Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
NAPLEX Review Test #1
front 1 Structure of amide | back 1 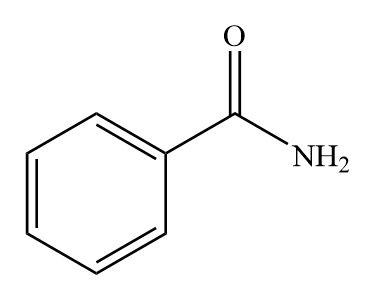 |
front 2 Structure of sulfonamide | back 2 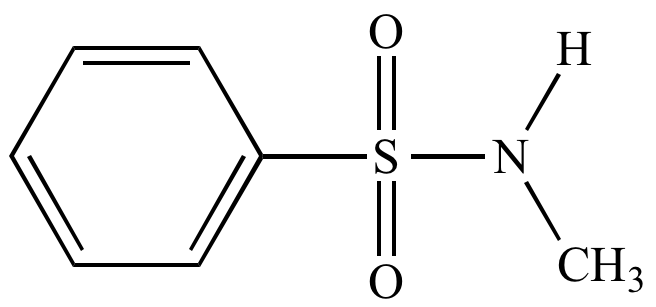 |
front 3 Which NSAID has sulfonamide functional group? | back 3 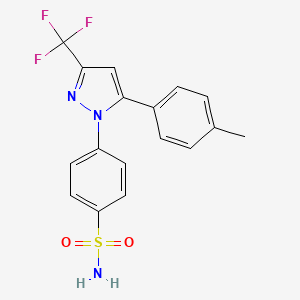 Celecoxib |
front 4 Structure of beta-lactam antibiotics | back 4 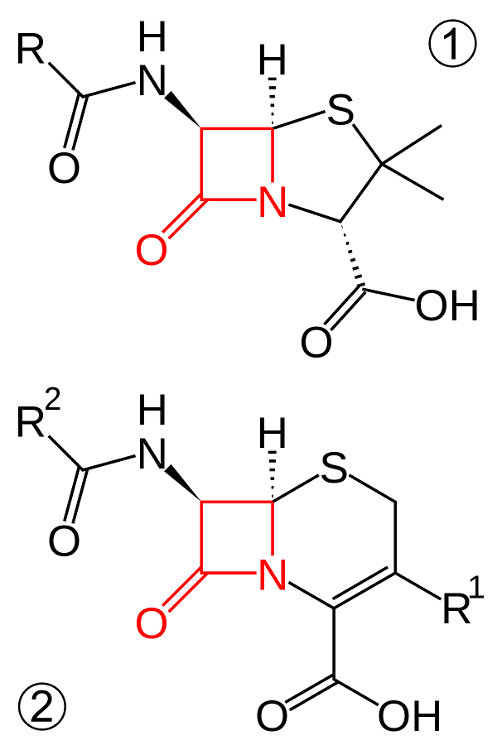 |
front 5 Define substrate/ligand | back 5 A substance that creates a signal or produces an effect by binding to a receptor, enzyme or transporter |
front 6 Define endogenous | back 6 A substance that is produced by the body (such as naturally-produced substrate) |
front 7 Define exogenous | back 7 A substance that is produced outside of the body (such as a drug or other chemical) |
front 8 Define agonist | back 8 A substance that combines with a receptor to initiate a reaction, can be endogenous or exogenous (mimicking endogenous)- activates receptors |
front 9 Define antagonist | back 9 A substance that reduces or blocks a reaction, can be endogenous or exogenous (blocks/inhibits, does not produce a reaction) |
front 10 Primary neurotransmitter involved in the somatic nervous system | back 10 acetylcholine (ACh) |
front 11 How does the parasympathetic nervous system ("rest and digest") work | back 11 By releasing ACh which binds to nicotinic receptors |
front 12 What are the physiologic responses when the parasympathetic system is activated | back 12 SLUDD (salivation, lacrimation, urination, defection, digestion) |
front 13 How does the sympathetic nervous system ("fight or flight") work | back 13 By releasing epinephrine and norepinephrine which acts on adrenergic receptors (alpha-1, beta-1 and beta-2) in the cardiovascular and respiratory system |
front 14 Activation of the SNS results in | back 14 increased BP, HR and bronchodilation and pupil dilation (decrease salivation, urination, peristalsis) |
front 15 Where are muscarinic receptors located | back 15 stomach and bladder |
front 16 Where are adrenergic receptors located | back 16 Heart (beta-1), smooth muscles including blood vessels (alpha-1), lungs (beta-2) |
front 17 Competitive inhibition | back 17 occurs when an antagonist binds to the same active site of a receptor as the endogenous substrate, preventing it from binding and causing a reaction |
front 18 Non-competitive inhibition, that antagonist binds to the receptor at a | back 18 site other than the active site (allosteric site) which changes the shape of the active site and prevents the endogenous substrate from binding |
front 19 Define pharmacodynamics | back 19 refers to the effect or change that a drug has on the body |
front 20 Define pharmacokinetics | back 20 refers to the effect or change that the body has on a drug |
front 21 CYP inhibitors | back 21 will have a decrease rate of drug metabolism and an increased serum drug level |
front 22 Common CYP inhibitors | back 22 G-PACMAN grapefruit, protease inhibitors, azole antifungals, cyclosporine, macrolides, amiodarone, non-DHP CCBS |
front 23 CYP inducers | back 23 will have an increased rate of drug metabolism and a decreased serum drug level |
front 24 Common CYP inducers | back 24 PS PORCS phenytoin, smoking, phenobarbital. oxcarbazepine, rifampin, carbamazepine, st. johns wart |
front 25 When a drug blocks/inhibits P-gp, a drug that is a P-gp substrate | back 25 will have increased absorption and the substrate drug level will increase |
front 26 Therapeutic drug monitoring (TDM) involves | back 26 obtaining a drug level or other relevant labs to monitor efficacy and safety |
front 27 What is included in a CBC | back 27 WBC, RBC PLTs (CBC w/ diff, other WBCs are analyzed) |
front 28 What is included in a BMP | back 28 electrolytes, glucose, renal function (SCr, BUN), HCO3, bicarbonate |
front 29 What is included in a CMP | back 29 BMP + albumin, ALT, AST, total bilirubin, total protein |
front 30 increased WBC | back 30 leukocytosis |
front 31 increased RBC | back 31 polycythemia |
front 32 increased PLTs | back 32 thrombocytosis |
front 33 decreased WBC | back 33 leukopenia |
front 34 decreased RBC (or low Hgb) | back 34 anemia |
front 35 decreased PLTs | back 35 thrombocytopenia |
front 36 When should you calculate corrected calcium | back 36 when albumin is low |
front 37 What drugs can increase Ca+ | back 37 vitamin D, thiazide diuretics |
front 38 What drugs can decrease Ca+ | back 38 long-term heparin, loop diuretics, bisphosphonates, cinacalcet, systemic steroids, calcitonin, topiramate |
front 39 What drugs can decrease Mg | back 39 PPIs, diuretics, amphotericin B, chronic alcohol intake, diarrhea |
front 40 What drugs can increase K+ | back 40 ACEi, ARB, aldosterone antagonist, canagliflozin, bactrim, mycophenolate, cyclosporine, tacrolimus, drospirenone-containing contraceptives |
front 41 What drugs can decrease K+ | back 41 beta-2 agonist, diuretics, insulin steroids |
front 42 What drugs can increase Na+ | back 42 tolvaptan, hypertonic saline |
front 43 What drugs can decrease Na+ | back 43 carbamazepine, SSRIs, diuretics |
front 44 When is BUN increased | back 44 renal impairment and dehydration |
front 45 Define peak level | back 45 highest concentration in the blood a drug will reach |
front 46 Define trough level | back 46 lowest concentration in the blood a drug will reach in the blood and is drawn right before the next dose |
front 47 Obtaining drug levels at steady state is | back 47 often preferred (but not always) |
front 48 USP 795 | back 48 non-sterile |
front 49 USP 797 | back 49 sterile |
front 50 USP 800 | back 50 hazardous |
front 51 What is the orange book (FDA) | back 51 list of approved drugs that can be interchanged with generics based on therapeutic equivalence |
front 52 What is the pink book (CDC) | back 52 information on epidemiology and vaccine-preventable diseases |
front 53 What is the purple book (FDA) | back 53 list of biological drug products, including biosimilars |
front 54 What is the red book | back 54 drug pricing information |
front 55 Long acting drugs provides a | back 55 smooth level of drug release over time which reduces high "peaks" and decreased side effects |
front 56 Chemical incompatibility causes | back 56 drug degradation or toxicity due to a hydrolysis, oxidation or decomposition reaction |
front 57 Drugs with leaching/adsorption/absorption issues with PVC containers | back 57 LATTIN (leach absorbs to take in nutrients) lorazepam, amiodarone, tacrolimus, taxanes, insulin, nitroglycerin |
front 58 Drugs that are compatible with saline (no dextrose) | back 58 A DIAbetic Cant Eat Pie ampicillin, daptomycin, infliximab, ampicillin/sulbactam, caspofungin, ertapenem, phenytoin |
front 59 Drugs that are compatible with dextrose (no saline) | back 59 Outrageous Bakers Avoid Salt oxaliplatin, bactrim, amphotericin B, synercid |
front 60 Central lines are required for | back 60 highly concentrated drugs, long-term antibiotics, drugs with a pH, drugs that can damage tissue |
front 61 Drugs that require filter requirements | back 61 my GAL Is PAT who has a MaP golimumab, amphotericin B, lipids 1.2 micron, isavuconazonium, phenytoin, amiodarone, taxanes, mannitol, parental nutrition |
front 62 What drugs are "do not refrigerate" | back 62 Dear Sweet Pharmacist Freezing Makes Me Edgy dexmedetomidine, sulfamethoxazole/trimethoprim, phenytoin, furosemide, metronidazole, moxifloxacin, enoxaparin |
front 63 What drugs do you have to protect from light | back 63 Protect Every Necessary Med from Daylight phytonadione (vitamin K), epoprostenol, nitroprusside, micafungin, doxycycline |