Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
recycle
front 1 he Inpatient Psychiatric Facilities (IPFs) prospective payment methodology for assignment and proper reimbursement. | back 1 icd-9-cm codes |
front 2 A computer software program that assigns appropriate MS-DRGs according to the information provided for each episode of care is called a(n) | back 2 grouper |
front 3 CMS adjusts the Medicare Severity DRGs and the reimbursement rates every | back 3 fiscal year beginning October 1. |
front 4 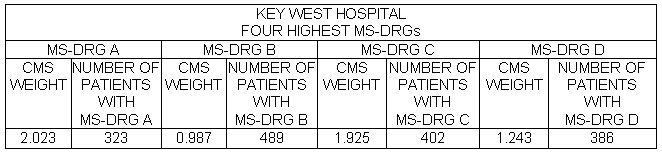 Key West Hospital collected the data displayed above concerning its four highest volume MS-DRGs. Which MS-DRG generated the most revenue for the hospital?
| back 4 MS-DRG C * REMEMBER THE HIGHEST MS-DRG YOU NEED TO MULTIPLY THE PATIENTS AND MS-DRG |
front 5 The prospective payment system used to reimburse hospitals for Medicare hospital outpatients is called | back 5 APC |
front 6 This accounting method attributes a dollar figure to every input required to provide a service. | back 6 COST ACCOUNTING |
front 7 The Correct Coding Initiative (CCI) edits contain a listing of codes under two columns titled "comprehensive codes" and "component codes." According to the CCI edits, when a provider bills Medicare for a procedure that appears in both columns for the same beneficiary on the same date of service
| back 7
|
front 8 A fiscal year is a yearly accounting period. It is the 12-month period on which a budget is planned. The federal fiscal year is | back 8 October 1st through September 30 of the next year |
front 9 This is the amount the facility actually bills for the services it provides. | back 9 CHARGES |
front 10 To compute the reimbursement to a particular hospital for a particular MS-DRG, multiply the hospital's base payment rate by the
| back 10 The relative weight is a number assigned to each MS-DRG published in the Federal Register, and it is used as a multiplier to determine reimbursement. Each hospital's prospective payment system (PPS) rate is a dollar amount based on that hospital's costs of operating as determined by several blended factors. This base payment rate is multiplied by the MS-DRG's (relative) weight to calculate that hospital's reimbursement for a given MS-DRG. Additional payments are made if applicable (such as disproportionate share, teaching hospital, cost outlier, etc.). The prospective payment system used to reimburse the "hospital" for outpatient surgery is APCs. The prospective payment used to reimburse a "free-standing surgery center" for outpatient surgery is ASCs. The prospective payment system used to reimburse the "physician" for outpatient surgery is RBRVS. |
front 11 Under the APC methodology, discounted payments occur when | back 11 there are two or more (multiple) procedures that are assigned to status indicator "T", and modifier-73 is used to indicate a procedure is terminated after the patient is prepared but before anesthesia is started. |
front 12 You are calculating the fee schedule payment amount for physician services covered under Medicare Part B. You already have the relative value unit figure. The only other information you need is | back 12 THE NATIONAL COVERSION FACTOR |
front 13 LIFETIME RESERVE DAYS ARE | back 13
Lifetime reserve days are applicable for hospital inpatient stays that are payable under Medicare Part A, not Medicare Part B. |
front 14 You are starting your new job as the sole HIM professional at a small psychiatric practice. The practice uses DSM for billing purposes. You find this "theoretically" reasonable because DSM | back 14 codes are also valid ICD-10-CM codes. Diagnostic and Statistical Manual of Mental Disorders, (DMS) |
front 15 The Health Insurance Portability and Accountability Act (HIPAA) requires the retention of health insurance claims and accounting records for a minimum of ________ years, unless state law specifies a longer period. | back 15 6 YRS. |
front 16 This is the difference between what is charged and what is paid. | back 16 CONTRATUAL ALLOWANCE |
front 17 The Centers for Medicare and Medicaid Services (CMS) will make an adjustment to the MS-DRG payment for certain conditions that the patient was not admitted with, but were acquired during the hospital stay. Therefore, hospitals are required to report an indicator for each diagnosis. This indicator is referred to as | back 17 PRESENT ON ADMISSION |
front 18 This document is published by the Office of Inspector General (OIG) every year. It details the OIG's focus for Medicare fraud and abuse for that year. It gives health care providers an indication of general and specific areas that are targeted for review. It can be found on the Internet on CMS'Web site. | back 18 OIG'S WORKPLAN |
front 19 Currently, which prospective payment system is used to determine the payment to the physician for outpatient surgery performed on a Medicare patient? | back 19 RBRVS |
front 20 When appropriate, under the outpatient PPS, a hospital can use this CPT code in place of, but not in addition to, a code for a medical visit or emergency department service. | back 20 CRITRICAL CARE |
front 21 When health care providers are found guilty under any of the civil false claims statutes, the Office of Inspector General is responsible for negotiating these settlements and the provider is placed under a | back 21 Corporate Integrity Agreement. |
front 22 HIGHEST TOTAL PROFIT------ can not determine highest total reimbursement------ patients XMS-DRG | back 22 X |
front 23 Some services are performed by a nonphysician practitioner (such as a Physician Assistant). These services are an integral yet incidental component of a physician's treatment. A physician must have personally performed an initial visit and must remain actively involved in the continuing care. Medicare requires direct supervision for these services to be billed. This is called | back 23 INCIDENT TO BILLING |
front 24 Under Medicare Part B, all of the following statements are true and are applicable to nonparticipating physician providers, | back 24
Under Medicare Part B, Congress has mandated special incentives to increase the number of health care providers signing PAR (participating) agreements with Medicare. One of those incentives includes a 5% higher fee schedule for PAR providers than for nonPAR (nonparticipating) providers. |
front 25 In calculating the fee for a physician's reimbursement, the three relative value units are each multiplied by the | back 25 geographic practice cost indices. The three relative value units are physician work, practice expense, and malpractice expense. These are adjusted by multiplying them by the geographical practice cost indices. Then, this total is multiplied by the national conversion factor. |
front 26 The present on admission (POA) indicator is required to be assigned to the ________ diagnosis(es) for ________ claims on ________ admissions. | back 26 principal and secondary, Medicare, inpatient |