Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
OB midterm
front 1 duration of pregnancy | back 1 Prenatal period: a time of physical and psychologic preparation for birth and parenthood Duration of pregnancy: gestation
|
front 2 Healthy People 2020 maternal goals | back 2
|
front 3 Top three risk factors ob | back 3
|
front 4 Paternal adaptation to pregnancy three phases | back 4
|
front 5 Maternal Adaptation to pregnancy three phases | back 5 uMaternal adaptation
|
front 6 3 parts to first prenatal visit | back 6
|
front 7 Follow up visits | back 7
|
front 8 nnormal prenatal care timeline | back 8 Normal prenatal care = q month until 28 weeks, then q 2 months until 36 weeks, then every week until delivery. |
front 9 iMMUNIZATIONS | back 9 Immunizations: MMR, TdAP (3rd trimester), flu, pneumovax, varicella |
front 10 1.With regard to follow-up visits and the physical examination for women receiving prenatal care, nurses should be aware that: a.The interview portions become more intensive as the visits become more frequent over the course of the pregnancy. b.Monthly visits are scheduled for the first trimester, every 2 weeks for the second trimester, and weekly for the third trimester. c.During the abdominal examination, the nurse should be alert for supine hypotension. d.For pregnant women, a systolic blood pressure (BP) of 130 mm Hg and a diastolic BP of 80 mm Hg is sufficient to be considered hypertensive | back 10 C |
front 11 What is supervena cavas syndrome | back 11 HOTN and less O2 to baby |
front 12 How to care for a variety of women in pregnancy | back 12
|
front 13 sex and pregooss | back 13
|
front 14 cAN I TRAVEL BY AIRPLANE | back 14 Travel beyond 34 – 35 weeks not condoned by airlines 2/2 risk of contractions from cabin pressure changes |
front 15 What else to teach mom at visits | back 15
|
front 16 When would mom get ultrasound to estimate date of delivery | back 16 best at 1-13 weeks |
front 17 1. Prenatal period definition: 2. Gestation definition: 3. Length of pregnancy/how many weeks in 1st 2nd and 3rd term?: | back 17 1. A time of physical and psychologic preparation for birth and parenthood 2. Duration of pregnancy: 3. Spans 9 calendar months, 10 lunar months 40 weeks or 280 days Trimesters First: weeks 1-13 Second: weeks 14-26 Third: weeks 27-40 |
front 18 Signs and Symptoms of Pregnancy: 1. Presumptive 2. Probable 3. Positive | back 18 1. Suggested by the patient - GI: Amenhorrea, nausea, vomiting, morning sickness - Breast tenderness, need to pee, fatigue - Quickening- feel the baby move at 16-20 weeks. 2. Probable: by examiner - Pregnancy Test - Uterine enlargement - Braxton Hicks contractions - Placental souffle - Ballottement 3. Positive: Attributed to the FETUS - Ultrasound - Movement felt by someone else- third trimester - Fetal heart beat distinct from mom - Visualization of fetus |
front 19 Estimated Date of Birth/Delivery: how to calculate? And who came up w/ this calculation? Also, what is the gold standard for finding date of birth? | back 19 1. Take last menstural period 2. Substract 3 calender months 3. Add 7 days 4 This rule was founded by: Naegeles 5. Gold standard is ultrasound |
front 20 Prenatal period: 1. Initial interview items | back 20 1. Initial visit
2. Physical assessment:
|
front 21 Prenatal: 2. Follow up visits | back 21 Follow-up visits
|
front 22 Terms: 1. Gravida | back 22 Gravida: women who is pregnant |
front 23 2. Gravity | back 23 Gravity: the pregnancy |
front 24 3. Mulitgravida | back 24 Multigravida- women with more than 2 pregnancies |
front 25 Multipara | back 25 Multipara: women who has completed 2 or more pregnancies |
front 26 Nulligravida | back 26 women who has never been pregnant |
front 27 Parity | back 27 Parity : number of pregnancies in which fetus or fetuses have reached VIABILITY (20 wks), NOT the number of fetuses born |
front 28 Nullipara | back 28 Nullipara : woman who has not completed pregnancy with a fetus or fetuses who have reached the stage of fetal viability |
front 29 Primipara | back 29 Primipara : A woman who has completed one pregnancy with a fetus or fetuses who have reached 20 weeks of gestation |
front 30 Multipara: | back 30 Multipara : A woman who has completed two or more pregnancies to 20 weeks of gestation or more |
front 31 Preterm: | back 31 Preterm : a pregnancy that has reached 20 weeks of gestation but ends before completion of 37 weeks of gestation |
front 32 Late preterm: | back 32 Late preterm : a pregnancy that has reached between 34 weeks 0 days and 36 weeks 6 days of gestation |
front 33 Early Term: | back 33 Early term : a pregnancy that has reached between 37 weeks 0 days and 38 weeks 6 days of gestation |
front 34 Full Term: | back 34 Full term : a pregnancy that has reached between 39 weeks 0 days and 40 weeks 6 days of gestation |
front 35 Late term : | back 35 Late term : a pregnancy that has reached between 41 weeks 0 days and 41 weeks 6 days of gestation |
front 36 Post term: | back 36 Post term : a pregnancy that has reached between 42 weeks 0 days and beyond of gestation |
front 37 2 digit system used to identify the number of pregnancies | back 37 2 digit system: G__ P__ G – Gravida P - Parity |
front 38 5 digit system | back 38 5 digit system: G__ T__ P__ A__ L__ G – Gravida T – Term birth P – Preterm birth A – Abortions and Miscarriages L – Living children |
front 39  | back 39 G- 3 T- 0 P-1 A- 1 L- 1 |
front 40  | back 40 G- 4 T- 1 P- 0 A- 2 L-1 |
front 41  | back 41 no data |
front 42 Uterus Changes in Pregnancy: - What is hegar sign - What are false contractions called - What is bouncing of the baby in utero called - what is quickening | back 42
|
front 43 Cervical changes in pregnanyc: what is chadwhick versus goodell sign | back 43
|
front 44 Vagina and vulva What is operculum | back 44
|
front 45 Breast changes | back 45
|
front 46 Cardiovascular changes BP, blood flow, hr, coaguability? | back 46 Slight hypertrophy:bigger heart: moves and rotates due to the fetus
pushing. Pulse: Apical impulse shifts. 20 weeks, audible splitting of s12 and 3. Maternal hr begins increasing at wk 5 but increases by 10-15 by 32 week. |
front 47 Respiratory changes | back 47
|
front 48 Renal - urine, ureters | back 48
|
front 49
| back 49 malasma: darkened pigmentation- especially in dark skinned people Linea nigra- from symphimas pubis to top of fundus. Striae gravadrum. PUPPP: pruritic, uriticaric, plaques and papules of pregnancy. – red marks on ab. |
front 50 muskuloskeletal | back 50 -Musckuloskletal: relaxin hormones +progesterone relaxes bones, ribs are relaxed so you can fit the baby. Pelvis- relactin makes it loser. Hip pain joint pain, waddleing. Posture changes- lower back change. Walk straight. Belly band. Carpel Tunnel |
front 51 GI changes GI, mouth, appetite, liver | back 51 Gastrointestinal system |
front 52 Sonograms in pregnacy | back 52
|
front 53 induction in wmoen with previous scars | back 53
|
front 54
| back 54
|
front 55
| back 55 UTI |
front 56 Change in hr in pregnancy | back 56
|
front 57 Anemia in pregnancy due to | back 57
|
front 58 Common antepartum complications | back 58
|
front 59 Diabetes Mellitis | back 59
|
front 60 Diabetes Mellitis classifications and types | back 60
|
front 61 Glucose changes in pregnnacy | back 61
|
front 62 Gestational Diabetes | back 62 Complicates 3% to 9% of all pregnancies Fetal risks
|
front 63 Macrosemia vs. LGA | back 63
|
front 64 macrosmia causes risk for... | back 64 shoulder dystopia |
front 65 Screening for gestational diabetes: 1. What makes them at high risk for GDM: 2. Screening | back 65 -screening: 1. High risk: obesity, corticosteroids, hx of gdm in previous pregnancies, races AA, NA Asian 2. Screen: -1 hour glucose testing test, glucola, sweet orange juice- draw one bloodwork or finger gluocse to see level- if over 130= positive -Do between 24 and 28- if positive do a longer test, a fasting, 1hr, 2hr and 3hr. -if before 20 weeks evaluated probably diabetes not GDM |
front 66 GDM care management: Antepartium | back 66
|
front 67 GDM Care: Intrapartum | back 67
|
front 68 GDM care: postpartum | back 68
|
front 69 Key points for diabetes in pregnancy | back 69
|
front 70 Hyperemesis Gravidarum | back 70
|
front 71 Assessment for HG | back 71
|
front 72 Initial Care for HG: can be done outpatient! | back 72
|
front 73 Key points for managing HG | back 73
|
front 74 Women with hyperemesis gravidarum: a.Are a majority, because 80% of all pregnant women suffer from it at some time b.Have vomiting severe and persistent enough to cause weight loss, dehydration, and electrolyte imbalance c.Need IV fluid and nutrition for most of their pregnancy d.Often inspire similar, milder symptoms in their male partners and mothers | back 74 B |
front 75 Hypertensive Disorders: background and significance | back 75
|
front 76 Morbidity and Mortality due to HTN Disorders | back 76
|
front 77 Types/Classification of HTN disorders | back 77 1. Gestational HTN 2. Preeclampsia 3. Eclampsia 4. Chronic HTN 5. Chronic HTN w/ superimposed preeclampsia |
front 78 Gestational HTN: | back 78
|
front 79 Systolic over 140 or diastolic over 90 is ______________. Systolic over 160 or diastolic over 110 is __________________. | back 79 1. hypertensive 2. very concerned |
front 80 Preeclampsia definition | back 80
|
front 81 common feature of gest. htn and preecclampsia | back 81 What is a common feature of gestational HTN and preeclampsia? |
front 82 Chronic HTN and Chronic HTN w/ superimposed preeclampsia | back 82
|
front 83 Preeclampsia etiology | back 83
|
front 84 Preeclampsia pathophysiology | back 84
|
front 85 Preeclampsia pathophysiology 2: what does this mean happens? | back 85
|
front 86 labs for preeclampsia | back 86
|
front 87 What does Right upper gastric pain test in preeclampsia | back 87 -Upper gastric is liver backing up! |
front 88 What does Headache, blurred vision, swelling mean in preeclampsia | back 88 retinal spasm and cortical brain spasm |
front 89 edema where is most important | back 89 hands nad face |
front 90 Chart on what happens in preeclampsia and s&sypmtoms Corticobrain spasm causes what three things? | back 90 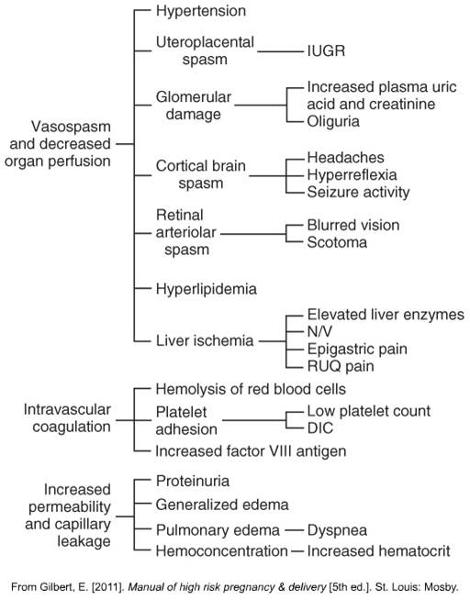 |
front 91 Identifying and preventing preeclampsia | back 91
|
front 92 Assessment and Nurising Diagnoses for Preeclampsia What is HELLP syndrome in preeclampsia | back 92
|
front 93 Interventions Preeclampsia mild | back 93
|
front 94 Interventions preeclampsia SEVERE wHEN DO PREECLAMPSIA PT USUALLY HAVE THE BABY? | back 94
|
front 95 When is delivery usually called for before 39 weeks | back 95 Consistent 160/110, organ compromise, or consistent elevated labs call for delivery regardless of whether 39 weeks has been reached. |
front 96 After 1st preeclampsia pregnancy will I have another, or HTN? | back 96
|
front 97 Key points preeclampsia | back 97
|
front 98 A client at 36 weeks of gestation presents to labor and delivery complaining of a constant headache for the past 2 days. She also states that her face “seems more swollen than usual.” What should be the nurse’s first action? a.Obtain a urine sample. b.Place the client on a fetal heart monitor. c.Notify the physician of the client’s concerns. d.Take the client’s blood pressure. | back 98 D |
front 99 why do we want a babe to make it to 34 wks what do we give then if required delivery | back 99 try to keep baby in for 34 weeks to allow for lung maturation and ensure baby will be able to breathe on its own once born. Give betamethasone in case delivery before 34 weeks is required. |
front 100 Antepartal Hemorragic Disorders: why are they a big deal and what are people at risk for? | back 100
|
front 101 Fetal risks from maternal hemmorage | back 101
|
front 102 Early Pregnancy Bleeding usually results in this | back 102
|
front 103 Types of miscarriages and what they mean | back 103 -Threatened: bleed a little, still viable. Do sonogram-check fetal heart -Inevitable: mom bleeding heavier, expelling everything- provide supportive measures. -Incomplete: tissue comes out, rather than formed fetus. Blood tissue clots- expel some of it, but some still stuck inside- intervene, send for scraping and vaccuuming. -Complete- everything comes out. No more disconfort- severe cramping, getsrid of everything, uterus stops crampong. -Missed- no bleeding, but no heart beat. Abortion. 3 fold treatment: expectant – let the body do it itself. 2nd is medical intervention = misoprostil- use for inducing missed miscarriage. -Recurrent: probably need sto go to reproductive med. 3 is a lot of babys to lose. >35 needs to go to see a specialist. -Recurrent- |
front 104 Miscarriage Management | back 104
|
front 105 What is an ectopic Pregnancy incidence and etiology clinical manifestations | back 105
1.Abdominal pain 2.Delayed menses 3.Abnormal vaginal bleeding (spotting) |
front 106 More on ectopic pregnancies, what do you do | back 106 -ectopicà lifethreatening. Instead of imbedding into the uterus, it is imbedded into follopian tubes. May rupture! ED - PAIN! One sided pain not general cramping. -Ectopic severe pain on the tube side. -Sonogram to determine where it is. -Ectopicàgive meds to abort. |
front 107 Late Pregnancy bleeding: Placenta Previa | back 107
|
front 108 placenta previa incidence manifestations maternal fetal outcomes | back 108
|
front 109 placenta previa: diagnoses and care management | back 109
|
front 110 Placental Abruption, premature Risk factors? | back 110
Maternal hypertension is a primary risk factor |
front 111 Placental Abruptions: manifestations diagnoses | back 111
|
front 112 key points hemmoragic disorders | back 112
|
front 113 What is the passenger during labor? - what is important in the passenger What is the presentation? | back 113 Passenger: fetus Size of the fetal head Bones in the fetal skull Fontanels Molding Presentation of the fetus: the part of the fetus that enters the pelvic inlet first and leads through the birth canal during labor Cephalic Breech Shoulder |
front 114 More to do with the passenger: What is the hardest part of passenger to come through? Why can this part come through okay? When should they lie in a cephalic position by? and why? What do they do if the baby is not cephalic? What does cephalic mean? What does breech mean? What does scapula mean Transverse?? | back 114 Passenger: Hardest part is head, which needs to maneuver and come out first. Majority come out head first. Should be in cephalic position by 37 weeks (term) baby is big, and cant maneuver. Will do an external rotation if not in cephalic at 37 weeks. Decreases csection rates. Cephalic- head down Breech- sacrum down Scapula- shoulder Transverese Fetal head: not completely fused, even though they have bones- don’t fuse till 18 montsh of age. helps with birth because still moveable. Biparietal diameter is the largest piece to get through thte pelvis. |
front 115 Fetal position means: What is cephalic Vertex? ROA? LOA? Rot/Lot Rop//Lot | back 115 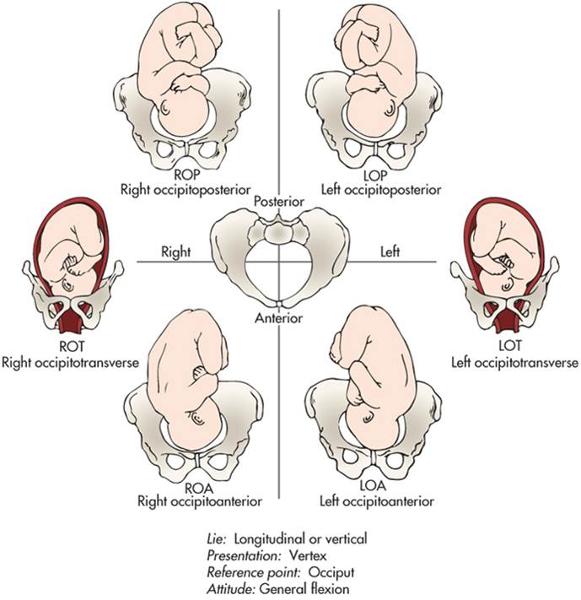 Fetal position : the relationship of a reference point on the presenting part to the four quadrants of the mother’s pelvis Position is denoted by a three-part letter abbreviation Vertex= cephalic/head first. -Roa and loa are most common -ROA- has to do with the bone. -Put heart rate monitor on back . -ROT- -ROP, LOP- posterior. -Transvere and posterior tak e a little longer and it is more uncomfortable. |
front 116 Factors affecting the labor of the passenger: Fetal lie vs Fetal attitude | back 116 Fetal lie : the relation of the long axis (spine) of the fetus to the long axis (spine) of the mother Longitudinal/ Vertical Fetal lie- in relation to long axis of spine in baby and mom - longitudinal/vertical is straight up and down in relationship to mom spine - transverse is horizontal Fetal attitude : the relation of the fetal body parts to one another General flexion |
front 117 Fetal position Fetal Station Fetal Engagement What landmark do we use to measure these? | back 117  Fetal position : the relationship of a reference point on the presenting part to the four quadrants of the mother’s pelvis Position is denoted by a three-part letter abbreviation Fetal station : a measure of the degree of descent of the presenting part of the fetus through the birth canal Fetal engagement : usually corresponds to 0 station *-Ischial spines is important landmark- most narrow diameter that baby needs to go through, talking about station that is the point of reference. O statioin is ischial spines. Anything above is negative. Anything below it is positive. -+4 you usually can see the head. |
front 118 What is the passageway | back 118 Passageway: Birth canal
2 openings, goes into inlet, comes out the outlet (spines, tuberosities and arch) |
front 119 Powers during labor: primary vs secondary and what effects both of these powers | back 119 Powers Primary powers: contractions Frequency, duration, intensity Effacement Dilation Secondary powers: bearing-down efforts Valsalva maneuver Laboring Down |
front 120 Positition and psychologic state of pt affecting labor | back 120 Position of laboring woman Discussed in depth in Chapter 19 Psychologic state of laboring woman Discussed in depth in Chapter 19 |
front 121 The process of labor begins w/ something in the cervix happening? What comes first | back 121 Thinning-->dilation-->decent of fetus |
front 122 How the fetus comes through in labor Mechanism of labor THIS ISIMPORTANT Seven cardinal movements | back 122 Mechanism of labor Turns and adjustments necessary in human birth process Seven cardinal movements of mechanism of labor 1.Engagement 2.Descent 3.Flexion 4.Internal rotation 5.Extension 6.Restitution and external rotation 7.Expulsion |
front 123 Each cardinal movement explained | back 123 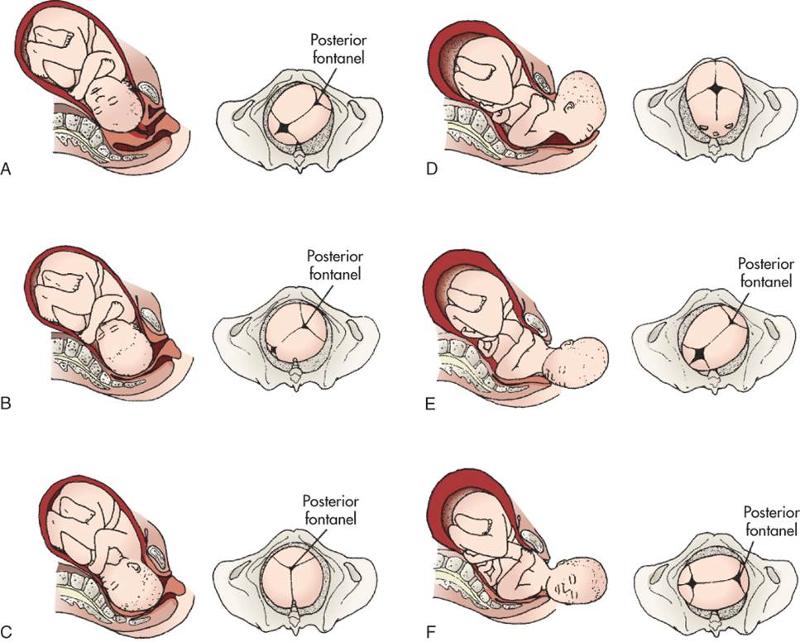 1.Engage: goes through internal inlet. 2.Descent – move down. (0 station is engaged and descended 3. Pelvic muscle flexes neck 4. internally rotaiton of head to get out of bony pelvic outlet 5. Extension of head to say hell 6. Restitution and aligns head with shoulders, head moves back 7. expulsion- baby pops out. |
front 124 cardinal again | back 124
|
front 125 Four stages of labor: know these | back 125 The first stage of labor lasts from the time dilation begins to the time when the cervix is fully dilated. The second stage of labor lasts from the time of full cervical dilation to the birth of the infant. (even if she is laboring down) The third stage of labor lasts from the infant’s birth to the expulsion of the placenta. The fourth stage of labor begins with the delivery of the placenta and includes at least the first 2 hours after birth. (q15 monitoring) |
front 126 5 ps of pregnancy | back 126 Labor and birth are affected by the five Ps: passenger, passageway, powers, position of the woman, and psychologic response. |
front 127 factors affecting pain response in laboring women | back 127 Physiologic factors Culture Anxiety Previous experience Gate-control theory of pain Comfort Support Environment |
front 128 Non pharmacologic pain measures | back 128 Childbirth preparation methods Relaxing and breathing techniques Focusing and relaxation Breathing techniques Effleurage and counterpressure Touch and massage Therapeutic touch Application of heat and cold |
front 129 non pharmaco pain methods | back 129 Acupressure and acupuncture Transcutaneous electrical nerve stimulation Water therapy (hydrotherapy) Intradermal water block Aromatherapy Music Hypnosis Biofeedback |
front 130 Pharm pain methods: anaelgesia vvs. anesthesia | back 130 Anesthesia encompasses analgesia, amnesia, and relaxation Analgesia : the alleviation of the sensation of pain or the raising of the threshold for pain perception without loss of consciousness The type of analgesic or anesthetic chosen is determined in part by the stage of labor of the woman and by the method of birth planned. FENTANYL GREAT |
front 131 Two types of anesthesia | back 131 Systemic analgesia Nerve block analgesia and anesthesia Epidural anesthesia or analgesia (block): currently the most effective pharmacologic pain relief method for labor Combined spinal-epidural (CSE) analgesia: sometimes referred to as a “walking epidural,” although women often choose not to walk because of sedation and fatigue, abnormal sensations in and weakness of the legs, and a feeling of insecurity Epidural and intrathecal (spinal) opioids |
front 132 Nursing guidelines for pharm therapies | back 132 General informed consent Informed consent for anesthesia Timing of administration Preparation for procedures Administration of medication Intravenous route Intramuscular route Regional (epidural or spinal) anesthesia Safety and general care |
front 133 When are sedatives a good idead? What is narcan used for | back 133 Sedatives may be appropriate for women in prolonged early labor when there is a need to decrease anxiety or promote sleep or therapeutic rest. Naloxone (Narcan) is an opioid (narcotic) antagonist that can reverse narcotic effects, especially respiratory depression. Pharmacologic control of pain during labor requires collaboration among the health care providers and the laboring woman. |
front 134 use of an epidural vs general | back 134 Epidural anesthesia and analgesia are the most effective available pharmacologic pain relief methods for labor. General anesthesia is rarely used for vaginal birth but may be used for cesarean birth or whenever rapid anesthesia is needed in an emergency childbirth situation. |
front 135 W/ anesthesia: what happens to moms bp, moms hr, and babies hr | back 135 bp down hr up in mom hr down in baby |
front 136 Different fetal monitoring techniques | back 136 Intermittent auscultation : |
front 137 Electronic fetal monitoring techniques: | back 137 Electronic fetal monitoring (Cont.): |
front 138 Fetal HR patterns: What is baseline HR? | back 138 Baseline fetal heart rate
|
front 139 What is variabilitiy | back 139 uVariability uDescribed as irregular waves or fluctuations in the baseline FHR of two cycles per minute or greater u4 possible categories of variability: uAbsence uMinimal uModerate uMarked |
front 140 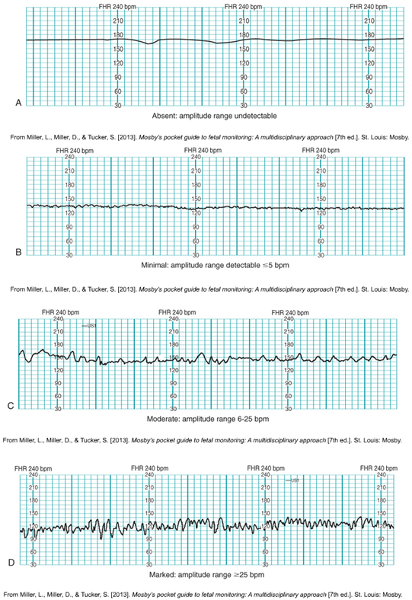 Variability patterns: | back 140 Normal baby- hr fluctuates. A- absent fluctuations, CONCERNED! B: minimal variability- less than 5 bpm change in fluctuation C- 6-25 bpm fluctuations- moderate variability D- Marked-active baby! Dark blue lines a minute Little squares are 10 seconds |
front 141 Another rare finding | back 141  Rare event= IN TROUBLE . Fetal anemia- moms blood type doesn’t match, rh- and + |
front 142 Fetaal tachycardia and bradycardia levels | back 142 Bradycardia= <110. Tahy= >160 |
front 143 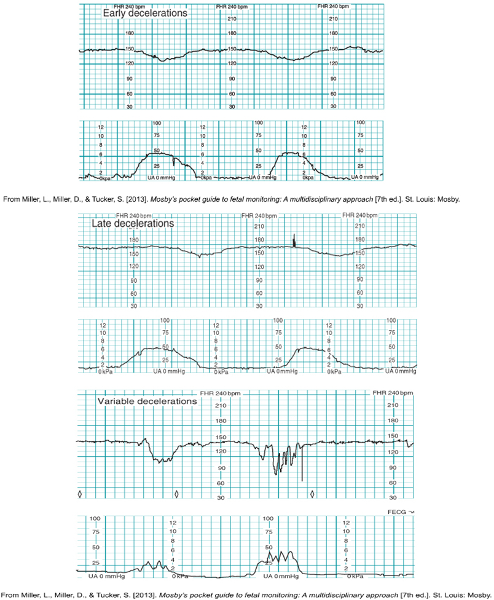 Change in fetal HR : what is a deceleration | back 143 Changes in FHR (Cont.): WORRY- due to blood flow insufficiency: contraction happens, decel happens after the contraction. Variable decelerations due to umbilical cord compression NOT variability, is due to umbilical cord compression. No pattern to variable decels. V for variable- SHARP dip. Baby may be leaning on cord, need to turn mom off of that cord. Prolonged decelerations:; lasting longer, 2 minutes, 5 minutes,2-10min is polonnged, tryin to get her to move, get it to get back up. |
front 144 what is acceleration | back 144
|
front 145 Categories for fetal hr's | back 145 uCategory I: normal uCategory II: indeterminate uCategory III: abnormal |
front 146 Category I | back 146 uBaseline FHR in the normal range of 110-160 beats/min uBaseline fetal heart rate variability: moderate uLate or variable decelerations: absent uEarly decelerations: may be present or absent uAccelerations: either present or absent |
front 147 Category II | back 147 uBradycardia not accompanied by absence of baseline variability uTachycardia uMinimal or absence of baseline variability not accompanied by recurrent decelerations uMarked baseline variability uNo accelerations in response to fetal stimulation uPeriodic or episodic decelerations |
front 148 Category III | back 148 uNonreassuring FHR patterns associated with fetal hypoxemia uHypoxemia can deteriorate to severe fetal hypoxia uAbsence of baseline variability uRecurrent or late decelerations uBradycardia uSinusoidal pattern |
front 149 5 Essential parts to a fetal HR | back 149 The five essential components of the FHR tracing that must be evaluated regularly are baseline rate, baseline variability, accelerations, decelerations, and changes or trends over time. |
front 150 Components of Intrauterine resuscitation | back 150 If any component is abnormal, corrective measures must be taken immediately to improve fetal oxygenation: intrauterine resuscitation Supplemental oxygen Maternal position changes Increasing intravenous fluids |
front 151 1.While evaluating an external monitor tracing of a woman in active labor whose labor is being induced, the nurse notes that the fetal heart rate (FHR) begins to decelerate at the onset of several contractions and returns to baseline before each contraction ends. The nurse should: a.Change the woman’s position b.Discontinue the oxytocin infusion c.Insert an internal monitor d.Document the finding in the client’s record | back 151 D, document this is a normal finding! |