Elevate both arms overhead |
front 105 During the Pemberton maneuver, the patient’s arms are raised until
they: | back 105 B. Touch the side of head |
front 106 A positive Pemberton’s sign initially presents with: | back 106 B. Facial suffusion and neck vein dilation |
front 107 If the Pemberton maneuver continues for 1–2 minutes in a positive
test, the patient’s face may become: | back 107 D. Cyanotic |
front 108 The most common cause of hyperthyroidism is: | back 108 C. Diffuse toxic goiter |
front 109 Diffuse toxic goiter is also known as: | back 109 A. Graves disease |
front 110 Graves disease is classified as which type of disorder? | back 110 B. Autoimmune disorder |
front 111 Graves disease is caused by production of which antibody? | back 111 B. Thyroid-stimulating immunoglobulin |
front 112 A patient with hyperthyroidism most commonly presents with which skin
finding? | back 112 B. Warm skin |
front 113 Which neurologic symptom is commonly associated with
hyperthyroidism? | back 113 A. Hand tremor |
front 114 Which psychiatric symptom is frequently seen in
hyperthyroidism? | back 114 B. Anxiety and insomnia |
front 115 Heat intolerance in hyperthyroidism is primarily due to: | back 115 B. Increased metabolic rate |
front 116 Which reproductive symptom may occur in women with hyperthyroidism? | back 116 Amenorrhea |
front 117 Excessive sweating associated with hyperthyroidism is termed: | back 117 B. Hyperhidrosis |
front 118 Which ocular sign is classically associated with Graves
disease? | back 118 B. Proptosis |
front 119 Hyperthyroidism may also cause cardiovascular symptoms such as: | back 119 B. Palpitations |
front 120 Changes in which structure may occur in hyperthyroidism leading to
abnormal growth patterns? | back 120 B. Nails |
front 121 Hyperthyroidism may occasionally be caused by which thyroid
abnormality? | back 121 C. Hot nodule |
front 122 Patient with exophthalmos, weight loss, palpitations: Thyroglossal duct cyst Thyroid carcinoma Graves’ Disease | back 122 Graves’ Disease |
front 123 Older patient with firm, non-tender thyroid nodule: Thyroglossal duct cyst Thyroid carcinoma Graves’ Disease | back 123 Thyroid carcinoma |
front 124 Young patient with midline neck mass moving with swallowing: Thyroglossal duct cyst Thyroid carcinoma Graves’ Disease | back 124 Thyroglossal duct cyst |
front 125 Patient with progressively enlarging lateral neck mass: Laryngeal SCC Lymphoma or metastatic carcinoma Meningitis | back 125 Lymphoma or metastatic carcinoma |
front 126 Neck stiffness, fever, photophobia: Laryngeal SCC Lymphoma or metastatic carcinoma Meningitis | back 126 Meningitis |
front 127 Elderly male smoker with hoarseness >2 weeks: Laryngeal SCC Lymphoma or metastatic carcinoma Meningitis | back 127 Laryngeal SCC |
front 128 During axillary examination, proper technique requires the pectoral
muscles to be: | back 128 B. Fully relaxed |
front 129 When examining the patient’s right axilla, the examiner supports the
patient’s right forearm with the examiner’s: | back 129 C. Right hand |
front 130 In right axillary palpation, the examining fingers are usually those
of the examiner’s: | back 130 A. Left hand |
front 131 At the start of palpating the axilla, the examiner’s fingers should
be placed: | back 131 B. Low in the axilla |
front 132 As the patient’s right arm is drawn medially, the examiner should
move the palpating hand: | back 132 A. Upward into the axilla |
front 133 In addition to the axilla, which regions are specifically included in
this lymph node exam? | back 133 C. Supraclavicular and subclavian |
front 134 Which finger movement is recommended for detecting adenopathy in the
axilla? | back 134 C. Small circular motions |
front 135 During this palpation technique, the examiner’s fingers are described
as: | back 135 B. Riding over the ribs |
front 136 Freely mobile axillary nodes measuring 3 to 5 mm are generally
considered: | back 136 A. Common benign findings |
front 137 Small mobile axillary lymph nodes most often suggest lymphadenitis
secondary to: | back 137 B. Minor hand trauma |
front 138 Which body region is specifically mentioned as a source of trauma
leading to these reactive nodes? | back 138 C. Hand and arm |
front 139 After one axilla has been examined, the other should be assessed with
the examiner’s: | back 139 C. Opposite hand |
front 140 Orthostatic hypotension: Dizziness may accompany the _____ in blood pressure. In most affected patients, there is also an _____ in heart rate. | back 140 drop increase |
front 141 Risk factors: old age, meds, cardiac, heat exposure, bed rest, pregnancy, alcohol What is this? | back 141 Orthostatic hypotension |
front 142 Korotkoff sounds are best described as: | back 142 B. Turbulent arterial sounds |
front 143 Korotkoff sounds are produced when a blood pressure cuff: | back 143 A. Partially occludes an artery |
front 144 Which Korotkoff phase is most accurate for determining diastolic
blood pressure in adults? | back 144 D. Phase 5 |
front 145 Compared with phase 4 muffling, phase 5 is preferred because it
reflects: | back 145 B. Sound disappearance |
front 146 Masked hypertension refers to patients who: | back 146 C. Appear normal in clinic |
front 147 Masked hypertension is especially concerning because it indicates
increased risk of: | back 147 C. Cardiovascular disease |
front 148 If the patient’s arm is not supported at heart level during BP
measurement, the reading may be falsely high because the patient is
performing: | back 148 B. Isometric exercise |
front 149 Failure to support the arm properly most directly causes an
artificially elevated: | back 149 B. Blood pressure reading |
front 150 Pressing too hard with the diaphragm significantly lowers which
measurement? | back 150 A. Diastolic pressure |
front 151 When positioning the cuff, the bladder should be centered over
the: | back 151 C. Brachial artery |
front 152 During blood pressure measurement by palpation, the systolic pressure
is identified by the: | back 152 B. Return of brachial pulse |
front 153 Coarctation of the aorta may occur as an isolated defect or in
association with which cardiac lesion? | back 153 C. Bicuspid aortic valve |
front 154 Which additional congenital lesion is commonly associated with
coarctation of the aorta? | back 154 A. Ventricular septal defect |
front 155 In a new patient with hypertension, evaluation for coarctation should
always include blood pressure measurement in the: | back 155 B. Lower extremity |
front 156 During blood pressure assessment for suspected coarctation, the
patient is positioned: | back 156 C. Prone |
front 157 For lower-extremity blood pressure measurement in suspected
coarctation, the cuff is placed around the: | back 157 C. Posterior midthigh |
front 158 When measuring leg blood pressure for coarctation, the stethoscope is
commonly placed over the: | back 158 B. Popliteal fossa |
front 159 In addition to the popliteal artery, which distal artery may be used
for auscultation during this exam? | back 159 C. Dorsalis pedis artery |
front 160 Which other distal artery may be used when checking lower-extremity
pressure in suspected coarctation? | back 160 A. Posterior tibial artery |
front 161 A leg systolic blood pressure lower than the arm systolic pressure
should raise suspicion for: | back 161 B. Coarctation of the aorta |
front 162 Suspicion for coarctation increases further when the femoral pulse
is: | back 162 D. Delayed compared with radial |
front 163 In a normal patient, the femoral and radial pulses should: | back 163 B. Peak at the same time |
front 164 Which pulse comparison is specifically useful when evaluating
possible coarctation of the aorta? | back 164 B. Radial and femoral |
front 165 A delayed femoral pulse relative to the radial pulse is classically
termed: | back 165 B. Radiofemoral delay |
front 166 The reason lower-extremity blood pressure is important in new
hypertension evaluation is that coarctation can: | back 166 B. Be missed without leg comparison |
front 167 During general inspection, the examiner should first assess the
patient’s: | back 167 A. State of consciousness and grooming |
front 168 In overall inspection, nutritional status is evaluated because
chronically ill patients are more often: | back 168 B. Cachectic rather than overweight |
front 169 A thin body habitus with poor muscle development, small bone
structure, and malnourishment is termed: | back 169 C. Asthenic |
front 170 An athletic build with well-developed muscles and bones is most
consistent with which body type? | back 170 D. Sthenic |
front 171 A short, rounded body habitus with good musculature but frequent
weight problems is described as: | back 171 A. Hypersthenic |
front 172 During inspection, asymmetry is important because it may
suggest: | back 172 B. Underlying focal pathology |
front 173 Left supraclavicular swelling on inspection should raise concern
for: | back 173 C. Gastric carcinoma |
front 174 A miotic pupil in the setting of asymmetry may suggest a: | back 174 A. Tumor of the lung apex |
front 175 A left-sided varicocele may be a clue to: | back 175 B. Hypernephroma |
front 176 Inspection of speech patterns can provide important information
about: | back 176 A. Cranial nerve function |
front 177 A basic mental status screen during inspection should include
orientation to: | back 177 B. Person, place, and date |
front 178 Which of the following is one of the cardinal signs of
inflammation? | back 178 C. Redness |
front 179 Which set correctly lists the classic cardinal signs of
inflammation? | back 179 A. Swelling, heat, redness, pain, disturbed function |
front 180 The pain associated with swelling is primarily caused by: | back 180 B. Increased pressure on nerve fibers |
front 181 Which inspection finding best reflects a disturbance of function as
part of inflammation? | back 181 A. Inability to use the affected part |
front 182 Which body type is most likely to be described as thin with poor
musculature? | back 182 D. Ectomorphic |
front 183 During palpation of the chest, an abnormal impulse on the right side
is most concerning for: | back 183 A. Ascending aortic aneurysm |
front 184 A pulsatile mass palpated in the abdomen should raise concern
for: | back 184 C. Abdominal aortic aneurysm |
front 185 An acutely tender right upper quadrant mass that descends with
inspiration is most likely: | back 185 D. Inflamed gallbladder |
front 186 Which condition is most likely to change the percussion note? | back 186 B. Collapsed lung |
front 187 A dull percussion note in the lower midline abdomen of a man most
likely represents: | back 187 A. Distended urinary bladder |
front 188 When examining the heart, chest, and abdomen, auscultation should
be: | back 188 C. Combined with other techniques |
front 189 Absence of normal bowel sounds should raise concern for: | back 189 B. Surgical emergency |
front 190 Daylight is preferred for physical examination because artificial
light may: | back 190 D. Mask skin color changes |
front 191 Before beginning the examination, the examiner should: | back 191 C. Wash hands |
front 192 During the exam, it is best to: | back 192 A. Minimize unnecessary movement |
front 193 Physical examination is generally organized by: | back 193 D. Body regions |
front 194 By convention, the examiner stands: | back 194 B. At the patient’s right |
front 195 By convention, the examiner primarily uses the: | back 195 A. Right hand |
front 196 Which statement should the examiner avoid during the
examination? | back 196 D. “That’s normal” |
front 197 Universal precautions assume that all blood and body fluids may
contain: | back 197 C. Blood-borne pathogens |
front 198 In occupational exposure, the most important source of HIV, HBV, and
HCV infection is: | back 198 B. Blood |
front 199 Which preventive measure is specifically recommended for healthcare
workers regarding HBV? | back 199 D. HBV vaccination |
front 200 Which item is considered a protective barrier? | back 200 A. Gloves |
front 201 Which is also listed as a protective barrier? | back 201 B. Gown |
front 202 Which item belongs to standard protective barriers? | back 202 C. Mask |
front 203 Which piece of equipment is included among protective
barriers? | back 203 A. Eye protection |
front 204 Compared with lung collapse, which finding generally does not alter
the percussion note? | back 204 D. Solid abdominal mass |
front 205 Which finding most strongly supports acute gallbladder
inflammation? | back 205 B. RUQ mass descends inspiration |
front 206 Which statement best reflects proper overall exam technique? | back 206 C. Integrate methods and precautions |
front 207 Transmission-based precautions are primarily intended to: | back 207 A. Decrease pathogen transmission in hospitals |
front 208 Which infection requires airborne precautions? | back 208 B. Tuberculosis |
front 209 A patient with suspected varicella should be placed in a: | back 209 C. Negative-pressure room |
front 210 Which personal protective equipment is specifically required for
airborne precautions? | back 210 D. N95 respirator |
front 211 Droplet precautions are used for pathogens spread primarily
by: | back 211 A. Large respiratory droplets |
front 212 Which precaution category is most appropriate for many respiratory
viruses? | back 212 B. Droplet precautions |
front 213 Under droplet precautions, appropriate protective equipment
includes: | back 213 A. Surgical mask and gloves |
front 214 Contact precautions are mainly used for pathogens spread by: | back 214 C. Skin contact or surfaces |
front 215 Which infection is a classic indication for contact
precautions? | back 215 D. Clostridioides difficile |
front 216 Which combination is standard for contact precautions? | back 216 D. Gown and gloves |
front 217 After a needlestick injury, the affected area should first
be: | back 217 A. Flushed vigorously with water |
front 218 After initial cleansing of a needlestick injury, the next step is
to: | back 218 B. Seek guidance from the needlestick coordinator |
front 219 When indicated after needlestick exposure, HIV postexposure
prophylaxis should be started: | back 219 C. As soon as possible |
front 220 Following a needlestick injury, the exposed provider should also be
tested for: | back 220 A. Hepatitis B or hepatitis C |
front 221 Which vaccine is specifically recommended for all healthcare workers
with direct patient contact? | back 221 B. Hepatitis B vaccine |
front 222 In addition to hepatitis B vaccination, healthcare workers should
receive the: | back 222 D. Annual influenza vaccine |
front 223 The most important contributors to validity of the physical
examination are: | back 223 C. Clinical experience and technique reliability |
front 224 False-positive and false-negative findings primarily reduce
the: | back 224 A. Precision of examination techniques |
front 225 Which factor can distort the examiner’s interpretation of a physical
finding? | back 225 B. Unconscious bias |
front 226 Which statement best reflects a core goal of the physical
exam? | back 226 D. Reliable methods improve diagnostic validity |
front 227 Measures the proportion of actual positives correctly identified: specificty sensitivity negative predictive value positive predictive value | back 227 sensitivity |
front 228 Measures the proportion of actual negatives correctly identified: specificty sensitivity negative predictive value positive predictive value | back 228 specificty |
front 229 The probability that a person with a positive test actually has the disease: specificty sensitivity negative predictive value positive predictive value | back 229 positive predictive value |
front 230 The probability that a person with a negative test actually does not have the disease: specificty sensitivity negative predictive value positive predictive value | back 230 negative predictive value |
front 231 breathlessness, chronic coughing (with or without | back 231 COPD |
front 232 COPD can be diagnosed with ________ | back 232 spirometry |
front 233 Which muscles provide the primary power for normal inspiration? | back 233 A. Intercostals and diaphragm |
front 234 Under normal resting conditions, expiration is usually: | back 234 B. Passive |
front 235 The primary breathing center is located in the: | back 235 C. Medulla |
front 236 The trachea normally bifurcates into the main bronchi at
approximately: | back 236 D. T4–T5 |
front 237 Compared with the left main bronchus, the right main bronchus
is: | back 237 A. Shorter, wider, and straighter |
front 238 Which airway sequence is correct from larger to smaller
structures? | back 238 B. Bronchi → bronchioles → alveolar duct → alveolar sac |
front 239 Which type of fissure is present in both lungs? | back 239 C. Oblique fissure |
front 240 On the anterior chest, the oblique fissure begins near the: | back 240 D. Sixth rib at MCL |
front 241 As it courses laterally, the oblique fissure reaches approximately
the: | back 241 A. Fifth rib at MAL |
front 242 Posteriorly, the oblique fissure ends near the: | back 242 B. T3 spinous process |
front 243 Which lobe lies inferior to the right oblique fissure? | back 243 C. Right lower lobe |
front 244 Which lobes lie superior to the right oblique fissure? | back 244 D. Right upper and middle |
front 245 Which lobe lies inferior to the left oblique fissure? | back 245 A. Left lower lobe |
front 246 Which lobe lies superior to the left oblique fissure? | back 246 B. Left upper lobe |
front 247 A foreign body is more likely to enter the right main bronchus
because it is: | back 247 C. Shorter, wider, and straighter |
front 248 Which statement about the horizontal fissure is correct? | back 248 B. It is present only in the right lung |
front 249 The horizontal fissure separates which two lobes? | back 249 A. Right upper from right middle |
front 250 The horizontal fissure extends from the sternal border of the: | back 250 C. Fourth rib |
front 251 Laterally, the horizontal fissure reaches the: | back 251 B. Fifth rib at MAL |
front 252 The bifurcation of the trachea is called the: | back 252 C. Carina |
front 253 The carina lies approximately at the level of the: | back 253 D. T4 vertebra |
front 254 The angle of Louis is an important landmark because it approximates
the level of the: | back 254 A. Carina |
front 255 At the end of expiration, the right hemidiaphragm is located
anteriorly near the: | back 255 D. Fifth rib |
front 256 Posteriorly, the right hemidiaphragm at end-expiration is near: | back 256 B. T9 |
front 257 The right hemidiaphragm normally sits slightly higher than the left
primarily because of the: | back 257 C. Liver |
front 258 Which pulmonary symptom is most common? | back 258 A. Cough |
front 259 A cough is best described as a: | back 259 B. Coordinated forced expiration |
front 260 Repeated closure of which structure interrupts the cough
reflex? | back 260 D. Glottis |
front 261 During coughing, expiratory muscles contract against a partially
closed glottis, causing: | back 261 C. High intrapulmonary pressure |
front 262 When the glottis suddenly opens during a cough, the result is: | back 262 B. Explosive rush of air |
front 263 The most common cause of chronic cough is probably: | back 263 A. Tobacco smoking |
front 264 Smoker’s cough is caused primarily by: | back 264 D. Inhaled tobacco irritants |
front 265 Smoker’s cough is usually most prominent: | back 265 C. In the morning |
front 266 A psychogenic cough is typically: | back 266 B. Nonproductive and stress-related |
front 267 Psychogenic cough should be diagnosed only: | back 267 D. After excluding other causes |
front 268 Uninfected sputum is usually described as: | back 268 A. Odorless mucoid material |
front 269 Uninfected sputum most commonly appears: | back 269 B. Transparent whitish-gray |
front 270 Sputum containing pus is termed: | back 270 C. Purulent |
front 271 Purulent sputum is often what color? | back 271 D. Yellow or greenish |
front 272 Hemoptysis can occur when pulmonary emboli cause: | back 272 C. Pulmonary infarction |
front 273 Hemoptysis from pulmonary embolism is associated with necrosis of
the: | back 273 B. Pulmonary parenchyma |
front 274 The most common cause of hemoptysis is probably: | back 274 A. Bronchitis |
front 275 Patients with hemoptysis may report which associated sensation? | back 275 D. Warmth in the chest |
front 276 Sudden shortness of breath that awakens a patient from sleep is
called: | back 276 C. Paroxysmal nocturnal dyspnea |
front 277 Which feature best characterizes paroxysmal nocturnal dyspnea? | back 277 B. Improves when sitting up |
front 278 Difficulty breathing while lying flat is termed: | back 278 A. Orthopnea |
front 279 A patient who needs multiple pillows to sleep most likely has: | back 279 B. Orthopnea |
front 280 Dyspnea that occurs while sitting upright and improves when lying
down is called: | back 280 D. Platypnea |
front 281 A patient reports breathing is easier only when lying on the left
side. This is called: | back 281 B. Trepopnea |
front 282 Unexplained dyspnea should prompt further questioning about: | back 282 A. Industrial exposure |
front 283 Wheezes are best described as: | back 283 C. High-pitched sounds from narrowed airways |
front 284 Wheezes are usually heard most prominently during: | back 284 D. Expiration |
front 285 The usual mechanism producing wheezing is: | back 285 B. Partially obstructed airflow |
front 286 Which condition is a classic cause of wheezing due to
bronchospasm? | back 286 A. Asthma |
front 287 Which of the following can also cause wheezing? | back 287 A. Mucosal edema |
front 288 Loss of elastic support in the airways may contribute to: | back 288 C. Wheezing |
front 289 Which structural abnormality can cause wheezes? | back 289 A. Tortuous airways |
front 290 Which obstructive problem may produce wheezing? | back 290 B. Foreign body obstruction |
front 291 A decrease in wheezing may indicate: | back 291 A. Airway opening or severe worsening |
front 292 In acute asthma, disappearance of wheezing may be dangerous because
it can reflect: | back 292 C. Progressive airway closure |
front 293 A “silent chest” during an acute asthmatic attack is: | back 293 D. An ominous sign |
front 294 A silent chest in asthma most strongly suggests: | back 294 A. Worsening obstruction |
front 295 Central cyanosis most commonly results from: | back 295 B. Inadequate gas exchange in the lungs |
front 296 Which location is most useful for detecting central cyanosis? | back 296 A. Oral mucous membranes and lips |
front 297 Cyanosis of the nails accompanied by warm hands is most suggestive
of: | back 297 D. Central cyanosis |
front 298 A cyanotic area that does not disappear after warming is most
consistent with: | back 298 C. Central cyanosis |
front 299 Which nail finding may accompany longstanding central cyanosis? | back 299 A. Clubbing |
front 300 Central cyanosis typically becomes more pronounced with: | back 300 D. Exercise |
front 301 Peripheral cyanosis occurs primarily because of: | back 301 C. Excessive oxygen extraction in the periphery |
front 302 Peripheral cyanosis is usually limited to the: | back 302 B. Fingers, toes, and nose |
front 303 Which feature best distinguishes peripheral cyanosis from central
cyanosis? | back 303 A. It disappears when the area is warmed |
front 304 Hereditary methemoglobinemia is a cause of: | back 304 D. Congenital cyanosis |
front 305 Pleuritic chest pain is usually caused by inflammation of the: | back 305 C. Parietal pleura |
front 306 Pleuritic pain is classically described as: | back 306 B. Sharp and worse with inspiration |
front 307 Snoring is strongly associated with: | back 307 A. Obstructive sleep apnea |
front 308 Which patient profile is most suggestive of obstructive sleep
apnea? | back 308 D. Overweight patient with daytime sleepiness |
front 309 Nasal flaring on general assessment most directly suggests: | back 309 B. Increased work of breathing |
front 310 Prominent use of the sternocleidomastoid and trapezius during
inspiration suggests: | back 310 C. Airway obstruction |
front 311 Increased anteroposterior chest diameter is commonly seen in: | back 311 A. Advanced COPD |
front 312 When the AP diameter equals the lateral chest diameter, the finding
is called: | back 312 D. Barrel chest |
front 313 Flail chest is characterized by: | back 313 C. Paradoxical inward chest movement during inspiration |
front 314 Flail chest is most commonly associated with: | back 314 D. Multiple rib fractures |
front 315 Kyphoscoliosis is best described as: | back 315 D. Abnormal AP diameter with lateral spinal curvature |
front 316 The major respiratory consequence of severe kyphoscoliosis is: | back 316 B. Restricted chest and lung expansion |
front 317 Pectus excavatum is associated with: | back 317 C. Mitral valve prolapse |
front 318 Which finding favors central rather than peripheral cyanosis? | back 318 D. Blue lips with oral mucosal discoloration |
front 319 Tactile fremitus is most useful for assessing the: | back 319 A. Density of underlying lung tissue |
front 320 Which process typically increases tactile fremitus? | back 320 B. Lung consolidation |
front 321 Pneumonia increases tactile fremitus primarily because the lung
becomes: | back 321 A. More solid |
front 322 Which factor would most likely decrease tactile fremitus? | back 322 C. Excess chest wall fat |
front 323 Air in the chest cavity generally causes tactile fremitus to: | back 323 D. Decrease |
front 324 Fluid in the chest cavity usually causes tactile fremitus to: | back 324 B. Decrease |
front 325 Overexpansion of the lungs, as in emphysema, generally causes tactile
fremitus to: | back 325 C. Decrease |
front 326 Which percussion note is expected over normal lung? | back 326 A. Resonant |
front 327 Which percussion note is expected over the stomach? | back 327 C. Tympanic |
front 328 Percussion over the liver normally produces a: | back 328 B. Dull note |
front 329 Which percussion note is expected over the thigh? | back 329 D. Flat |
front 330 Which combination best fits pneumonia? | back 330 D. Increased fremitus, increased resonance |
front 331 Which combination best fits pneumothorax? | back 331 C. Decreased fremitus, increased resonance |
front 332 Which combination best fits pleural effusion? | back 332 A. Decreased fremitus, decreased resonance |
front 333 Smoker with chronic cough, dyspnea, barrel chest, pursed-lip breathing | back 333 Emphysema (COPD) |
front 334 Young patient with wheezing, intermittent dyspnea, and nocturnal cough | back 334 Asthma |
front 335 Patient with fever, productive cough, bronchial breath sounds, dullness on percussion | back 335 Pneumonia |
front 336 Post-op patient with sudden dyspnea, pleuritic chest pain, tachycardia | back 336 Pulmonary Embolism |
front 337 Thin young male with sudden chest pain and absent breath sounds on one side | back 337 Spontaneous Pneumothorax |
front 338 Patient with dull percussion, absent breath sounds, and tracheal shift away | back 338 Large Pleural Effusion |
front 339 Which cerebral structure subserves higher mental, sensory, motor, and
associative processing? | back 339 B. Cerebrum |
front 340 A patient has a small infarct causing impaired voluntary movement of
the right arm and leg. The lesion most likely involves the: | back 340 C. Precentral gyrus |
front 341 Fibers arising from the primary motor cortex normally govern: | back 341 B. Contralateral skeletal movement |
front 342 A cortical lesion produces flaccid paralysis of the left face, arm,
and leg. The lesion is most likely in the: | back 342 A. Right precentral gyrus |
front 343 A patient reports numb “pins-and-needles” over the right body after a
cortical stroke. The damaged cortex is most likely the: | back 343 A. Left postcentral gyrus |
front 344 The primary sensory cortex is located in the: | back 344 C. Postcentral gyrus |
front 345 The primary visual cortex is centered in the: | back 345 D. Occipital lobe |
front 346 The fissure closely associated with primary visual cortex is
the: | back 346 C. Calcarine fissure |
front 347 The calcarine fissure anatomically separates the: | back 347 A. Cuneus and lingual gyri |
front 348 A patient with a right visual cortex lesion develops a left visual
field deficit. The most likely deficit is: | back 348 C. Left homonymous hemianopsia |
front 349 Occipital cortical irritation may cause all of the following
except: | back 349 D. Complete central blindness |
front 350 In a classic primary visual cortex lesion, which visual function is
often preserved? | back 350 C. Central macular vision |
front 351 The primary auditory cortex lies in the: | back 351 B. Temporal lobe |
front 352 The gyrus most closely associated with primary auditory cortex is
the: | back 352 D. Transverse temporal gyrus |
front 353 A destructive lesion of primary auditory cortex most
characteristically causes: | back 353 C. Tinnitus without true deafness |
front 354 Which structure is classically linked to emotion as part of the
limbic system? | back 354 B. Amygdala |
front 355 The basal ganglia are most directly involved in modulation of: | back 355 C. Fine voluntary movement, posture, autonomic integration |
front 356 Basal ganglia lesions are most likely to produce: | back 356 B. Tremor and rigidity |
front 357 The thalamus lies on each side of the: | back 357 D. Third ventricle |
front 358 All sensory pathways except which modality relay through the
thalamus? | back 358 C. Olfaction |
front 359 In addition to sensory relay, the thalamus is a major site for: | back 359 A. Motor modulation |
front 360 A patient retains crude pain and temperature perception despite
destruction of primary sensory cortex. Which structure most likely
preserves this function? | back 360 B. Thalamus |
front 361 The structure most responsible for maintaining alertness and
attention by electrically exciting the cerebral cortex is the: | back 361 C. Thalamus |
front 362 Emotional coloring of sensory experiences is strongly associated with
the: | back 362 A. Thalamus |
front 363 Which pair is included with the hypothalamic region? | back 363 A. Optic chiasm, neurohypophysis |
front 364 Which function is most characteristically hypothalamic? | back 364 C. Water balance regulation |
front 365 The brainstem consists of the: | back 365 A. Midbrain, pons, medulla |
front 366 Cranial nerve nuclei associated with the brainstem are
primarily: | back 366 C. CN III–XII |
front 367 The brainstem reticular formation is most important for: | back 367 B. Constant muscle stimulation |
front 368 Injury to the ascending reticular activating system would most
directly impair: | back 368 A. Consciousness and arousal |
front 369 Which structure contains the superior and inferior colliculi? | back 369 C. Midbrain |
front 370 The motor nuclei of which cranial nerves are located in the
midbrain? | back 370 B. III and IV |
front 371 A lesion causing vertical gaze difficulty with impaired upward gaze
most likely involves the: | back 371 C. Superior colliculus |
front 372 The superior colliculi are functionally part of the: | back 372 B. Visual system |
front 373 The inferior colliculi are functionally part of the: | back 373 A. Auditory system |
front 374 A focal lesion of the cerebral peduncle would most likely
cause: | back 374 B. Contralateral spastic paralysis |
front 375 Relative to the cerebellum, the pons lies: | back 375 C. Ventral |
front 376 Relative to the medulla, the pons is: | back 376 A. Rostral |
front 377 Which cranial nerve range is classically associated with the
pons? | back 377 B. CN V–VIII |
front 378 The acoustic/vestibular nuclei are associated with: | back 378 C. CN VIII |
front 379 The medulla is located between the: | back 379 B. Pons and spinal cord |
front 380 A medullary lesion classically causes loss of pain and
temperature: | back 380 C. Contralaterally |
front 381 Hemiplegia from a medullary lesion is typically: | back 381 B. Contralateral |
front 382 Cranial nerve deficits from a medullary lesion most often
occur: | back 382 C. Ipsilaterally |
front 383 Which cranial nerve group is most associated with the medulla? | back 383 B. CN IX–XII |
front 384 The cerebellum is located in the: | back 384 B. Posterior cranial fossa |
front 385 The midline cerebellar structure is the: | back 385 C. Vermis |
front 386 The cerebellum consists of a vermis and: | back 386 B. Two lateral hemispheres |
front 387 Which function is most characteristic of the cerebellum? | back 387 B. Motor coordination |
front 388 The cerebellum is especially important for fine movements of
the: | back 388 C. Hands |
front 389 Which finding is most consistent with a cerebellar lesion? | back 389 B. Intention tremor |
front 390 Rapid alternating movement difficulty is called: | back 390 C. Dysdiadochokinesia |
front 391 A patient with a cerebellar lesion is most likely to have: | back 391 A. Staggering gait |
front 392 Proximally, the spinal cord is continuous with the: | back 392 B. Medulla |
front 393 Distally, the spinal cord attaches to the first part of the: | back 393 C. Coccyx |
front 394 The anterior horn of spinal gray matter is primarily: | back 394 B. Motor |
front 395 Sympathetic preganglionic neurons are located in the lateral horn
from: | back 395 B. T1–L2 |
front 396 The posterior horn of spinal gray matter is primarily: | back 396 B. Sensory |
front 397 In the spinal cord, gray matter is: | back 397 C. Central |
front 398 In the spinal cord, white matter is: | back 398 B. Peripheral |
front 399 The anterior white column contains the ventral: | back 399 B. Corticospinal tract |
front 400 The ascending tract in the anterior white column is the
ventral: | back 400 C. Corticobulbar tract |
front 401 The ventral corticospinal tract is mainly involved in: | back 401 B. Voluntary motion |
front 402 The ventral spinothalamic tract carries: | back 402 C. Light touch |
front 403 The lateral white column contains the lateral: | back 403 B. Corticospinal tract |
front 404 Which tract in the lateral white column conveys reflex
proprioception? | back 404 C. Spinocerebellar tract |
front 405 The lateral spinothalamic tract is found in the: | back 405 B. Lateral column |
front 406 The posterior white column contains the fasciculi: | back 406 A. Gracilis and cuneatus |
front 407 Which sensation is carried by the posterior columns? | back 407 C. Vibration sense |
front 408 Which modality is also carried in the posterior columns? | back 408 A. Passive motion |
front 409 Two-point discrimination is carried mainly by the: | back 409 B. Posterior white column |
front 410 How many pairs of spinal nerves are present? | back 410 B. 31 pairs |
front 411 The cell bodies of dorsal root fibers are in the: | back 411 C. Dorsal root ganglion |
front 412 A spinal reflex is best defined as coordination between afferent and
efferent neurons at the: | back 412 A. Same spinal level |
front 413 A patient loses pinprick on the right body after a left cord lesion.
Pain and temperature fibers normally: | back 413 A. Cross within 1–2 segments |
front 414 After crossing, pain and temperature fibers ascend in the: | back 414 B. Contralateral lateral spinothalamic tract |
front 415 Pain and temperature information ultimately projects from the
thalamus to the: | back 415 C. Postcentral gyrus |
front 416 Conscious proprioceptive fibers first ascend in the: | back 416 D. Dorsal columns |
front 417 Proprioceptive fibers from the cord initially synapse in: | back 417 B. Ipsilateral gracile or cuneate nuclei |
front 418 Proprioceptive fibers decussate in the: | back 418 A. Medial lemniscus |
front 419 Headache is the most common: | back 419 C. Neurologic symptom |
front 420 A sudden severe headache should raise concern for: | back 420 D. Stroke |
front 421 Continuous headaches are most often associated with: | back 421 A. Muscle spasm |
front 422 Recurrent headaches are classically associated with: | back 422 B. Migraine or cluster headache |
front 423 Throbbing headaches most strongly suggest: | back 423 C. Vascular problems |
front 424 Pain from the sinuses, eyes, or teeth causing headache is: | back 424 D. Referred pain |
front 425 Headaches may be accompanied by: | back 425 A. Visual phenomena, nausea, vomiting |
front 426 Migraine is best described as: | back 426 B. Biphasic aura then headache |
front 427 The prodromal phase of migraine is called the: | back 427 C. Aura |
front 428 During migraine aura, a patient may experience: | back 428 A. Photophobia, blurred vision, scotoma |
front 429 As a migraine aura fades, the next phase usually is: | back 429 B. Headache onset |
front 430 Classic migraine pain is typically: | back 430 C. Unilateral and pulsating |
front 431 Migraine duration commonly lasts: | back 431 D. Hours to days |
front 432 Which is a recognized migraine trigger? | back 432 A. Birth control pills |
front 433 Which dietary item can precipitate migraine? | back 433 B. Chocolate |
front 434 Migraine commonly has which background feature? | back 434 A. Family history |
front 435 Cluster headaches are attributed to: | back 435 B. Oculosympathetic disturbances |
front 436 The classic cluster headache patient is a middle-aged: | back 436 C. Man with eye pain |
front 437 Cluster headache pain usually centers around the: | back 437 D. Eye |
front 438 A single cluster headache attack usually lasts: | back 438 A. Up to 1 hour |
front 439 Cluster headaches often awaken patients: | back 439 C. From sleep repeatedly for 2-4 weeks |
front 440 Which finding occurs during a cluster headache? | back 440 B. Ipsilateral miosis |
front 441 Which additional sign supports cluster headache? | back 441 A. Ptosis and tearing |
front 442 Cluster headaches may be precipitated by: | back 442 C. Alcohol |
front 443 A child briefly stares, loses awareness for 10 seconds, then rapidly
returns to normal. This is most consistent with: | back 443 B. Absence seizure |
front 444 Generalized tonic-clonic seizure may begin with: | back 444 A. Aura of giddiness |
front 445 During the tonic phase of a grand mal seizure, the patient typically
has: | back 445 C. Rigidity with possible apnea |
front 446 During the clonic phase, a patient may have: | back 446 B. Salivation and eye rolling |
front 447 Which feature is common after a generalized tonic-clonic
seizure? | back 447 D. Postictal confusion or deep sleep |
front 448 Sudden brief contractions of the eyelids and forearms without loss of
consciousness suggest: | back 448 C. Myoclonic seizure |
front 449 Febrile convulsions are most common in children: | back 449 A. 6 months to 6 years |
front 450 Vertigo is best described as: | back 450 C. Spinning with unsteady walking |
front 451 Acute vertigo may be accompanied by: | back 451 A. Nausea, vomiting, sweating |
front 452 A patient has severe vertigo, vomiting, hearing loss, tinnitus, and
nystagmus away from the affected ear. The most likely diagnosis
is: | back 452 B. Meniere disease |
front 453 A medication known to damage the labyrinth and cause deafness
is: | back 453 C. Gentamicin |
front 454 Dizziness with stumbling should raise concern for: | back 454 B. Stroke |
front 455 Persistent unsteadiness upright due to vestibular-ocular-cerebellar
disruption is: | back 455 B. Ataxia |
front 456 Ataxia is typically worsened when the patient: | back 456 C. Closes the eyes |
front 457 Ataxia is often improved when the patient: | back 457 B. Watches the feet |
front 458 Motor ataxia usually reflects abnormality of the: | back 458 A. Cerebellum and central vestibular pathways |
front 459 Motor ataxia classically produces a: | back 459 C. Wide-based lurching gait |
front 460 Hemiparesis, paresthesia, hemianopsia, garbled speech, and limb
weakness suggest a: | back 460 D. Supratentorial lesion |
front 461 Nystagmus, vomiting, diplopia, altered consciousness, and yawning
suggest a: | back 461 B. Brainstem lesion |
front 462 Which symptom pair best matches brainstem lesion localization? | back 462 A. Diplopia and nystagmus |
front 463 After head trauma, a patient develops progressive confusion from a
venous bleed beneath the dura. This is most consistent with: | back 463 A. Subdural hematoma |
front 464 Head trauma with a subdural hematoma may commonly produce: | back 464 B. Changes in consciousness |
front 465 Sudden painless visual loss should make you think first of: | back 465 C. Vascular accident or detachment |
front 466 Chronic painless visual loss is more suggestive of: | back 466 A. Optic pathway compression |
front 467 Which condition is classically painful? | back 467 B. Acute closed-angle glaucoma |
front 468 Which glaucoma pattern is usually not painful? | back 468 C. Chronic open-angle glaucoma |
front 469 Visual loss occurring before a headache is most characteristic
of: | back 469 C. Migraine |
front 470 Transient monocular visual loss lasting only minutes from carotid
disease is: | back 470 B. Amaurosis fugax |
front 471 Amaurosis fugax is most commonly due to disease of the: | back 471 D. Internal carotid artery |
front 472 Amaurosis fugax usually lasts: | back 472 A. Up to 3 minutes |
front 473 Diplopia most directly involves dysfunction of: | back 473 B. CN III, IV, VI |
front 474 Which condition is a recognized cause of diplopia? | back 474 A. Thyroid disease |
front 475 Another classic cause of diplopia is: | back 475 C. Myasthenia gravis |
front 476 Brainstem lesions may produce: | back 476 A. Diplopia |
front 477 A complete oculomotor palsy most classically causes: | back 477 A. Ptosis and mydriasis |
front 478 In a complete CN III palsy, all extraocular movements are lost
except: | back 478 C. Abduction |
front 479 A painful complete CN III palsy should raise concern for: | back 479 A. Posterior communicating aneurysm |
front 480 Another cause of complete CN III palsy is: | back 480 B. Cavernous sinus thrombosis |
front 481 Language problems and slurred speech are common in: | back 481 B. Stroke |
front 482 Dementia is best defined as: | back 482 C. Progressive cognitive impairment |
front 483 Dementia most often impairs: | back 483 A. Orientation, memory, judgment |
front 484 Which is the most common cause of dementia listed here? | back 484 D. Alzheimer disease |
front 485 Which is also a listed cause of dementia? | back 485 A. Normal pressure hydrocephalus |
front 486 Transient ischemic attacks are best described as: | back 486 B. Short focal deficits |
front 487 TIAs usually last: | back 487 A. Only a few minutes |
front 488 TIAs are followed by complete: | back 488 C. Recovery |
front 489 Roughly what fraction of patients with TIAs develop stroke within 4–5
years? | back 489 C. 30% |
front 490 Which gait best matches Parkinson disease? | back 490 B. Short quick shuffling gait |
front 491 Physiologic tremor usually occurs at: | back 491 B. 10 to 12 per second |
front 492 Physiologic tremor becomes more obvious: | back 492 A. After exercise |
front 493 Intention tremor is typically: | back 493 B. Slow and movement-worsened |
front 494 Intention tremor frequency is usually: | back 494 C. 2 to 4 per second |
front 495 Which is a listed cause of intention tremor? | back 495 A. Multiple sclerosis |
front 496 Which other setting can cause intention tremor? | back 496 B. Alcohol withdrawal |
front 497 Chorea is characterized by: | back 497 A. Involuntary jerky movements |
front 498 Chorea is classically associated with: | back 498 C. Huntington disease |
front 499 Huntington disease commonly includes: | back 499 A. Personality change, dementia |
front 500 Lower extremity numbness is especially common in: | back 500 B. Diabetes mellitus |
front 501 Numbness occurring essentially anywhere is more typical of: | back 501 C. Multiple sclerosis |
front 502 Proximal arm weakness makes it hardest to: | back 502 D. Brush hair |
front 503 Distal arm weakness most impairs: | back 503 C. Buttoning clothes |
front 504 Distal leg motor weakness classically causes: | back 504 B. Footdrop |
front 505 Proximal leg weakness makes it difficult to: | back 505 A. Climb stairs |
front 506 Trigeminal neuralgia is best described as: | back 506 A. Extreme jabbing facial pain |
front 507 Trigeminal neuralgia most often involves which divisions? | back 507 B. Maxillary and mandibular |
front 508 Trigeminal neuralgia may be provoked by: | back 508 A. Touch, chewing, cold |
front 509 Herpes zoster infection of a sensory root is called: | back 509 C. Shingles |
front 510 Shingles typically produces: | back 510 B. Linear vesicular eruption |
front 511 In shingles, the rash usually appears: | back 511 B. 3–4 days after pain |
front 512 Pain in shingles follows the: | back 512 C. Sensory root distribution |
front 513 ____ ____ of the ulnar aspect of the forearm and hand may be responsible for epitrochlear adenopathy. Epitrochlear nodes are also observed in non-Hodgkin ____. | back 513 Acute infections lymphoma |
front 514 true or false for carotids: It is often helpful to ask the patient to hold their breath during the auscultation. Usually, either nothing or transmitted heart sounds are heard. | back 514 true |
front 515 carotids: The presence of a _____ should be noted. This may be a _____ resulting from local atherosclerotic disease of the carotid artery. Loud murmurs originating from the heart can occasionally be transmitted to the _____. With experience, the examiner can determine whether the disorder is local in the neck or distal in the heart. | back 515 murmur bruit neck |
front 516 _____ is responsible for motor, sensory, associative, and higher mental functions | back 516 Cerebrum |
front 517 Chief sensory and motor integrating mechanism | back 517 thalamus |
front 518 Maintains and regulates consciousness, alertness, and attention by electrically exciting the cerebral cortex | back 518 thalamus |
front 519 Acts to maintain orientation in space and modulate movements Responsible for fine movements of the hands | back 519 cerebellum |
front 520 Coordinates and refines muscle group actins for smoothness and accuracy | back 520 cerebellum |
front 521 80% of the brain blood supply is from the ________ | back 521 ICAs |
front 522 _____ horn contains sympathetic preganglionic neurons from T1-L2 | back 522 lateral |
front 523 Lateral CS tract does _____ movement | back 523 voluntary reflex |
front 524 _____ _____ column is btwn the posterolateral and posterior median sulci: Contains ascending fibers of the fasciculus gracilis and cuneatus | back 524 Posterior white |
front 525 _____ fibers pass into dorsal columns, fasciculus gracilis or cuneatus to their ipsilateral nuclei, cross in the _____ _____, thalamus, postcentral gyrus | back 525 Proprioception medial lemniscus |
front 526 wide-based gait with irregular placement of the feet and poor center of gravity, with lurching to each side: _____ ataxia due to ______ | back 526 motor lurching |
front 527 Understand written and verbal commands but cannot repeat them: _____ lobe lesion | back 527 frontal |
front 528 Patient has difficulty understanding written and verbal commands and cannot repeat them: _____ lobe lesion | back 528 Temporoparietal |
front 529 _____ is failure to recognize a sensory stimulus despite normal primary sensation | back 529 Agnosnia |
front 530 _____ _____ is when a patient has normal vision and can’t recognize an object. | back 530 Visual agnosia |
front 531 _____ _____ is failure to recognize based on palpation. | back 531 Tactile agnosia |
front 532 _____ is inability to perform a voluntary movement in absence of
deficits in motor strength, sensation, or _____ is decreased ability to perform the activity _____ apraxia: the patient is unable to construct or draw simple design | back 532 Apraxia Dyspraxia Constructional |
front 533 still able to wrinkle forehead in _____ lesion | back 533 UMN |
front 534 Pt lies on back and tongue blade is quickly stroked horizontally
laterally to medially towards the umbilicus. This will cause a
contraction of the abdominal muscles with umbilicus deviating towards
stimulus b. Oppenhiem’s sign c. Chaddock’s sign d. Hoffmann’s sign | back 534 a. Abdominal superficial reflex |
front 535 stroke the lateral aspect of foot and if the big toe
a. Abdominal superficial reflex b. Oppenhiem’s sign c. Chaddock’s sign d. Hoffmann’s sign | back 535 c. Chaddock’s sign |
front 536 downward pressure along the shin causes the big toe to
a. Abdominal superficial reflex b. Oppenhiem’s sign c. Chaddock’s sign d. Hoffmann’s sign | back 536 b. Oppenhiem’s sign |
front 537 the patient’s hand is pronated, and the Doc grabs the terminal
| back 537 Hoffmann’s sign |
front 538 ability to identify a number “written” in the palm of one’s hand: a. Graphesthesia b. Stereognosis c. diadochokinetic d. Romberg | back 538 a. Graphesthesia |
front 539 Graphesthesia indicates an issue in what lobe? | back 539 parietal |
front 540 Have the pt attempt to identify and object a. Graphesthesia b. Stereognosis c. Diadochokinetic d. Romberg | back 540 b. Stereognosis |
front 541 which one is parietal and occipital lobe issue? a. Graphesthesia b. Stereognosis c. Diadochokinetic d. Romberg | back 541 b. Stereognosis |
front 542 adiadochokinetic vs diadochokinetic | back 542 too little vs too much in rapid alternating movements |
front 543 A patient with severe cerebral hemispheric injury develops abnormal
flexion of the upper extremities with extension of the lower
extremities. This posture is called: | back 543 B. Decorticate posturing |
front 544 Pt with midbrain or pons lesions have: | back 544 B. Decerebrate posture |
front 545 A 68-year-old man with severe COPD reports fatigue, worsening dyspnea, and a 20-lb unintentional weight loss over the past 10 months. His BMI remains within the normal range. The physician is concerned about nutritional status and pulmonary prognosis. Which of the following statements best explains the nutritional risk in this patient? A. COPD patients losing ≥15% weight risk malnutrition | back 545 A. COPD patients losing ≥15% weight risk malnutrition |
front 546 Which measure best reflects lean body mass and correlates with pulmonary prognostic markers such as six-minute walk distance, dyspnea, predicted FEV₁, airway obstruction, lung hyperinflation, and total lung capacity? A. Body mass index | back 546 B. Fat-free mass index |
front 547 A COPD patient has a normal body weight but reduced skeletal muscle strength and poor exercise tolerance. Imaging shows reduced lean tissue mass despite stable total body weight. Which explanation best accounts for this finding? A. Increased adipose storage masks muscle loss | back 547 B. Fat-free mass depletion reduces peripheral muscle strength |
front 548 Which physiologic function most directly depends on adequate nutritional intake in COPD patients? A. Surfactant synthesis and exercise capacity | back 548 C. Respiratory muscle strength and exercise capacity |
front 549 Which mechanism best explains the increased susceptibility to respiratory infections in nutritionally depleted COPD patients? A. Increased airway smooth muscle tone and mucosal
resistance | back 549 C. Decreased cell-mediated immunity and mucosal resistance |
front 550 Which combination best represents antioxidant nutrients linked to improved lung function? A. Vitamin A, zinc, copper, folate | back 550 B. Vitamin C, vitamin E, β-carotene, selenium |
front 551 Investigators note that individuals with diets rich in tea, fruits, vegetables, and whole grains show improved lung function and slower disease progression. These foods likely benefit COPD patients primarily because they are: A. High in antioxidants with protective pulmonary effects | back 551 A. High in antioxidants with protective pulmonary effects |
front 552 Laboratory testing reveals increased oxidative stress within airway tissues. Which mechanism best explains these findings? A. Excess nitric oxide suppressing macrophages | back 552 B. Imbalance between reactive oxygen species and antioxidants |
front 553 A patient with advanced COPD reports decreased food intake despite access to adequate food. He states he simply does not feel hungry most of the time. Which factor most directly explains this contributor to weight loss? A. Reduced appetite | back 553 A. Reduced appetite |
front 554 A COPD patient complains that constant coughing and sputum production make eating unpleasant and difficult. Which mechanism best explains this effect on nutrition? A. Increased gastric motility and swallowing difficulty | back 554 B. Altered taste and swallowing difficulty |
front 555 A patient with severe COPD lives alone and reports difficulty maintaining adequate nutrition. He states that preparing meals makes him short of breath and extremely tired. Which COPD-related factor most directly contributes to his weight loss? A. Dyspnea and fatigue limiting food preparation | back 555 A. Dyspnea and fatigue limiting food preparation |
front 556 A COPD patient with persistent sadness and loss of interest in normal activities reports a reduced desire to eat and progressive weight loss. Which factor best explains this mechanism? A. Hyperthyroidism | back 556 B. Depression causing anorexia |
front 557 A patient with advanced COPD reports feeling full after only a few bites of food and sometimes has difficulty swallowing. Examination reveals severe lung hyperinflation. Which mechanism best explains this symptom? A. Lung hyperinflation compressing abdominal organs | back 557 A. Lung hyperinflation compressing abdominal organs |
front 558 Which cytokine most directly contributes to weight loss, muscle loss, and increased resting energy requirements in COPD? A. Tumor necrosis factor-α | back 558 A. Tumor necrosis factor-α |
front 559 A COPD patient with severe muscle wasting undergoes endocrine evaluation. Laboratory studies reveal low circulating leptin and testosterone levels. Which metabolic effect best explains the muscle loss observed in this patient? A. Increased protein synthesis | back 559 B. Increased protein catabolism |
front 560 A cachectic patient with severe COPD has elevated circulating growth hormone levels but persistent muscle wasting and metabolic dysfunction. Which mechanism best explains this paradox? A. Increased insulin resistance | back 560 B. Growth hormone resistance |
front 561 A patient with advanced COPD reports severe fatigue and early muscle exhaustion during minimal exertion. Laboratory studies show reduced phosphocreatine stores in skeletal muscle. Which metabolic consequence most directly explains the exercise intolerance? A. Reduced mitochondrial respiration | back 561 B. Early lactic acidosis |
front 562 A researcher studying severe COPD finds abnormalities in the metabolism of a branched-chain amino acid critical for muscle protein synthesis. Which amino acid is most likely involved? A. Valine | back 562 C. Leucine |
front 563 Certain electrolytes (calcium, magnesium, potassium and phosphorus) are especially important because depletion may contribute to the impairment of ______ muscle function. | back 563 respiratory |
front 564 When severely undernourished COPD patients are rapidly re-fed with glucose infusions, careful attention must be paid to these electrolytes to avoid ______ ______ | back 564 refeeding syndrome |
front 565 ghrelin improves body composition by decreasing muscle ______. | back 565 wasting |
front 566 A nutrition plan is being designed for a patient with COPD and chronic systemic inflammation. Which dietary lipid pattern is least desirable because it may promote a proinflammatory state and worsen inflammatory burden? A. High omega-6 PUFA intake | back 566 A. High omega-6 PUFA intake |
front 567 A clinician modifies a COPD patient’s diet to reduce inflammation by replacing one class of polyunsaturated fatty acids with less bioactive fats derived from fish oils. Which change best reflects this strategy? A. Replace omega-3 with omega-6 | back 567 B. Replace omega-6 with omega-3 |
front 568 assess ______ as a predictor of mortality | back 568 albumin |
front 569 Which statement best explains why immunosuppressive drugs can significantly affect nutrition management? A. They alter metabolism and intake | back 569 A. They alter metabolism and intake |
front 570 A patient taking cyclosporine develops hyperkalemia with elevated serum cholesterol and triglyceride levels. Which dietary modification is most appropriate? A. Reduce potassium, saturated fat, cholesterol | back 570 A. Reduce potassium, saturated fat, cholesterol |
front 571 A transplant patient is switched from cyclosporine to tacrolimus. Which metabolic complication should the care team monitor most closely? A. Hyperkalemia | back 571 B. Hyperglycemia |
front 572 A patient taking azathioprine complains of poor intake because of persistent gastrointestinal upset. Which adverse-effect combination is most characteristic of this drug? A. Constipation, dry mouth, bloating | back 572 B. Nausea, vomiting, diarrhea |
front 573 A patient receiving mycophenolate mofetil reports chronic loose stools and upper abdominal discomfort. Which adverse-effect pair best matches this medication? A. Diarrhea and dyspepsia | back 573 A. Diarrhea and dyspepsia |
front 574 Which nutritional consequence is most strongly associated with corticosteroid therapy? A. Hyperglycemia with obesity risk | back 574 A. Hyperglycemia with obesity risk |
front 575 While palpating the carotid artery of a healthy patient, the examiner notes a smooth contour with an upward stroke that is steeper and more rapid than the downward stroke. Which pulse description is most accurate? A. Normal pulse | back 575 A. Normal pulse |
front 576 A frail patient with low cardiac output has a carotid pulse that feels small and weak. The examiner notes only a gentle pressure rise before reaching a distinct peak. Which pulse type is present? A. Normal pulse | back 576 B. Diminished pulse |
front 577 During carotid palpation, the examiner feels a large, strong, hyperkinetic pulse with a rapid rise of the ascending limb and a quick sharp tap at the peak. Which pulse type best matches this finding? A. Normal pulse | back 577 C. Increased pulse |
front 578 A patient’s carotid waveform is described as having a prominent percussion wave and tidal wave, with or without an additional dicrotic wave. Which pulse description is most accurate? A. Normal pulse | back 578 D. Double-peaked pulse |
front 579 A clinician evaluating a patient’s pulse explains that cardiac rhythm on physical exam can be broadly described using which 3 categories? A. Regular, regularly irregular, irregularly irregular | back 579 A. Regular, regularly irregular, irregularly irregular |
front 580 A patient’s pulse is irregular, but the irregularity repeats in a definite, predictable pattern on palpation. Which rhythm description is most accurate? A. Regular | back 580 B. Regularly irregular |
front 581 A patient’s pulse has no repeating pattern whatsoever, with grossly variable intervals between beats. Which rhythm description best fits this finding? A. Regular | back 581 C. Irregularly irregular |
front 582 A medical student tries to classify an abnormal pulse only by palpation. The attending says the best method to definitively diagnose the rhythm is: A. Carotid auscultation | back 582 C. Electrocardiography |
front 583 Which finding is most consistent with premature beats? A. Completely random pauses only | back 583 B. Isolated extra beats in regular rhythm |
front 584 A patient has a coupled rhythm in which beats occur in pairs. The first beat is a sinus beat, followed by a premature beat that is usually ventricular. This pattern is called: A. Trigeminy | back 584 B. Bigeminy |
front 585 A premature beat occurs very early in diastole. When assessing the rhythm only by palpation, what pitfall may occur? A. The sinus beat feels exaggerated | back 585 B. The premature beat may be missed |
front 586 A patient has a grossly irregular pulse with no detectable pattern on physical exam. Which arrhythmia is classically associated with this finding? A. Atrial fibrillation | back 586 A. Atrial fibrillation |
front 587 A dermatology student is reviewing the structure of the skin. Which layer contains keratin-producing cells that undergo maturation, keratinization, and shedding in a cycle that takes approximately 4 weeks? A. Epidermis | back 587 A. Epidermis |
front 588 A patient presents with a deep skin laceration that disrupts the dense connective tissue stroma containing sensory and autonomic nerve fibers and forming the bulk of the skin. Which layer has most likely been damaged? A. Epidermis | back 588 B. Dermis |
front 589 A surgeon makes an incision deep enough to reach the third layer of skin composed largely of fatty connective tissue that cushions underlying structures. Which layer is this? A. Epidermis | back 589 C. Subcutaneous tissue |
front 590 A patient presents with excessive sweating of the palms and soles during stress. Which sweat glands are primarily responsible for this pattern of secretion? A. Apocrine glands | back 590 B. Eccrine glands |
front 591 A clinician explains that certain sweat glands are larger and mainly located in the axillae, areolae, pubic region, and perineum. Which glands are being described? A. Eccrine glands | back 591 C. Apocrine glands |
front 592 A teenager with acne has overactivity of glands associated with hair follicles that produce an oily secretion called sebum and are distributed across most of the body. Which glands are involved? A. Eccrine glands | back 592 C. Sebaceous glands |
front 593 During a nail exam, a clinician points to the whitish semilunar area at the base of the nail plate that represents proliferating epithelial cells from the nail matrix. What is this structure called? A. Cuticle | back 593 B. Lunula |
front 594 A patient develops goosebumps in response to cold exposure. Which muscle attached to the hair follicle below the sebaceous gland is responsible for this reaction? A. Arrector pili | back 594 A. Arrector pili |
front 595 A patient complains of generalized itching without a visible rash. The clinician explains that pruritus may indicate either a skin condition or: A. Vitamin deficiency only | back 595 B. Internal systemic illness |
front 596 A patient’s nails show splitting, discoloration, ridging, thickening, and separation from the nail bed. These findings are best described as: A. Nail hypertrophy only | back 596 C. Nail abnormalities or dystrophy |
front 597 A dermatology resident explains that many skin diseases cannot be cured directly and treatment often focuses on symptom relief rather than elimination of the underlying cause. This approach is called: A. Preventive treatment | back 597 C. Palliative therapy |
front 598 A patient develops recurrent rashes during periods of intense psychological stress. Which factor most likely contributes to this skin reaction? A. Viral activation only | back 598 B. Anxiety as a stressor |
front 599 What is true? A. Moisture occurs only in infections | back 599 B. Moisture may occur with fever or emotions |
front 600 dystrophic state in which the nail plate thins & a
cuplike a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 600 d. koilonychia |
front 601 Most commonly associated with iron deficiency anemia: a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 601 d. koilonychia |
front 602 Entirely white except for a band of pink at the distal tip: a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 602 a. terry's nails |
front 603 also called “half-and-half nails” a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 603 b. lindsay's nails |
front 604 blood spots that appear underneath the nail a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 604 c. splinter hemorrhages |
front 605 Presence is most often related to local, light trauma: a. terry's nails b. lindsay's nails c. splinter hemorrhages d. koilonychia | back 605 c. splinter hemorrhages |
front 606 white transverse line or band that result from poisoning or a. terry's nails b. lindsay's nails c. beau's lines d. mees' bands | back 606 d. mees' bands |
front 607 transverse grooves or depressions parallel to the lunula a. terry's nails b. lindsay's nails c. beau's lines d. mees' bands | back 607 c. beau's lines |
front 608  what is this? | back 608 common wart |
front 609 A patient presents with a small rough growth on the finger. The clinician explains it is a common wart. Which definition best describes a common wart? A. Malignant dermal tumor from UV damage | back 609 B. Benign epidermal growth caused by HPV |
front 610 A child develops several warts after sharing towels with a classmate who also had warts. What is the most likely mode of transmission? A. Airborne droplets only | back 610 C. Person-to-person contact |
front 611 On physical examination, a wart on the hand is palpated and appears as a firm raised lesion with a rough keratinized surface. Which description best matches the classic morphology of a wart? A. Soft papule with smooth surface | back 611 B. Firm nodule with rough keratinous surface |
front 612 A patient undergoes surgical treatment for a common wart. Because the lesion is confined to the epidermis, which surgical approach is typically sufficient for complete removal? A. Excision to level of dermis | back 612 A. Excision to level of dermis |
front 613  is this squamous or basal? | back 613 squamous |
front 614  is this squamous or basal? | back 614 basal |
front 615 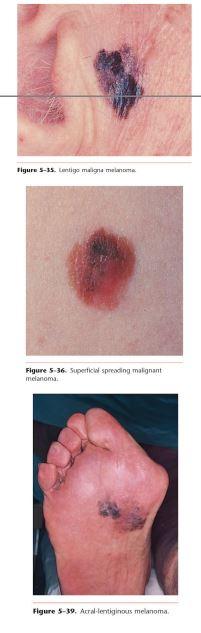 what is this? | back 615 melanoma |
front 616 A biopsy from a sun-exposed skin lesion shows a malignant neoplasm of keratinocytes arising in the epidermis with local invasion into the dermis. Which diagnosis is most likely? A. Basal cell carcinoma | back 616 B. Squamous cell carcinoma |
front 617 A skin lesion presents as a scaling, crusting nodule that intermittently ulcerates and bleeds. Which diagnosis is most consistent with this morphology? A. Basal cell carcinoma | back 617 B. Squamous cell carcinoma |
front 618 A clinician evaluates a cutaneous malignancy that developed mainly on chronically sun-exposed skin. Which diagnosis is most strongly associated with predominant development on skin exposed to sunlight? A. Squamous cell carcinoma | back 618 A. Squamous cell carcinoma |
front 619 A malignant skin lesion is diagnosed as a neoplasm of basal cells of the epidermis and is noted to be the most common skin malignancy. Which diagnosis is this? A. Squamous cell carcinoma | back 619 B. Basal cell carcinoma |
front 620 A pearly skin lesion with a rolled, well-defined border and a central ulcerated depression is found on the face. Which diagnosis is most likely? A. Basal cell carcinoma | back 620 A. Basal cell carcinoma |
front 621 Which feature best distinguishes basal cell carcinoma from squamous cell carcinoma? A. Rapid growth with frequent metastasis | back 621 D. Slow growth with rare metastasis |
front 622 A biopsy from a deeply pigmented skin lesion shows a malignant neoplasm of melanocytes in the epidermis. Which diagnosis is most likely? A. Basal cell carcinoma | back 622 C. Melanoma |
front 623 Which statement best characterizes the epidemiology and prognosis of melanoma? A. It is uncommon and rarely fatal | back 623 C. It is uncommon but highly fatal |
front 624 A dermatologist notes that melanoma incidence has been: | back 624 B. Increasing faster than other malignancies |
front 625 Which skin finding is most consistent with the usual pigmentation pattern of melanoma? A. Flesh-colored translucent papule | back 625 C. Varied black, blue, brown lesion |
front 626 Which melanoma subtype is frequently seen in geriatric patients and appears in areas of sun-exposed, sun-damaged skin? A. Nodular melanoma | back 626 B. Lentigo maligna melanoma |
front 627 A lesion is diagnosed as the most common type of melanoma, accounting for about 70% of all cases, and appears as an irregularly colored plaque with sharp notches and variegated pigmentation. Which subtype is this? A. Lentigo maligna melanoma | back 627 D. Superficial spreading melanoma |
front 628 Which melanoma subtype carries an excellent prognosis if diagnosed early? A. Superficial spreading melanoma | back 628 A. Superficial spreading melanoma |
front 629 A dark blue-black skin lesion has grown rapidly over several months. It represents the second most common melanoma subtype, comprising about 15% of cases. Which diagnosis is most likely? A. Lentigo maligna melanoma | back 629 B. Nodular melanoma |
front 630 Which melanoma subtype is the most common form seen in African Americans and Asians and occurs on non-hair-bearing parts of the body? A. Nodular melanoma | back 630 C. Acral-lentiginous melanoma |
front 631 In white individuals, melanomas tend to occur predominantly: | back 631 C. In the lower extremities and back |
front 632 Which melanoma locations are associated with a worse prognosis than lesions on the extremities? A. Face, ears, eyelids | back 632 B. Back, axillae, neck, scalp |
front 633 Melanoma occurs more often after which sun-exposure pattern in fair-skinned individuals? A. Chronic occupational sun exposure | back 633 B. Brief intense sun exposure |
front 634 Less than 5% of all melanomas occur in: | back 634 C. African-American patients |
front 635  Cafe-au-lait spots, contact dermatitis, lipoma, neurofibroma? | back 635 contact dermatitis |
front 636  Cafe-au-lait spots, contact dermatitis, lipoma, neurofibroma? | back 636 lipoma |
front 637  Cafe-au-lait spots, contact dermatitis, lipoma, neurofibroma? | back 637 Cafe-au-lait spots |
front 638  Cafe-au-lait spots, contact dermatitis, lipoma, neurofibroma? | back 638 neurofibroma |
front 639 A patient presents with a soft-tissue mass under the skin that feels rubbery and is composed of benign subcutaneous fat. Which diagnosis is most likely? A. Neurofibroma | back 639 B. Lipoma |
front 640 Which statement best describes a lipoma? A. Malignant tumor of adipose tissue | back 640 C. Common benign subcutaneous fat growth |
front 641 A child is noted to have several flat, well-circumscribed brown patches on the trunk. Which lesion best matches this description? A. Cafe-au-lait spots | back 641 A. Cafe-au-lait spots |
front 642 Cafe-au-lait spots result from: | back 642 B. Increased hyperactive melanocytes |
front 643 An adult is found to have 7 cafe-au-lait spots, each measuring 2 cm
in diameter. This finding should raise concern for: | back 643 C. Neurofibromatosis |
front 644 A dermal tumor produced by focal proliferation of neural tissue with
a normal overlying epidermis is called: | back 644 B. Neurofibroma |
front 645 Which feature best distinguishes a neurofibroma from many other skin
tumors? | back 645 B. The epidermis remains normal |
front 646 On palpation, cutaneous neurofibromas are typically: | back 646 C. Soft in consistency |
front 647  What is this? contact dermatitis, tinea corporis, psoriasis, onychomycosis | back 647 psoriasis |
front 648  What is this? contact dermatitis, tinea corporis, psoriasis, onychomycosis | back 648 tinea corporis |
front 649  What is this? contact dermatitis, tinea corporis, psoriasis, onychomycosis | back 649 onychomycosis |
front 650 The underlying dermis displays mild inflammation: contact dermatitis, fungal infections, psoriasis, onychomycosis | back 650 fungal infections |
front 651 A patient presents with a chronic noninfectious skin disorder that often runs in families and may also affect the joints and nails. Which condition best fits this description? A. Psoriasis | back 651 A. Psoriasis |
front 652 A patient with psoriasis presents with sharply demarcated plaques that are slightly raised and covered with thick scale due to excess keratin production. Which description best characterizes these lesions? A. Vesicular plaques with crusting | back 652 B. Well-defined hyperkeratotic plaques |
front 653 A patient with psoriasis complains of severe itching and symmetric lesions. Which body locations are most characteristically involved? A. Palms, soles, eyelids | back 653 C. Elbows, knees, scalp, intergluteal cleft |
front 654 Dermatophyte infections affecting the skin, hair, and nails most commonly belong to which genera? A. Candida, Aspergillus, Cryptococcus | back 654 B. Trichophyton, Microsporum, Epidermophyton |
front 655 What does the term “tinea” specifically indicate? A. Bacterial infection | back 655 C. Fungal cause |
front 656 A patient presents with a fungal infection in which organisms invade the nail bed. This condition is also noted to be the most common nail disorder. Which diagnosis is most likely? A. Psoriatic nail disease | back 656 B. Onychomycosis |
front 657 A patient with onychomycosis notices gradual worsening of the nail over time. Which set of nail changes is most characteristic? A. Color, structure, texture changes | back 657 A. Color, structure, texture changes |
front 658 Inflammation of the nail bed in onychomycosis promotes: | back 658 B. Hyperkeratosis and thickening |
front 659  What is this? Herpesvirus, Pityriasis rosea, Herpes zoster, Acne | back 659 Pityriasis rosea |
front 660  What is this? Herpesvirus, Pityriasis rosea, Herpes zoster, Acne | back 660 Herpes zoster |
front 661  What is this? Herpesvirus, Pityriasis rosea, Herpes zoster, Acne, tinea versicolor | back 661 Acne |
front 662  what is this? Herpesvirus, ganglion cyst, Pityriasis rosea, Herpes zoster, Acne, tinea versicolor | back 662 ganglion cyst |
front 663  what is this? Herpesvirus, ganglion cyst, Pityriasis rosea, Herpes zoster, Acne, tinea versicolor, | back 663 tinea versicolor |
front 664 A 22-year-old patient presents with a common, acute, self-limiting inflammatory skin disease of unknown cause that typically appears during the spring. Which diagnosis best matches this description? A. Pityriasis rosea | back 664 A. Pityriasis rosea |
front 665 A patient develops a widespread rash that was preceded several days earlier by a single lesion resembling tinea corporis. What is this initial lesion called? A. Sentinel lesion | back 665 B. Herald patch |
front 666 A patient diagnosed with pityriasis rosea asks how long the rash will last. The clinician explains that the condition usually persists for approximately: A. 1–2 days | back 666 C. 3–6 weeks |
front 667 A patient presents with shingles, characterized by a painful vesicular eruption following a dermatomal distribution. Which diagnosis best fits this condition? A. Psoriasis | back 667 B. Herpes zoster |
front 668 The underlying cause of herpes zoster is the reactivation of which virus? A. Herpes simplex virus | back 668 C. Varicella-zoster virus |
front 669 Herpesvirus infections are commonly encountered in which group of patients? A. Patients with HIV infection | back 669 A. Patients with HIV infection |
front 670 In patients with HIV, the presence of herpesvirus infections is thought to be: A. Protective against opportunistic infections | back 670 B. Predictive of future progression to AIDS |
front 671 The likelihood of herpesvirus infection becomes extremely high when CD4+ T-cell counts drop below which threshold? A. 500 cells/mm³ | back 671 D. 100 cells/mm³ |
front 672 Acne is best described as which type of disease? A. Viral disease of sweat glands and sebaceous glands | back 672 B. Pustular disease of hair follicles and sebaceous glands |
front 673 Which lesions are considered the primary lesions in acne? A. Vesicles, bullae, plaques | back 673 B. Pustules, papules, comedones |
front 674 Within the dermis in acne, the hair follicle becomes occluded by a collection of: A. Melanin, collagen, lymphocytes | back 674 B. Keratin, sebum, inflammatory cells |
front 675 A patient presents with a chronic, painless lesion on the dorsum of the wrist that is fluctuant and cystic. Which diagnosis best fits this description? A. Lipoma | back 675 B. Ganglion cyst |
front 676 A ganglion cyst develops because of leakage of which substance through the tendon sheath of a joint capsule? A. Lymphatic fluid | back 676 B. Synovial fluid |
front 677 The name “Bible cyst” originated from a historical treatment method in which clinicians attempted to rupture the cyst by: A. Freezing the lesion with ice | back 677 B. Striking it with a Bible or large book |
front 678 When multiple small ganglion cysts appear near one another, they may look like separate lesions but are usually connected by: A. Shared epidermal tract | back 678 C. Common deep tissue stalk |
front 679 A small pale red skin lesion with a pulsating central arteriole and radiating “legs” is identified on the upper chest. What is the most likely diagnosis? A. Telangiectasia | back 679 B. Spider angioma |
front 680 Spider angiomas are most commonly found on which body areas? A. Face, neck, arms, upper trunk | back 680 A. Face, neck, arms, upper trunk |
front 681 Spider angiomas are more commonly associated with which patient populations? A. Children and athletes | back 681 C. Pregnant women and liver disease |
front 682  Vitiligo, Scabies, Urticaria, Insect bites, Pyoderma gangrenosum, Erythema multiforme | back 682 Vitiligo |
front 683  Vitiligo, Scabies, Urticaria, Insect bites, Pyoderma gangrenosum, Erythema multiforme, Karposi’s sarcoma | back 683 Urticaria |
front 684  Vitiligo, Scabies, Urticaria, Insect bites, Pyoderma gangrenosum, Erythema multiforme, Karposi’s sarcoma | back 684 Erythema multiforme |
front 685  Karposi’s sarcoma, Vitiligo, Scabies, Urticaria, Insect bites, Pyoderma gangrenosum, Erythema multiforme, Norwegian scabies | back 685 Scabies |
front 686  Vitiligo, Scabies, Urticaria, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Erythema multiforme, Karposi’s sarcoma | back 686 Norwegian scabies |
front 687  Vitiligo, Scabies, Urticaria, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Karposi’s sarcoma, Erythema multiforme | back 687 Pyoderma gangrenosum |
front 688  Vitiligo, Scabies, Urticaria, Karposi’s sarcoma, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Erythema multiforme | back 688 Insect bites |
front 689  Vitiligo, Scabies, Urticaria, Karposi’s sarcoma, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Erythema multiforme | back 689 Karposi’s sarcoma |
front 690 Vitiligo lesions are best described morphologically as: A. Large macules that are totally depigmented | back 690 A. Large macules that are totally depigmented |
front 691 A patient with urticaria develops transient wheals after exposure to an allergen. Which mechanism most directly causes the dermal edema seen in this condition? A. Keratin overproduction in epidermis | back 691 B. Release of histamine increasing vascular permeability |
front 692 A patient develops an immunologic skin reaction with lesions triggered by infection or medications. The rash contains several lesion types including papules, bullae, plaques, and distinctive target-shaped lesions. Which diagnosis best fits this presentation? A. Psoriasis | back 692 B. Erythema multiforme |
front 693 Erythema multiforme: A. Intraepidermal vesicle separation with papillary
inflammation | back 693 C. Subepidermal separation with papillary inflammation |
front 694 The condition involves mucous membranes and represents the most severe form associated with erythema multiforme. What is this condition called? A. Toxic epidermal necrolysis | back 694 B. Stevens–Johnson syndrome |
front 695 Scabbies physical finding? A. Vesicular plaque | back 695 C. Burrow |
front 696 symptoms appear faster in norweigen or normal scabbies? | back 696 norweigen |
front 697 norweigen scabbies has (less/more) itching than normal scabbies? | back 697 less |
front 698 Neglected personal hygiene & impaired immune system lead to: A. Psoriasis | back 698 D. Norweigen Scabbies |
front 699 Pyoderma gangrenosum is associated with what gastric issue? | back 699 IBS |
front 700 Pyoderma gangrenosum: male or female more? | back 700 female |
front 701 The classic form of the disease is a RARE, slow-growing neoplasm occurring mostly on the lower extremities: Vitiligo, Scabies, Urticaria, Karposi’s sarcoma, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Erythema multiforme | back 701 Karposi’s sarcoma |
front 702 More common in older men of Mediterranean or Jewish eastern European descent: Vitiligo, Scabies, Urticaria, Karposi’s sarcoma, Norwegian scabies, Insect bites, Pyoderma gangrenosum, Erythema multiforme | back 702 Karposi’s sarcoma |
front 703 true or false: Some patients with classic KS may develop another type of cancer before the KS lesions appear or even later in life | back 703 true |
front 704 true or false: The risk of developing KS is closely linked to the CD8+ count. | back 704 false cd4+ |
front 705 KS: Average length of patient survival from the onset of the disease is ____ months | back 705 18 |
front 706  Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 706 Seborrheic dermatitis |
front 707  Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 707 Erythema nodosum |
front 708  Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 708 Lichen planus |
front 709  Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 709 Seborrheic warts |
front 710  Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 710 Scleroderma |
front 711 A patient with progressive systemic sclerosis develops skin tightening and multiorgan involvement due to the fundamental pathologic process underlying the disease. Which change best explains the symptoms of scleroderma? A. Buildup of collagen in skin and organs | back 711 A. Buildup of collagen in skin and organs |
front 712 A woman with long-standing scleroderma is found to have stony-hard nodules in the soft tissues of her hands. Which process best explains this finding? A. Fat necrosis | back 712 B. Soft tissue calcification |
front 713 In scleroderma, which vascular abnormality is most associated with visceral involvement? A. Large-vein thrombosis and small artery changes | back 713 C. Microvessel and small artery changes |
front 714 A patient presents with tender erythematous subcutaneous nodules that are symmetrically distributed on both shins. Which diagnosis is most likely? A. Erythema nodosum | back 714 A. Erythema nodosum |
front 715 The pathogenesis of erythema nodosum is most strongly associated with which immune mechanism? A. Type I immediate hypersensitivity | back 715 D. Type IV delayed hypersensitivity |
front 716 A patient with erythema nodosum develops lesions that are initially flat, firm, hot, red, and painful. Which description best matches the early morphology? A. Flat firm hot painful lumps | back 716 A. Flat firm hot painful lumps |
front 717 After appearing, lesions of erythema nodosum typically begin to regress after: A. 1 to 2 days | back 717 B. 1 to 2 weeks |
front 718 Patient usually experiences severe pain as the lesions ulcerate: Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 718 Lichen planus |
front 719 greasy-looking scale in a seborrheic distribution, associated with HIV infection: Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 719 Seborrheic dermatitis |
front 720 failure of keratinocytes to mature normally: Erythema nodosum, Scleroderma, Lichen planus, Seborrheic warts, Seborrheic dermatitis | back 720 Seborrheic warts |
front 721  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 721 keloid |
front 722  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 722 Nevi |
front 723  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 723 Pemphigus vulgaris |
front 724  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 724 Bullous pemphigoid |
front 725  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 725 Atopic dermatitis |
front 726  nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 726 Erythema migrans |
front 727  Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 727 Bullous diabeticorum |
front 728  Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 728 Anthrax |
front 729  Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 729 Cutaneous larva migrans |
front 730  Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 730 Tuberous sclerosis |
front 731  Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 731 Smallpox |
front 732 hyperproliferative response of fibrous tissue to injury,
inflammation, or nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 732 keloid |
front 733 Disease is caused by the production of antibodies to the
intercellular nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 733 Pemphigus vulgaris |
front 734 No racial predilection, & the disease is NOT as serious as pemphigus nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 734 Bullous pemphigoid |
front 735 form of eczema; common disease associated with other nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 735 Atopic dermatitis |
front 736 many patients have elevated levels of serum IgE: nelvi, keloid, Pemphigus vulgaris, Atopic dermatitis, Bullous pemphigoid, Erythema migrans, Bullous diabeticorum | back 736 Atopic dermatitis |
front 737 occurs in patients with long-standing diabetes: Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 737 Bullous diabeticorum |
front 738 Topical application of thiabendazole is the treatment: Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 738 Cutaneous larva migrans |
front 739 rapid progression of high fever, severe respiratory distress,
& Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 739 Anthrax |
front 740 distinctive erythematous, vesicular rash, centrifugal in distribution: Tuberous sclerosis, Anthrax, Bullous diabeticorum, Cutaneous larva migrans, Smallpox | back 740 Smallpox |