Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Developmental milestones
front 1 what are the 5 components/stages of child development, birth to 5 yrs? | back 1
|
front 2 what are the 5 components/stages of development in school-aged children, 5-18 yrs? | back 2
|
front 3 Play is the way the child learns what no one can | back 3 Occupation in a Young Child |
front 4 refers to activities that support the | back 4 occupation |
front 5 Occupation serves the basic needs of a __________ | back 5 baby |
front 6 What are the three basic levels of need in the “Baby Hierarchy of Needs”? | back 6
|
front 7 What are the basic things babies do? | back 7 Eat, sleep, poop, and explore. |
front 8 What do physical needs include for babies? | back 8 Eating, sleeping, and excretion. |
front 9 What do emotional and cognitive needs include for babies? | back 9 Exploration and interaction with their environment. |
front 10 What is one example of meeting a baby’s physical need for nutrition? | back 10 Providing healthy, age-appropriate food options. |
front 11 What is one example of meeting a baby’s physical need for sleep? | back 11 Offering a crib or playpen with comforting toys to promote rest. |
front 12 What is one example of meeting a baby’s physical need for movement? | back 12 Allowing indoor and outdoor exploration in safe environments. |
front 13 What is one example of meeting a baby’s physical need for comfort? | back 13 Ensuring a clean, safe, and healthy living space. |
front 14 What are examples of meeting babies’ physical needs? (4 things) | back 14
|
front 15 What are examples of meeting babies’ emotional needs? | back 15
|
front 16 What helps meet a baby’s emotional need for security? | back 16 Creating confidence to explore and develop autonomy. |
front 17 What helps meet a baby’s emotional need for bonding? | back 17 Ensuring the baby feels “heard” through physical touch and responsive interactions. |
front 18 What helps meet a baby’s emotional need for attachment? | back 18 Providing stable, consistent relationships. |
front 19 When do children typically form full attachments to parents? | back 19 Between ages 1 and 3 years. |
front 20 What helps meet a baby’s cognitive need for communication? | back 20 Encouraging interaction and social participation. |
front 21
| back 21 enriched environments |
front 22 What are the 3 main cognitive needs for babies? | back 22
|
front 23
| back 23 learning |
front 24 __________________ are created as babies seek to have | back 24 Occupations |
front 25 What are 4 examples of physical occupations in babies? | back 25
|
front 26 eating, self-feeding | back 26 nutrition |
front 27 physical occupations form the basis for ______________________________ | back 27 Activities of Daily Living (ADLs) |
front 28 rest, recuperation | back 28 sleep |
front 29 dressing, bathing, toileting | back 29 comfort |
front 30 interaction with the environment | back 30 movement |
front 31
| back 31 Emotional Occupations |
front 32 Meeting basic cognitive needs sets the foundation | back 32 Cognitive Occupations |
front 33 What are the 3 main cognitive occupations for babies? | back 33
|
front 34 What is the OT’s role with babies ages 1–3? | back 34 Partnering with babies and caregivers to improve occupational performance and competence in natural environments. |
front 35 What are the 4 key OT concepts when working with children? | back 35
|
front 36 What are the 5 essential concepts of OT intervention with children? | back 36
|
front 37 typical development- Knowledge of neurological,
physiological, | back 37 occupational performance |
front 38 Children develop on fairly _______________ timelines | back 38 predictable |
front 39 Progressions in development vary by many ____________________ | back 39 contextual factors |
front 40 What are the 4 main physical milestones at 1 year? | back 40
|
front 41 What are 4 typical feeding milestones for a 1-year-old? | back 41
|
front 42 Why is experimenting with utensils important? | back 42 It develops fine motor coordination and hand-to-mouth control. |
front 43 What are 5 typical social/emotional skills at 1 year? | back 43
|
front 44 What does stranger anxiety indicate? | back 44 The baby can now distinguish familiar people from strangers — a healthy developmental sign. |
front 45 What type of play is most common at 1 yr? | back 45 Social play with caregivers — early interactive play like peek-a-boo. |
front 46 What are 6 key language & communication milestones at 1 year? | back 46
|
front 47 What self-awareness behavior appears at 1 yr? | back 47 Recognizes self in a mirror. |
front 48 What communication skills show at 1 year? | back 48 Responds to facial expressions and smiles socially. |
front 49 at 1 yr old, what gesture shows desire for interaction? | back 49 Lifts arms to be picked up. |
front 50 What words usually emerge @ 1 yr? | back 50 “Mama,” “Dada,” and repeated simple words. |
front 51 1 Year – Language/Communication= observing others facial expressions | back 51 Eye contact |
front 52 1 Year – Language/Communication= regarding oneself in the mirror | back 52 Self-awareness |
front 53 1 Year – Language/Communication= in response to others | back 53 Social smile |
front 54 What physical transitions occur at 1 year? | back 54 Moves between lying, sitting, and standing. |
front 55 What new standing skill appears at 1 year? | back 55 Pulls to stand and begins cruising along furniture. |
front 56 What early walking skill appears @ 1 yr? | back 56 Experiments with standing and stepping. |
front 57 What physical goal drives this stage (@1 yr)? | back 57 Exploration and mobility. |
front 58 What feeding milestone occurs at 1 year? | back 58 Holds own bottle or sippy cup. |
front 59 When can solids be introduced @1 yr? | back 59 After head control and sitting balance develop. |
front 60 What self-feeding skill appears @1 yr? | back 60 Finger-feeds independently. |
front 61 What utensil skill develops @1 yr? | back 61 Experiments with spoon and cup (messy but intentional). |
front 62 What social milestone forms at 1 year? | back 62 Establishes trust with caregivers |
front 63 How does a 1-year-old share play? | back 63 Brings toys to caregiver. |
front 64 What social action is used for attention at 1 yr? | back 64 Repeats sounds or actions. |
front 65 What early game reflects social awareness? | back 65 Peek-a-boo. |
front 66 What are 7 cognitive skills seen at 1 year? | back 66
|
front 67 Learning through interacting with environment | back 67 Sensorimotor stage (birth to 2 years) |
front 68 Pretend play that uses objects to represent something else (e.g., pretending a block is a phone). | back 68 symbolic play |
front 69 What 2 physical red flags may indicate delay/are detectable risks @ 1 year? | back 69
|
front 70 What 2 social red flags may indicate delay/are detectable risks @ 1 year? | back 70
|
front 71 What 2 cognitive red flags may indicate delay/ are detectable risks @ 1 year? | back 71
|
front 72 What are 2 typical reasons for OT referral at 1 year? | back 72
|
front 73 What physical deficits might a 1-year-old with developmental delays show? (2 things) | back 73
|
front 74 What are signs of abnormal tone? | back 74 Too stiff (spastic) or too floppy (hypotonic) movements. |
front 75 What are feeding red flags for a 1-year-old? | back 75
|
front 76 what are 3 examples of poor oral motor control in a 1 year old? | back 76
|
front 77 What are 4 common diagnoses seen at 1 year that may require OT? | back 77
|
front 78
| back 78 Cerebral Palsy (CP) |
front 79 Is CP progressive or nonprogressive? | back 79 Nonprogressive — the brain injury doesn’t worsen, but its effects can change over time. |
front 80 What body systems does CP primarily affect? | back 80 The motor system — including movement, tone, and posture. |
front 81 How common is CP? | back 81 It is the most prevalent cause of motor dysfunction in children, affecting approximately 0.14–0.21% of live births ( |
front 82 Which socioeconomic group shows higher prevalence of CP? | back 82 Children from lower socioeconomic backgrounds. |
front 83 What are the 5 prenatal causes of CP? | back 83
|
front 84 A __________ is any substance or factor that can cause birth defects or developmental problems. When a pregnant person comes into contact with one, that’s called _______________________. Common examples include:
| back 84
|
front 85 What are the 3 perinatal causes of CP? | back 85
|
front 86 What are the 3 postnatal causes of CP? | back 86
|
front 87 What causes the impairment in muscle activity in CP? | back 87 Brain lesions that affect the areas controlling movement. |
front 88 What causes cerebral palsy (CP)? | back 88 damage or abnormalities in the developing brain (brain lesions) that disrupt normal communication between the brain and muscles. |
front 89 How do brain lesions lead to symptoms of CP? | back 89 The brain lesions impair muscle control, coordination, tone, and movement, causing difficulty with posture, balance, and motor function. |
front 90 What 3 types of muscle tone abnormalities and/or movement disorders can occur in CP? | back 90
|
front 91
| back 91 spasticity |
front 92
| back 92 dystonia |
front 93
| back 93 ataxia |
front 94 What is a hallmark sign of CP in movement, another result of the brain lesions? | back 94 Inefficient, uncoordinated muscle activation patterns. |
front 95 What is the average age of referral for CP evaluation? | back 95 8 months |
front 96 When do most children begin therapy services for CP? | back 96 Around 12 months |
front 97 When is the average age of diagnosis for CP? | back 97 16 mnths |
front 98
| back 98 dyskinesia |
front 99 In cerebral palsy, dyskinesia is known as an ___________________ type of CP — meaning the damage occurs in areas of the brain outside the main motor pathways (the extrapyramidal system) that help control automatic and smooth movements. Because of this, children with dyskinetic CP have______________________ movements that change with posture, stress, or emotion. These movements often fall into two main patterns:
| back 99
|
front 100 People with dyskinetic CP might show a mix of both types — movements can switch between slow and rigid to fast and flinging — but they usually do not have muscle weakness; the problem lies in ______________________, not in the _________________________________. | back 100
|
front 101 What are the types of CP based on body areas affected? (3) | back 101
|
front 102 When do brain lesions that cause CP typically occur? | back 102 The damage usually happens before, during, or shortly after birth, while the brain is still developing. |
front 103 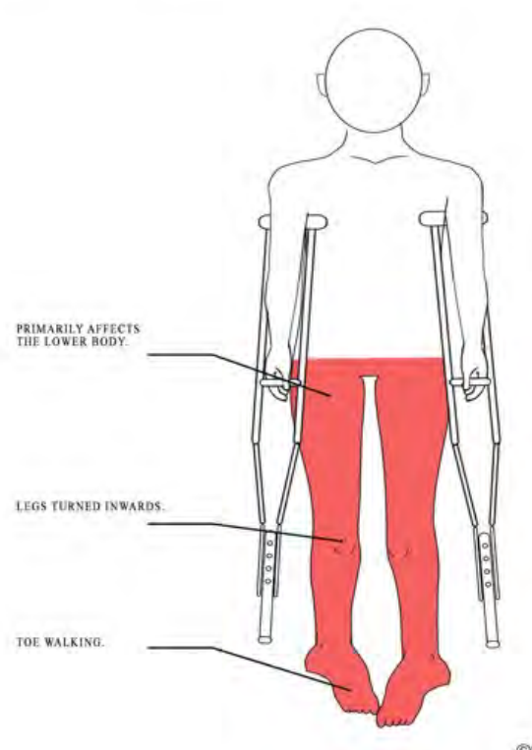
| back 103 di- (spastic) diplegia/paraplegia |
front 104 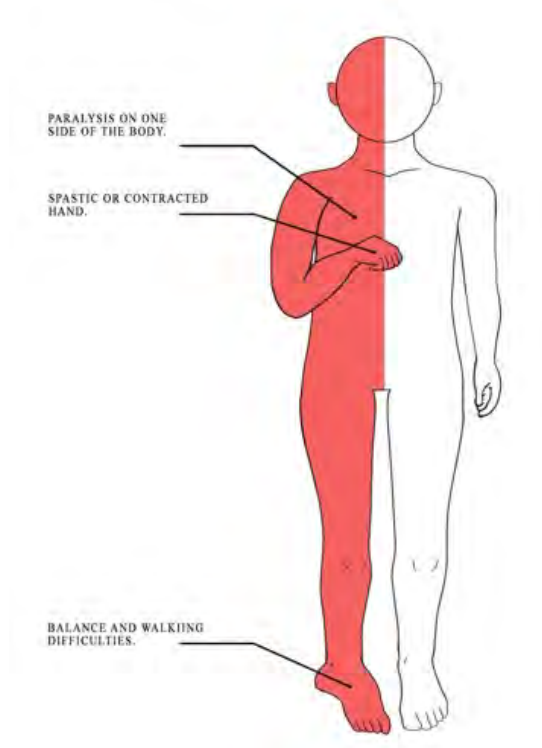
| back 104 Hemi- Spastic Hemiplegia |
front 105 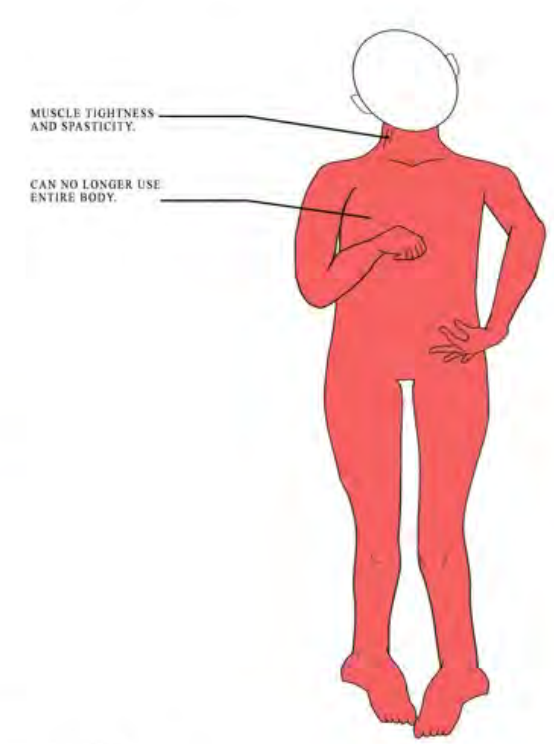
| back 105 Quadri Spastic Quadriplegia |
front 106 What are two major functional classification systems used for CP? | back 106
|
front 107 what does Gross Motor Function Classification System (GMFCS) measure? | back 107 Levels of gross motor function (e.g., sitting, walking, mobility). |
front 108 what does Manual Ability Classification System (MACS) measure? | back 108 How children with CP handle objects in daily activities (manual dexterity). |
front 109 How is CP diagnosed? | back 109 Through multiple motor assessments and neurological exams, confirmed by MRI. |
front 110 What are the 3 primary OT intervention goals for babies n toddlers w/ CP? | back 110
|
front 111 What are the five categories of Green-Light OT interventions? | back 111
|
front 112 What does “Green-Light” mean in CP interventions? | back 112 Strong research support — evidence-based and recommended OT practices. |
front 113 What is the goal of Green-Light interventions? | back 113 To improve motor function, participation, and independence through effective, proven methods. |
front 114 Activities that retrain the brain and muscles to work together effectively. | back 114 Neuromuscular Re-education |
front 115 What Green-Light neuromuscular interventions are recommended? (2) | back 115
|
front 116 method of therapy where the stronger limb is restrained to encourage use of the weaker limb, promoting neuroplasticity and active movement. | back 116 Constraint-Induced Movement Therapy (CIMT)? |
front 117 method of therapy that involves activities that require both hands to work together, improving coordination and bilateral integration. | back 117 Bimanual Training |
front 118 Practicing meaningful daily tasks to improve real-world function and independence. | back 118 task-based intervention |