Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Abnormal Psych Exam 3
front 1 Priyanka is highly restrictive of her calorie intake and exercises vigorously each day. Despite having a severely low body weight, Priyanka believes she is overweight and needs to continue losing weight. When Priyanka goes to a doctor, she is MOST likely to be diagnosed with | back 1 Anorexia nervosa |
front 2 Mel has been diagnosed with anorexia nervosa. His body weight is
15 | back 2 Restricting |
front 3 Research indicates that approximately _____ percent of individuals
who struggle | back 3 25% |
front 4 Which of the following symptoms is NOT characteristic of anorexia nervosa? | back 4 lack of interest in food (symptoms: distorted body image, amenorrhea, fear of gaining weight) |
front 5 Research indicates that approximately _____ percent of individuals
who struggle | back 5 75% |
front 6 Which of the following symptoms is characteristic of bulimia nervosa
but is NOT | back 6 concern about pleasing others (distorted body perception, disturbed eating attitudes, feelings of anxiety, depression, obsessiveness, and perfectionism) |
front 7 Which of the following is true about the prevalence rates of anorexia nervosa (AN), bulimia nervosa (BN), and binge-eating disorder (BED)? | back 7 BED>BN>AN |
front 8 Which of these is NOT true about anorexia nervosa, bulimia nervosa, and binge-eating disorder? | back 8 The age of onset is typically over the age of 20 |
front 9 Relatives of people with eating disorders are up to _____ times more likely to develop one of these disorders themselves. | back 9 6 |
front 10 While many individuals with anorexia nervosa benefit from treatment, studies indicate that this disorder continues to be a chronic, serious problem for at least _____ percent of these people, even after treatment. | back 10 20% |
front 11 The drugs receiving the most attention recently for reducing binge
eating and | back 11 antidepressants |
front 12 Treatment is shown to provide immediate, significant improvement in about _____ of cases of bulimia nervosa. | back 12 40% |
front 13 What are some key features of an Anorexia Nervosa diagnosis? | back 13 The individual purposely takes in too little food, resulting in a low BMI, fear of gaining weight, and seeks to prevent it, distorted body perception, and places inappropriate emphasis on weight or shape in self-judgements or does not consider the implications of their low weight |
front 14 What are the two main subtypes of Anorexia Nervosa? | back 14 Restricting type and Binge-eating/purging type |
front 15 What are the traits of the restricting type | back 15 Lose weight by cutting out sweets and fattening snacks, and eventually eliminating all food. |
front 16 What are the traits of the binge-eating/purging type? | back 16 Lose weight by forcing themselves to vomit after meals or by abusing laxatives or diuretics. |
front 17 What are some key features of Bulimia Nervosa | back 17 Repeated binge-eating episodes, repeated performance of ill-advised compensatory behaviors to prevent weight gain (vomiting), symptoms take place at least weekly for 3 months, and inappropriate influence of weight and shape on appraisal of oneself. |
front 18 What are some key features of Binge-eating disorder to obtain a diagnosis? | back 18 Recurrent binge-eating episodes, binge eating episodes can contain at least three of these features ( really fast eating, absence of hunger, uncomfortably full, secret eating cause of shame, feelings of disgust, guilt, depressed, significant distress, binge eating episodes take place at least weekly over the course of 3 months, absence of excessive compensatory behaviors. |
front 19 What are the specifiers and their criteria for Anorexia Nervosa? | back 19 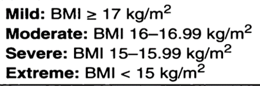 Severe and Extreme usually treated in hospital settings |
front 20 Escalation toward anorexia nervosa ______________________________________ | back 20 may follow a stressful event |
front 21 What are some key points about the clinical picture of anorexia nervosa? | back 21 - fear driving motivation - Thinking is distorted -potential psychological problems -substance misuse |
front 22 What are some medical problems that can occur as a result of anorexia nervosa? | back 22 Amenorrhea and Lanugo (thin hairs) |
front 23 In bulimia nervosa, weight is _____________________________________________ | back 23 Typically in the normal range, but can fluctuate. |
front 24 What are some similarities between anorexia and bulimia nervosa? | back 24 - DISTURBED EATING ATTITUDES - distorted body perception - fear of becoming obese -preoccupied with food, weight, and appearance |
front 25 What are some differences between anorexia and bulimia nervosa? | back 25 AMENORRHEA is LESS likely, different medical complications, dental problems more likely |
front 26 What are some key points about the Dx checklist for Binge-eating disorder. | back 26 - recurrent binge-eating episodes - episodes consist of at least three of these features (usually fast eating, absence of hunger, uncomfortably full, secret eating due to shame, feelings of disgust, depression, or guilt - significant distress -take place weekly over the course of 3 months - absence of excessive compensatory behaviors |
front 27 What are the specifiers for binge eating disorder? | back 27 Mild: 1-3 episodes per week Moderate: 4-7 episodes per week Severe: 8-13 episodes per week Extreme: 14 or more binge eating episodes per week |
front 28 What is the main cause of eating disorders? | back 28 Multidimensional risk perspective - more factors = greater likelihood of developing a disorder (psychodynamic, CB, biological, societal pressures, family environment, multicultural) |
front 29 Psychodynamic factors of eating disorders: | back 29 Ego deficiencies *Bruch: psychodynamic theory of eating disorders - disturbed mother-child interactions - People with eating disorders inaccurately perceive internal cues, including emotional cues, and are more likely to worry about how they are viewed by others. |
front 30 Cognitive-behavioral factors of ED's | back 30 - improper labeling of internal sensations and needs -Little control over life may result in excess control of body size. |
front 31 How does depression contribute to eating disorders? | back 31 Helps set the stage for eating disorders - Similar brain circuit abnormalities are involved in those with eating disorders and depression - Antidepressant drugs |
front 32 Biological factors of ED's | back 32 Genetics, brain circuit dysfunction, WEIGHT SET POINT - Larger and more active insula, orbitofrontal cortex, and striatum; smaller prefrontal cortex. |
front 33 How do societal pressures contribute to eating disorders? | back 33 - Western standards for female attractiveness - socially accepted prejudice against overweight people - social networking, internet activity, TV |
front 34 How does family environment contribute to eating disorders? | back 34 - History of emphasis on thinness, appearances, or dieting - Dieting and perfectionistic mothers |
front 35 What multicultural factors cause ED's ? | back 35 Racial and ethnic differences, Gender differences - Eating behaviors, values, and goals of women in minority groups in the United States were considerably healthier than those of non-Hispanic white American women |
front 36 What are the specifiers for bulimia nervosa? | back 36 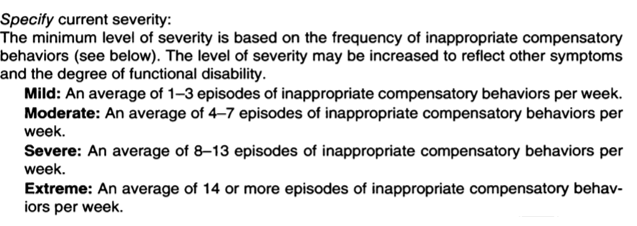 |
front 37 What is the Dx checklist for substance use disorders? | back 37 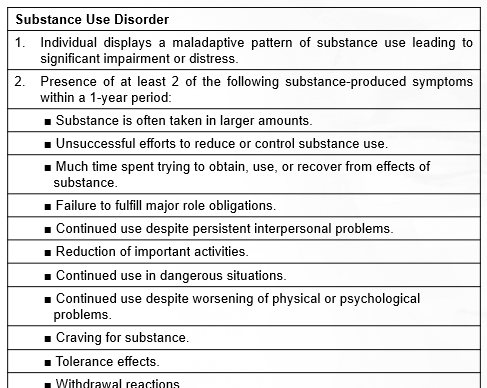 |
front 38 In any given year, ____ percent of all teens and adults in the United States, more than 20 million people, have a substance use disorder. | back 38 7.4 |
front 39 Only ____ percent of all those with substance use disorders receive treatment from a mental health professional. | back 39 18.4 |
front 40 What are some drugs that fall under depressants? | back 40 - alcohol - sedative/hypnotics anxiolytics (benzos, barbs) - opioids |
front 41 What are some examples of stimulants? | back 41 -caffeine - amphetamines (legals, meths) - cocaine |
front 42 What are some examples of hallucinogens? | back 42 MDMA, Ectasy, Molly, LSD |
front 43 What is the main example of cannabis? | back 43 THC, used recreationally typically, relaxing and stimulates. |
front 44 What is an important symptom of withdrawal, especially from prolonged use? | back 44 DTs, deliurium tremens |
front 45 What are the personal and social impacts of alcoholism? | back 45 - it destroys families, social relationships, and careers |
front 46 What are examples of opioids? | back 46 opium, heroin, morphine, codeine, methadone |
front 47 Medical opioids are: | back 47 morphine, codeine, oxycodone |
front 48 Why are opioids dangerous? | back 48 overdose, ignorance of tolerance, mixing with other substances |
front 49 What are the physical dangers of cocaine? | back 49 Overdose, death |
front 50 Hallucinogens produce- | back 50 powerful changes primarily in sensory perception, natural hallucinogens |
front 51 Effects of polysubstance use | back 51 Synergistic effects ( they add ) Antagonistic effects ( they counteract each other) |
front 52 What are the causes for substance-related disorders? | back 52 - sociocultural views - psychodynamic views - CB views - Bio views COMBINATION |
front 53 What is the sociocultural view of SUD | back 53 - people who live in socioeconomic conditions - families that value or tolerate drug use - other stress |
front 54 Psychodynamic views of SUD | back 54 -powerful early years dependency needs - display substance abuse personality |
front 55 CB views of SUD? | back 55 Operant conditioning by tension reduction, the rewarding effects of drugs all related to conditioning |
front 56 Bio views of SUD? | back 56 genetics, NTs, Pleasure Pathway * Incentive-sensitization theory * reward deficiency syndrome |
front 57 What are the types of treatments for SUD | back 57 Detox, antagonist drugs, and drug maintenance therapy. |
front 58 Antabuse is used for (antagonist) | back 58 Alcoholism |
front 59 Narcan is used for (antagonist) | back 59 Opioids |
front 60 Methadone is used for (drug maintenence therapy) | back 60 pain killers and heroin |
front 61 Cramps, anxiety attacks, sweating, and | back 61 Withdrawal |
front 62 Epidemiological studies indicate that ____ | back 62 7.4 |
front 63 Studies indicate that no more than _____ | back 63 20 |
front 64 Which racial or ethnic group has the lowest rates of substance use disorders | back 64 Asian americans |
front 65 What percentage of the American | back 65 25% |
front 66 Long-term excessive alcohol use can lead to____, a disease involving
memory loss, | back 66 Korsakoff's syndrome |
front 67 Despite long established links between | back 67 10% |
front 68 The sedative-hypnotic drugs Xanax, Ativan, and Valium are all classified as: | back 68 benzodiazepines |
front 69 Unlike the withdrawal symptoms that are | back 69 death |
front 70 Cocaine increases the available supplies of | back 70 acetylcholine |
front 71 Studies indicate that approximately 1 in | back 71 10 |
front 72 Opioids are an example of a | back 72 depressant |
front 73 Tolerance to stimulant drugs is in part | back 73 dopamine |
front 74 People are MOST likely to obtain | back 74 a friend or relative |
front 75 _________ is known as an increase of effects | back 75 A synergistic effect |
front 76 Teaching clients to identify high-risk | back 76 relapse-prevention training |