WCC QOTD &
What should the wound care specialist prioritize when a patient reports severe pain as a reaction to a newly applied enzymatic debrider?
Educate the patient that pain is an expected side effect
Apply a thicker layer of the enzymatic debrider
Reassess the patient's pain and the application techniqe of the debrider
Change to a different type of debrider STAT
Reassess the patient's pain and the application techniqe of the debrider
Reassessing both the patient's reported pain & the application technique of the enzymatic debrider is essential, as pain may indicate incorrect application or an adverse reaction. * Alter application method, or amount to alleviate pain. *
What is this:
A targeted wound care technique that uses topical prescription enzymes (like collagenase) to chemically break down and dissolve dead or necrotic tissue (eschar and slough) without harming healthy, viable tissue. It is typically applied daily under a moist dressing to continuously clean the wound bed.
Enzymatic debrider
The five most commonly known enzymatic debriders.
Collagenase, Bromelain are the most popular.
There's also:
- Fibrinolysin and Desoxyribonuclease
- Papain-Urea (e.g., Panafil)
Bromelain (e.g., NexoBrid):
A pineapple-derived concentrate of proteolytic enzymes often used for rapid, non-surgical debridement of severe burn wounds
Collagenase (e.g., Santyl):
The most widely used enzymatic debrider. It breaks down collagen in necrotic tissue to help clear slough and eschar.
_____ is a powerful proteolytic enzyme extracted from the raw latex of the papaya plant (Carica papaya). It works by breaking down large, complex proteins into smaller peptides and amino acids.
Papain
What is this?
A combination that breaks down proteins (using papain) while the urea softens the tissue to make it easier to dissolve.
Papain-Urea (e.g., Panafil)
Fibrinolysin and Desoxyribonuclease:
An older combination often derived from bovine tissue that targets fibrin clots and DNA in wound debris
____ (chemically known as carbamide, with the formula CH₄N₂O) is a nitrogen-containing organic compound. It is the primary waste product of protein metabolism in mammals and is excreted in urine. --Synthetically produced ___ has widespread industrial applications, particularly as an agricultural fertilizer and a moisturizing ingredient in skincare
Urea
How should a burn be treated if a patient has a small burn that covers less that 10% of the body's total surface area?
The burn should not be dressed
Clean the wound and apply silver sulfadiazine
Apply dry dressing
Dress with sterile sheets
Clean the wound and apply silver sulfadiazine
A small burn covering less that 10% of the total body surface sould be cleaned and silver sulfadiazine should be applied.
What sould burns covering more that 10% of the body's surface be dressed with?
Dry dressing, or Sterile sheets
How should burns on the neck, face, head, or perineum be treated?
With water based ointments such as Bacitracin
Which wound healing phase typically involves granulation tissue formation in burn wounds?
Proliferative phase
This phase characterized by the formation of granulation tissue. During this phase, fibroblasts actively produce collagen, and new blood vesses from through angionesis. This processes create a scaffold for wound contraction & eventual closure. * Keratinocytes also begin migrating across the wound bed, initiate reepithelializtion.
_____ ____ the body's primary goal is to clean & prepare the wound for healing. Neutrophils and Macrophages remove debris, bacteria, & dead tissue. Essential granulation tissue DOES NOT form during this stage
Inflammatory Phase
_____ ____, also called the remodelig phase occurs after granulation tissue has filled the wound. During this time, the wound contracts & collagen fibers are reorganized to increase tensile strength. * Scar formation & tissue remodeling take place in this phase rather than during the initial granulation.
Maturation Phase
______, sometimes considered part of the inflammatory phase, involves coagulation. Platelet aggregation & clot formation stop bleeding & provide the initial matrix for cell migration, but granulation tissue does not develop at this stage.
Hemostasis
Which patient scenario is most appropriate for the application of hydrocolloid dressings?
A surgical wound showing signs of infection
A diabetic foot ulcer w/heavy exudate
A pressure ulcer with necrotic tissue
A shallow, minimally exuding burn wound
A shallow, minimally exuding burn wound
Hydrocollod dressings are designed to maintain a moist wound environment, which promotes epithlialization & protects against bacterial contamination.
Hydrocolloid dressings are most suitable for :
Shallow wounds w/minimal exudate (e.g., mile, partial-thickness burns)
Superficial leg ulcers
Donor sites
Low to moderate pressure wounds
_____ dressings can conform to the skin, absorb light exudate, and provide a barrier to external irrtants. Making this dressing occlusive.
Hydrocolloid
Hydrocolloid dressing are not appropriate for:
* Wounds containing necrotic tissue (moisture under a hydrocolloid can worsen necrosis & promote bacterial growth; debridement is required first.
* Heavily exuding wounds: Excess fluid can overwhelm the dressing, causing leakage & loss of effectiveness.
* Infected wounds: Occlusion may trap bacteria & exacerbate infection; infected wound require drainage & antimicrobial management before using an occlusive dressing
An ___ ___is an airtight and watertight medical bandage that completely seals a wound from the outside environment. By locking moisture in and blocking bacteria, air, and fluids, it prevents the wound from drying out, accelerates healing, and reduces scarring. Hyrdocolloid dressings is this type of dressing.
occlusive dressing
A wound care specialilst is teaching a group of nurses about hydrotherapy for wound mgt. How does hydrotherapy facilitate wound healing?
By mechancally debriding the wound
By reducing the mechanical load on the wound
By decreasing pH levels in the wound bed
By increasing systemic metabolic activity
By mechancally debriding the wound
Hydrotherapy assists wound healing primarily through mechanical debridement. * The water flow loosens & removes necrotic tissue, debris & contaminants from the wound bed. ~ This mechanical action prepares the wound for the formation of new, healthy tissue & helps reduce the bacterial load, creating a cleaner environment that promotes healing.
You are a wound care spec. respnsible for developing eductional resource for staff & patients in your healthcare facility. A newly hired RN expresses interest in learning more about wound care mgt. How should you best facilitate wound care education for the hired nurse?
Direct the nurse to read medical journals on wound care independently
Provide the nurse w/access to online platforms offering wound care courses & resources
Encourage the nurse to see educational resources from community based clinics
Direct the nurse's request for education on wound care mgt. to the nursing manager for furher guidance
Provide the nurse w/access to online platforms offering wound care courses & resources.
* Most helpful providing access to an online platform that offers structured wound care courses and up-to-date resources.
The context of treating a venous leg ulcer, why is compression therapy often recommended?
To reduce edema & improve venous return
To promote oxygenation of tissues
To decrease peripheral neuropathy
To increase leukocyte infiltration
To reduce edema & improve venous return
* Compression Therapy is the cornerstone in managing venous leg ulcers because it mechanically reduces venous hypertension-a primary cause of venous ulcers.
What treatment is this is this?
By applying controlled pressure to the lower extremities, this helps veins compress & decrease the diameter of distended vessels, therby enhancing valve function.
Compression Therapy
Which of the following offloacing measures is most effective at relieving pressure & healing diabetic foot ulcers (DFUs)?
Surgical shoes
Bed rest
Wheelchair
Total-contact Cast (TCC)
Total-contact Cast (TCC)
Offloading & redistributing pressure are fundamental to prevent foot ulcers, lower extremity amputtions & promoting healing of existing diabetic foot ulcers.
Total contact casting (TCC) is a-
specialized, non-removable cast that extends from the foot to just below the knee. It molds closely to the exact contours of the foot, distributing body weight evenly across the entire sole. This offloads pressure from ulcers and bony prominences, making it the "gold standard" for treating diabetic foot ulcers
A 46-year old patient w/a history of diabetes presents with a non-healing foot ulcer. The wound has moderte exudate and signs of infection. Which of the following products choices is containdicted for this patient?
Calcium alginate dressing
Hydrocolloid dressing
Silver-containing dressing
Foam dressing
Hydrocolloid dressing
This dressings are occlusive & not containdicted for clinically infected wounds; they can limit drainage/inspection and may worsen infection risk in this context.
For a DFU w/moderate exudate & signs of infection choose the following dressings that manage exudate & allow appropriate infection mgt.
Alginate
Foam
Antimicrobial options may be used when indicated.
Which of the following indicates the need to apply anti-embolism stockings (AES)?
Absent peripheral pulses
Recent vein ligation
Arterial insufficiency
Deep vein throbosis (DVT) prophylaxis
Deep vein throbosis (DVT) prophylaxis
* AES are indicated for immobile or bedridden patient as a mechanical means of prophylaxis against deep vein thrombosis (DVT) & pulmonary embolism (PE) in a-risk patients.
Contraindications of AES - anti-embolism stockings are:
Arterial insufficiency- claudication or lower extremity pain w/elevtion
Absent peripheral pulses
Anatomic abnormalites
Aermatitis, loss of skin integrity
Massive leg edema or pulmonary edema from CHF
Lower extremity ischemia or gangrene
Recent vein ligation
* These conditions either impede proper blood flow or inbvolve surgical or pathological states in which compression therapy could exacerbate the problem.
Claudication is-
muscle pain, cramping, or fatigue—typically in the legs or buttocks—that is triggered by physical activity like walking and promptly relieved by rest
An 88 YO female pt. has been admitted to a LTC facilty w/a stage 3 pressure ulcer on her sacrum. The facility's protocol emphasizes a comprehensive, multidisciplinary approach. Which of the following actions should be the wound care spec. prioritize in accoradance to the facilty processes?
Apply a hydrocolloid dressing
Implement daily saline dressings
Refer the patient for surgical debridement of the wound
Request a nutritional assessment by a dietitian
Request a nutritional assessment by a dietitian
* A nurtitional assessment is dicated for any patient w/a stage 3 pressure ulcer.
A dietician can identify deficits in-
Protein, calories, and micronutrients; support collagen synthesis; and enhance imnune function.
______ is the most abundant protein in human blood plasma, produced by the liver. It is essential for maintaining blood volume and pressure by keeping fluid inside the blood vessels. It also acts as a carrier, transporting vital substances like hormones, vitamins, enzymes, and medications throughout the body
Albumin
A Stage __ pressure ulcer (or bedsore) is a severe, full-thickness skin injury where the damage extends completely through the outer and middle skin layers into the fatty subcutaneous tissue. It forms a deep, crater-like wound. While body fat is visible, muscle, tendon, and bone are not exposed.
3
What is the most commonly used compression product during the initial phase of treatment for lymphedema?
Intermittent pneumatic compression
Tubular sleeves
Stockings
Wraps
Wraps
Compression wraps are frequently employed as CT products, in early stages of lymphedema treatment, when there are rapid changes in limb volume d/t edema reduction.
Us of wraps for treatment of Lymphedema
Typically a healthcare professional applies the wraps, which remain in place for 3-7 days.
Types of wraps used in treatment of lymphedema:
inelastic paste wraps
multilayer elastic wraps
signle layer inelastic (short stretch) bandages
__________ is a chronic condition causing painful swelling, usually in the arms or legs. It happens when the lymphatic system—which drains excess fluid from tissues—is damaged or blocked, causing lymphatic fluid to build up beneath the skin
Lymphedema
Lymphedema is caused by the buildup of protein-rich lymph fluid in the body's soft tissues, resulting in swelling. This occurs when the lymphatic system—which is responsible for draining excess fluid and fighting infection—is _______ _______
is blocked, damaged, or poorly developed
What is a positive Buerger's sign?
A thickened fold of skin at the base fo the second toe or second finger can be gently pinched and lifted (Stemmer's sign)
Upon elevating the lower extremity for 60 sec., skin pallor is noted in patients w/ischemic skin.
Exercise induces cramping, or tiredness of the calf, thigh, or buttock (claudication)
When the lower extremity is dependent, the ischemic limb exhibits a red or ruddy color (dependent rubor)
Upon elevating the lower extremity for 60 sec., skin pallor is noted in patients w/ischemic skin.
* A positive Buerger's sign is the developement of pallor when the lower extremity is elevated for 60 sec, indicating poor arterial circulation and peripheral arterial disease (PAD).
What health conditions could a positive Buerger's sign indicate?
Poor arterial circulation & peripheral arterial disease (PAD).
_____ __ _______ is positive when the ischemic limb becomes red or ruddy in the dependent position, reflecting reactive hyperemia.
Goldflam's sign, or dependent rubor
_______ refers to exercise-induced cramping or fatigue of the calf, thigh, or buttock muscles.
Claudication
______ is identified by a thickened skin fold at the base of the second toe or finger that cannot be lifted, an early indicator of primary lymphedema
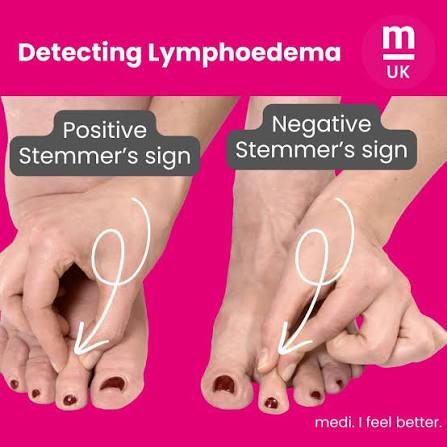
Stemmer's sign
How to test for Stemmer's sign- how it works
- The Test: An examiner gently attempts to pinch and lift a fold of skin at the base of the second toe (or the second finger).
- Negative Sign: If the skin can be easily lifted or pinched, the test is negative, usually indicating no lymphedema.
- Positive Sign: If the skin is too thickened and fibrotic to be pinched into a fold, the test is positive. This thickening occurs because of trapped, protein-rich fluid in the tissues
Is this the result of a positive, or negitive Stemmer's sign test?
If the skin is too thickened and fibrotic to be pinched into a fold, the test is ______. This thickening occurs because of trapped, protein-rich fluid in the tissues
positive
Which of the following topical agents is most appropriate for superficial second degree burns?
Silver sulfadiazine cream
Mupirocin
Aloe vera
Bacitracin
Silver sulfadiazine cream
* this is most extensively used topical agent for burn wounds in the US. Its bacterial action likely targets the bacterial cell membrane & cell wall. Application is painless, & many pt.s find the cream comfortable / soothing.
____ is not recommended in treatment for superficial second degree burns. It is reserved for infections due to methicillin-resistant Staphylococcus aureus (MRSA)
Mupirocin
_____ is appropriate for minor (first-degree) burns but is insufficient for the superficial SECOND-degree injuries.
Bacitracin
What is the primary function of the skin?
Thermoregulation
Sensing the environment
Protection
Vitamin D metabolism
Protection
* Skin's primary function is to act as a protective barrier. It defends the body against bacteria & other microbes, mechanical trauma, harmful chemicals, and excessive heat, cold, moisture, dryness, and UV radiation.
A patient w/limited insurance coverage is DC'd from the inpatient facility. When planning home wound care treatment for this patient, who should the wound care specialist prioritize collaboration with?
The Primary care physician
The social worker
The insurance company
The pharmacist
The insurance company
The insurance rep. will have specific information regarding the patient's policy-what treatments are covered & any exceptions of limitations that apply. This allows the wound specialist to plan care that aligns w/the patient's coverage, minimizing financial burden.
What is the primary purpose of educating the interprofessinal team members about wound care mgt.
To reduce overall costs related to wound care
To expedite wound healing
To standardize care procedures
To improve patient outcomes
To improve patient outcomes
Educating the interprofessional team aims to improve patient outcomes by ensuring that all team members understand and apply best practices in wound care.
Which of the following conditions is a contraindication for using Electrical Stimulation (ES) in wound care?
Peripheral vascualar disease
Osteomyelitis
Diabetic neuropathy
Pressure injuries
Osteomyelitis- Bone infection
This would be a contraindication for Osteomyelitis because the increased blood flow and cellular activity resulting from ES could exacerbate the infection. The stimulation may spread the infection to surrounding tissues, complicating pt. outcomes.
Which physical sign or symptom does not indicate malnutrition?
Obesity
Dry skin & dry mouth
Muscle weakness
Hair loss
Obesity
The Fontaine classification system for PAOD-peripheral artery occlusive disease, mild intermittent claudication corresponds to which stage?
Stage 2a
Stage 4
Stage 3
Stage 1
Stage 2a
Fontaine classification system for PAOD includes:
Stage 1: Asymptomatic
Stage 2a: Mild or intermitten claudication (occurs w/moderate-to heavy activity, relieved within 10ms of rest; typically 50% vessel occlusion)
Stage 2b: Moderate-to-severe claudication
Stage 3: Ischemic rest pain (occurs at rest, often nocturnal; indicates >90% occlusion)
Stage 4: Tissue loss (ulceration or gangrene due to total occlusion of below-knee vessels)
Fontaine classification system for PAOD includes:
Stage 1: Asymptomatic
Stage 2a: Mild or intermitten claudication (occurs w/moderate-to heavy activity, relieved within 10ms of rest; typically 50% vessel occlusion)
Stage 2b: Moderate-to-severe claudication
Stage 3: Ischemic rest pain (occurs at rest, often nocturnal; indicates >90% occlusion)
Stage 4: Tissue loss (ulceration or gangrene due to total occlusion of below-knee vessels)
Fontaine classification system for PAOD stage:
Tissue loss (ulceration or gangrene due to total occlusion of below knee vessels)
Stage 4
Fontaine classification system for PAOD stage:
Ischemic rest pain (occurs at rest, often nocturnal; indicates >90% occlusion)
Stage 3
Fontaine classification system for PAOD stage:
Moderate-to-severe claudication
Stage 2b
Fontaine classification system for PAOD stage:
Mild or intermittent claudication with moderate to heavy activity, that relieves after 10mins of rest. Typically means 50% vessel occlusion
Stage 2a
Fontaine classification system for PAOD stage:
Asymptomatic
Stage 1
Which of the following situations would indicate a need to revise the current wound care plab for a patient with a venous leg ulcer?
The wound has decreased in size by only 25% after four weeks of treatment
The skin around the wound is intact and without irritation
The exudate is foul-smelling & heavy after two weeks of treatment
The patient reports decreased pain at the wound site
The exudate is foul-smelling & heavy after two weeks of treatment
*This suggests infection or inadequate exudate management.
A 78 YO female patient presents with a non-healing venous ulcer on her right ankle. The patient has a history of varicose veins and leg edema. How would an ABI ankle-brachial index measurement of 1.2 be interpreted in this context?
Normal arterial circulation
Moderate arterial insufficiency
Arterial Calcification
Mild arterial insufficiency
Normal arterial circulation
An ABI of 0.9 to 1.3 indicates normal arterial circulation. 1.2 falls squarely within the normal range, confirming adequate arterial blood flow.
An ABI below 0.9 suggests-
arterial insufficiency (mild: 0.7-0.9)
An ABI of 0.4 to 0.7 means
Moderate arterial insufficiency
An ABI of < 0.4 (less than 0.4) means
Severe arterial insufficiency
An ABI of 1.3 often indicates
arterial calcification with non-compressable vessels.
* Do not use compression for treatment *