Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Pharmacology Exam One
front 1 Pharmaceutic phase | back 1 DISSOLUTION is the fist phase of drug action |
front 2 In the pharmaceutic phase the drug becomes a solution so that it can: | back 2 Cross the biological membrane |
front 3 Which form of drug is the most rapidly absorbed from the GI Tract? | back 3 Liquid Suspension Drugs need to be in a solution so that they are absorbed |
front 4 pharmacokinetics | back 4 is the process of drug movement to achieve drug action. Absorption--> distribution --> metabolism-->and excretion |
front 5 Protein- based drugs are destroyed by the | back 5 small intestine by digestive enzymes such as insulin and growth hormones |
front 6 According to your text a drug that is NOT highly protein bound would be: | back 6 Freely distributed to the extravascular tissue |
front 7 The route for drug absorption that has the greatest bioavailability is: | back 7 Intravenous |
front 8 Passive absorption | back 8 occurs mostly by diffusion (movement from higher concentration to lower). With the process of diffusion, the drug does not require energy to move across the membrane. |
front 9 Active absorption | back 9 requires a carrier such as an enzyme or protein to move the drug against a concentration gradient. Energy is required. |
front 10 Pinocytosis | back 10 is a process by which cells carry a drug across their membrane by engulfing the dug particles. |
front 11 drugs that are lipid soluble pass | back 11 pass rapidly through GI membranes. The GI membrane is composed mostly of lipid and protein, so drugs pass easily. |
front 12 Water-soluble drugs need a | back 12 Carrier. either enzyme or protein to pass through the membrane |
front 13 Large particle pass through a cell membrane if the are | back 13 Non ionized (have no positive or negative charge). *weak acid drugs such as aspirin are less ionized in the stomach, and they pass through the stomach lining easily and rapidly. |
front 14 Drugs that are lipid soluble and nonionized are absorbed ____ than water-soluble and ionized drugs | back 14 FASTER |
front 15 The process in which the drug passes to the liver first is called | back 15 FIRST- PASS EFFECT, or hepatic first pass |
front 16 Bioavailability | back 16 is the subcategory of absorption. It is the percentage of administered drug dose that reaches the systemic circulation. |
front 17 The serum half-life of a drug is the time required: | back 17 After absorption for half of the drug to be eliminated |
front 18 T.C. has liver and Kidney disease. He is given a medication with a serum half-life of 30 hours. You expect the DURATION OF ACTION of this medication to: | back 18 Increase |
front 19 Free drugs | back 19 (drugs not bound to protein) are active and can cause a pharmacologic response. The portion of the drug that is bound is inactive because it is not available to receptors. As free drug in the circulation decreases, more bound drug is released from the protein to maintain the balance of free drug. |
front 20 When two highly protien bound drugs are given concurently | back 20 they compete for protein-binding sites, thus causing more free drug to be released into the circulation. |
front 21 Primarily ___ is what protein binding drugs bind to | back 21 albumin |
front 22 For elimination through the Kidneys to be possible, a drug must: | back 22 Be Water-Soluble |
front 23 Creatinine is normally excreted in urine as metabolic waste. However in a renal disorder you would expect the blood creatinine level to be: | back 23 Increase |
front 24 Metabolism | back 24 body inactivates or bio transforms drugs. Primary site is the liver. Most drugs are inactivated by liver enzymes and are then converted or transformed by hepatic enzymes to inactive metabolites or water-soluble substances for excretion. |
front 25 A large % of drugs are lipid soluble; thus the liver metabolizes the lipid-soluble drugs substances to______ | back 25 water-soluble substance for renal excretion |
front 26 factors affecting ABSORPTION | back 26
|
front 27 Cytochrome P450 is a | back 27 family of isozymes responsible for the biotransformation of several drugs.
Drug metabolism via the cytochrome P450 system has emerged as an important determinant in the occurrence of several drug interactions that can result in drug toxicities, reduced pharmacological effect, and adverse drug reactions. Recognizing whether the drugs involved act as enzyme substrates, inducers, or inhibitors can prevent clinically significant interactions from occurring. |
front 28 Prodrugs | back 28 converted from inactive form to active |
front 29 Most drugs are excreted by the kidneys..other routes include? | back 29 Kidney = #1 bile, feces, lungs, saliva, sweat, and breast milk |
front 30 Acidic urine promotes the elimination of _____ & alkaline urine promotes elimination of ______ | back 30 weak based drugs weak acid based drugs |
front 31 Pharmacodynamics | back 31 is the study of the way drugs affect the body. Drug response can cause a primary or secondary physiologic effect or both. The primary is desirable, the secondary effect may be desirable or undesirable. |
front 32 Dose response = | back 32 the relationship between the minimal vs the maximal amount of drug needed to produce the desired affect. |
front 33 Onset of action | back 33 is the time it takes to reach the minimum effective concentration after a drug is administered. |
front 34 Peak action= | back 34 occurs when the drug reaches its highest blood or plasma concentration |
front 35 Duration of action= | back 35 the length of time the drug has a pharmacologic effect |
front 36 drugs act through receptors by ? | back 36 binding to the receptor to produce (INITIATE) a response or to block (PREVENT) a response The better a drug fits at the receptor site, the more biologically active the drug is. |
front 37 agonist drugs | back 37 drugs that produce a response |
front 38 antagonist drugs | back 38 drugs that block a response |
front 39 Cholinergic receptors pg.8 | back 39 are located in the bladder, heart, blood vessels, stomach, bronchi, and eyes. A drug that stimulates or blocks the cholinergic receptors affects the anatomic sites of location. |
front 40 Categories of Drug Action | back 40 1. stimulation or depression 2. replacement 3. inhibition or killing of organisms 4. irritation |
front 41 The biological activity of a drug is determined by the: | back 41 Fit of the drug at the receptor site |
front 42 A mechanism of drug action that does not involve a receptor or enzyme such as a cancer drug is: | back 42 Nonspecifc |
front 43 Drugs that attach but do not elicit a response are called: | back 43 Antagonists |
front 44 Knowledge of drug potency does NOT enable us to predict whether a potent drug is more or less toxic. The valid indicator that measures the margin safety of the drug is its: | back 44 Therapeutic Index |
front 45 Drugs with narrow therapeutic ranges such as digoxin (0.5-2 ug/ml), require plasma/serum drug level monitoring _____ to avoid drug toxicity. | back 45 At periodic Intervals |
front 46 After drug administration, the highest plasma/serum concentration of the drug at a specific time is called: | back 46 Peak Level |
front 47 Prior to administration of a medication, the nurse should check a drug reference book to obtain the following pertinent data for: | back 47 1. Protein-binding effect 2. Half-Life 3. Therapeutic Range |
front 48 A time response curve evaluates three parameters of drug action, which does NOT include: | back 48 Therapeutic Range |
front 49 When immediate drug response is desired, a large initial dose is given to rapidly achieve an MEC in the plasma. | back 49 Loading Dose |
front 50 Peak drug levels | back 50 indicate the rate of absorption of the drug highest concentration of a drug |
front 51 trough drug levels | back 51 indicate the rate of elimination of the drug lowest concentration of a drug |
front 52 drugs with a high therapeutic index have a | back 52 wide margin of safety and less danger of producing toxic effects |
front 53 Side effects and adverse reaction | back 53 are physiologic effects not related to desired drug affects. Adverse reaction are more severe than side effects. |
front 54 Tolerance | back 54 refers to a decreased responsiveness over the course of therapy. |
front 55 Absorption, Distribution, Metabolism(biotransformation), Excretion of drugs by the body | back 55 Pharmacokinetics |
front 56 Biochemical and Physical effects of drugs and mechanism of drug actions | back 56 Pharmacodynamics |
front 57 Name given by United States Adopted Name Council | back 57 Generic (NONPropietary) Name |
front 58 Celeste = | back 58 Hoe |
front 59 Lety= | back 59  (no comment) |
front 60 Pregnancy Category A | back 60 No risk to fetus |
front 61 Pregnancy Category B | back 61 no risk to animal fetus but information in humans is unavailable |
front 62 Pregnancy Category C | back 62 Adverse effects in animal fetus, in humans is unavailable |
front 63 Pregnancy Category D | back 63 Possible fetal risk in humans reported, however potential benefit may in selected cases may warrant use of drug |
front 64 Pregnancy Category X | back 64 Fetal Abnormalities reported and positive evidence of fetal risk in humans is available from animal/human studies. Never should be taken by pregnant women. |
front 65 Therapeutic action of drug Risk Vs. Benefit | back 65 Benefits |
front 66 Side Effects/ Adverse reactions or contraindication Risk Vs. Benefit | back 66 Risk |
front 67 prevention of disease through vaccine | back 67 Prophylactic (Drug Therapy) |
front 68 Drug bound to protein, cause inactive drug action/response | back 68 Protein bound drug |
front 69 Not bound to protein causing pharmacologic response that is active. | back 69 Free Drug |
front 70 As it decreases, more bound drug is released from protein | back 70 Free drug |
front 71 Time it takes for one half concentration to be eliminated | back 71 Half-Life |
front 72 Drug reaches highest blood/plasma concentration | back 72 Peak Action |
front 73 length of time drug has pharmacologic effect | back 73 Duration of Action |
front 74 Medication given on time. Given at Correct time. Lab aware of tests. Set up blood draw | back 74 Responsibilities of Nurse obtaining Peak And Trough |
front 75 Indicate Time of highest plasma concentration & Rate of absorption. | back 75 Peak |
front 76 Time of lowest plasma concentration & Rate of Elimination | back 76 Trough |
front 77 IV, IO ET, INHALATION SL, RECTAL, BUCCAL IM SQ PO | back 77 ROUTES of Drug Admin. in ORDER OF RAPID ABSORPTION |
front 78 "RIGHT" Medication Administration check list | back 78 right drug right dose right time right route right patient |
front 79 What Nurse listens to from pt as they list symptoms | back 79 Subjective Data |
front 80 What Nurse Observes | back 80 Objective Data |
front 81 Dissolution of the drug | back 81 Pharmaceutic |
front 82 Effect of drug action because of hereditary influence | back 82 Pharmacogenetic |
front 83 4 processes of drug movement to achieve drug action | back 83 Pharmacokinetic |
front 84 Effect of drug action on cells | back 84 Pharmacodynamic |
front 85 Drug that block a response | back 85 Antagonist |
front 86 Drug that produces a response | back 86 Agonist |
front 87 Drug absorbed by diffusion | back 87 Passive Absorption |
front 88 Which type of drug passes rapidly through the GI Membrane? | back 88 Lipid-Soluble and nonionized |
front 89 What Affects a drug absorption? | back 89 Hypotension, Pain, Stress |
front 90 Two drugs given together cancels the effect of each other | back 90 Antagonistic Effect |
front 91 Adrenergic agonist affect the.. | back 91 sympathetic nervous system |
front 92 Sympathomimetics affect the ... | back 92 sympathetic nervous system |
front 93 Adrenergic receptors are typically found where in the body? | back 93 effector cells of muscles, such as the heart, bronchiole walls, gastrointestinal tract, urinary bladder, and ciliary muscle or the eye. |
front 94 What does and Alpha ONE receptor do? | back 94 increases force of heart contraction; vasoconstriction increases blood pressure; mydriasis (dilation of pupils) occurs; decreases secretion in salivary glands; increases urinary bladder relaxation and urinary sphincter contraction. |
front 95 What does an Alpha TWO receptor do? | back 95 Inhibits release of norepi; dilates blood vessels; produces hypo-tension; decreases gastrointestinal motility and tone. |
front 96 Beta ONE receptors do? | back 96 Increases heart rate and force of contraction; increases renin secretion, which increases blood pressure. |
front 97 Beta TWO receptors do? | back 97 dilates bronchiloes; promotes gastrointestinal and uterine relaxation; promotes increase in blood sugar through glycogenolysis in liver; increases blood flow in skeletal muscles |
front 98 alpha-adrenergic receptors are located in | back 98 blood vessels, eyes, bladder, and prostate |
front 99 alpha 2 receptors are located in the | back 99 the postganglionic sympathetic nerve endings. |
front 100 Beata 1 receptors are located in the | back 100 kidney but primarily the heart |
front 101 beta 2 receptors are found mostly in the | back 101 smooth muscles of the lung and gastrointestinal tract, the liver, and the uterine muscle. |
front 102 Schedule I | back 102 heroin, hallucinogens (LSD, marijuana[except when prescirbed with cancer treatment], mescalin, peyote, psilocybin.) *high potential for drug abuse not accepted medical use. |
front 103 Schedule II | back 103 *high potential for drug abuse. Accepted medical use. Can lead to strong physical and psychological dependency ex: demerol, morphine, hydrocodone, methadone, oxycodone |
front 104 What schedule is cocaine? | back 104 schedule II |
front 105 schedule III | back 105 *Medically accepted drugs.Potential abuse is less that that of schedule I and II. May cause dependence. |
front 106 Schedule IV | back 106 *Medically accepted drugs. May cause dependence. |
front 107 Schedule V | back 107 *Medically accepted drugs. Very limited potential for dependence. (codeine in cough preparations) |
front 108 What is the nurses role in administering controlled substances? | back 108
|
front 109 misfeasance | back 109 negligence; giving the wrong drug or drug dose that results in the patient's death. |
front 110 nonfeasance | back 110 omission; omitting a drug dose that results in the patient's death |
front 111 Malfeasance | back 111 giving the correct drug but the wrong route that results in the patient's death |
front 112 How do you know a generic drug is just as effective? | back 112 *it is given an "A" rating generic drugs have the same active ingredients as brand name drugs but are usually less expensive because manufacturers do not have to do extensive testing; these drugs were clinically tested for safety and efficacy by the pharmaceutic company that first formlated the drug. |
front 113 Pharmacogenomics | back 113 refers to the general study of all the different genes that determine drug behavior. |
front 114 an enzyme system either induces or inhibits the action of substrates. Induction or inhibition of a substrate accounts for the variations in drug metabolism in individuals and groups. | back 114 Cytochrome P-450 enzyme system |
front 115 Poor metabolizers of antidepressants, antipsychotics, cardiovascular agents, and isoniazid, which can lead to toxicity | back 115 people of european descent |
front 116 Many have diminished therapeutic, effects from beta blockers, ACE inhibitors, and warfarin sodium | back 116 People of African descent |
front 117 drug interaction | back 117 as an altered or modified action or effect of a drug as a result of interaction with one or multiple drugs. |
front 118 Pharmacokinetic interactions | back 118 are changes that occur in the absorption, distribution, metabolism or bio-transformation, and excretion of one or more drugs |
front 119 One drug can block, decrease, or inccrease the absorption of another drug. It can do this by? | back 119
|
front 120 Category I - over the counter drugs | back 120 drugs judged to be safe and effective |
front 121 Category II- OTC | back 121 drugs judged to be unsafe or ineffective; these drugs should not be included in nonprescription products |
front 122 Category III- OTC | back 122 drugs for which there is insufficient data to judge safety or efficacy |
front 123 drug misuse | back 123 indiscriminate or recration use of a chemical substance or its use for purposes other than those for which is intended. |
front 124 drug abuse | back 124 drug use inconsistent with medical or social norms |
front 125 How do you define addiction | back 125 a compulsive, uncontrollable craving for and dependence on a substance to such a degree that cessation causes severe reactions |
front 126 what is tolerance | back 126 the need for a larger dose of a drug to obtain the original euphoria. Decreased effect of a substance that results from repeated exposure. It is possible to develop cross-tolerance to other substances in the same category |
front 127 what is craving for a drug | back 127 subjective need for a substance, usually experienced after decreased use or abstinence. Cue-induced craving is stimulated in the presence of situations previously associated with drug taking. |
front 128 Withdrawal syndrome | back 128 Constellation of physiologic and psychologic responses that occur when there is abrupt cessation or reduced intake of a substance on which an individual is dependent or when the effect is counteracted by a specific antagonist |
front 129 Metabolism of Alcohol? | back 129
|
front 130 Alcohol Pharmacology | back 130
|
front 131 Alcohol toxicity ..what happens? | back 131
*dangerous in combo with other depressants |
front 132 Physiological effects of Cocaine | back 132
|
front 133 Cocaine toxicity looks like? | back 133
|
front 134 Physiological effects of Meth | back 134
|
front 135 Meth toxicity ? | back 135
|
front 136 Aloe Vera | back 136 externally used for treatment of minor burns, insect bites, and sunburns. (fresh is better) Some success with the treatment of dandruff, oily skin, and psoriasis. Taken internally, aloe vera is a powerful laxative. Menstrual flow is increased with small doses. |
front 137 Garlic: what is it good for? | back 137 detoxifies body and increases immune function; decreases platelet aggregation; increases HDL and decreases cholesterol and triglycerides. Caution: with prescription anticoagulants because of increased fibrinolysis and decreased platelet aggregation SE: heartburn, flatulence, gastric irritation, decreased RBC, dizziness, diaphoresis |
front 138 Ginkgo biloba | back 138 Antioxidant; peripheral vasodilation and increased blood flow to CNS, reduces platelet aggregation. Uses: allergic rhinitis, Alzheimer's, anxiety/stress, dementia, vertigo, poor circulation, altitude sickness. Erectile dysfunction. |
front 139 Role of the nurse when it comes to educating about herbal therapies | back 139
|
front 140 Pharmacodynamics in the pediatric pt | back 140
|
front 141 Pharmacokinetics in the pediatric pt | back 141
|
front 142 Absorption and the pediatric pt | back 142
|
front 143 Distribution in the pediatric pt | back 143
|
front 144 Metabolism in the pediatric pt | back 144 higher metabolic rates |
front 145 Excretion in the pediatric pt | back 145 immature kidneys |
front 146 Pharmacokinetics in the geriatric pt (absorption, distribution, metabolism, excretion) | back 146
|
front 147 Pharmacodynamics in the geriatric pt | back 147
|
front 148 The geriatric pt and Cardiac glycosides | back 148 careful monitoring |
front 149 the geriatric pt and Anticoagulants | back 149 warfarin highly protein bound---> albumin levels are low= high free drug *close monitoring |
front 150 The geriatric pt and GI drugs | back 150
TAGAMET= CAUTION: not good for the older adult..it interacts with every other drug |
front 151 Are home health aide allowed to give medication? | back 151 legally home health aids may only assist with medications the patient customarily self-administers. |
front 152 What happened to the babies that were born after mom took THALIDOMIDE for morning sickness? | back 152 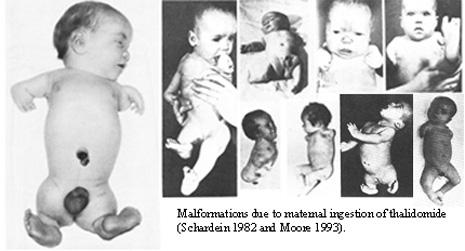 |
front 153 Herbal use and pregnancy | back 153  Moms need to be managed on how they can affect the body |
front 154 Iron and pregnancy | back 154 need more RBC= higher blood volume -dark leafy greens, fortified meats. -begin in the 2nd trimester -take on empty stomach -main issues include constipation, dark stools, nausea. -Relief: fiber and water |
front 155 Folic acid and pregnancy (vitamin B9 & folate) | back 155
|
front 156 What is Tocolytic therapy? | back 156
Moral of the story: if you limit the available calcium= interrupt uterine contractions= additional time for fetal maturation & delay delivery |