Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Chapter 3 (Surgical Tech)
front 1 What is the Primary Role for STSR when interacting with the surgical Pt.? | back 1 assisting the surgeon during the surgical procedure—the establishment and protection of a sterile field, the care and handling of surgical instrumentation, and assistance with technical tasks throughout the surgical procedure. |
front 2 Physical Need of the Patient | back 2 Any need or activity related to genetics, physiology, or anatomy |
front 3 Psychological Need of the Patient | back 3 A mental requirement or necessity for fulfillment as a person |
front 4 Social Need of the Patient | back 4 A need to fit into society and to be accepted by one’s peers |
front 5 Spiritual Need of the Patient | back 5 A need for a connection with a higher order |
front 6 Maslow's hierarchy of needs | back 6 A model developed that expresses human development and progression using developmental stages that prioritize needs establishes a means of prioritizing needs effective for basic understanding of individuals and for quick recognition of patient concerns |
front 7 Understanding the surgical Patient | back 7 Surgical patients are, first and foremost, people. They have a whole life outside the role of patient. That life is at risk with every surgical intervention. The person who is brought into your operating room is not “the hysterectomy in room 5” but rather Jane Doe, single mother of three, bank executive, aspiring vocalist, Episcopalian, African-American, Democrat, practical jokester, and a lot more. Health care is no place for someone who cannot or chooses not to care for the total individual, despite his or her own personal beliefs. One must never “lose sight” of the total person. To do so is to violate the ethical and moral obligations that every health care professional has to every patient. |
front 8 Causes of surgical intervention | back 8 genetic factors, trauma or disease have presented them with a condition that can only be or best be corrected with surgical intervention. Surgery is often the last resort after other treatment options have been exhausted. |
front 9 Human behavior in reaction to health, illness, and hospilization | back 9 varies with age, 2 broad factors are adaptation and stress |
front 10 Cardiac Death | back 10 The irreversible loss of cardiac and respiratory function. This is the permanent absence of heartbeat and respiration. |
front 11 Higher Brain Death | back 11 This is the irreversible loss of higher-brain function. The lower brain stem continues to provide respiration, blood pressure, and a heartbeat without the assistance of a respirator |
front 12 Whole Brain Death | back 12 The irreversible loss of all functions of the entire brain. Whole-brain death is the current law as to what defines death in most jurisdictions of the world and reflects the standard set by the Harvard School of Medicine. It includes a flat EEG, unresponsiveness, lack of pupil reflexes, and low body temperature. |
front 13 What are the five stages of Grief | back 13 Denial, Anger, Bargaining, depression, acceptance |
front 14 Denial | back 14 This is the initial stage. Patients may be saying something such as “It can’t be happening to me.” Denial is usually a temporary defense and a means of coping for the patient. |
front 15 Anger | back 15 When the first stage cannot be continued, it is replaced by feelings of anger, rage, envy, and resentment. The patient is asking, “Why me?” |
front 16 Bargaining | back 16 If a patient has been unable to face the reality and has gone through the stage of being angry, he or she may move to the stage of bargaining to postpone the inevitable. The patient may say, “Just let me live to see my son graduate.” |
front 17 Depression | back 17 When a terminally ill person can no longer deny the illness as it progresses, his or her anger is replaced with a sense of great loss. The patient may be thinking, “Please don’t take me away from my family.” |
front 18 Acceptance | back 18 When a patient has had enough time to work through the first four stages, he or she will reach a stage of being neither depressed nor angry. The statement of resolution may be, “I know I will be in a better place.” |
front 19 Causes of Death | back 19 accidental, terminal, prolonged, sudden |
front 20 Accidental | back 20 These deaths can be caused by nature (floods, lightening, earthquake) or humans (motor vehicle, gunshot). The family is left to deal with the emotional trauma. These cases may engender wrongful death suits. The surgical technologist should be aware of the protocol of preserving evidence. Photographs of hospital scenes or physical injuries to the individual may need to be obtained. |
front 21 Terminal | back 21 A patient who is terminal is suffering from a disease that is progressive and incurable. Death will be the final outcome. Palliative treatment is often prescribed for these patients to improve their quality of life during the course of the illness. These patients often feel they have imposed an economic burden on their family members. Examples of terminal illnesses include metastatic cancer and liver cirrhosis |
front 22 Prolonged | back 22 A condition that is long-lasting (more than 4–6 weeks and in many cases lifelong), and needs to be managed on a long-term basis. Two examples of chronic illnesses are asthma and high blood pressure. These types of illnesses are often managed through lifelong medical treatment. |
front 23 Sudden | back 23 Any death that occurs without warning, such as a cardiac arrest or SIDS (sudden infant death syndrome). |
front 24 Life Support | back 24 refers to a set of therapies that preserve a patient’s life when body systems are not functioning sufficiently to sustain life. may utilize some combination of several techniques including feeding tubes, intravenous drips, total parenteral nutrition, mechanical respiration, heart/lung bypass, defibrillation, urinary catheterization, and dialysis. Life-support therapies can be further broken down into “ordinary” or “extraordinary” means of care |
front 25 Euthanasia | back 25 comes from the Greek for “good death,” and Americans have recast its meaning as “easy death” or “painless inducement of quick death.” |
front 26 Passive (Euthanasia) | back 26 which is when the physician does nothing to preserve life. |
front 27 Active (Euthanasia | back 27 which requires actions that speed the process of dying, such as the administration of morphine. Active euthanasia is further divided into voluntary euthanasia, where the patient initiates facilitation of his or her death, and involuntary euthanasia, where the patient’s autonomous rights are violated. |
front 28 Advance Directives | back 28 general term that refers to one of two legal documents used to speak for patients in the event that they cannot make decisions for themselves. |
front 29 Organ Transplantation and Donation | back 29 began in the early 1950s. Under Title XI of the Omnibus Budget Reconciliation Act of 1986, hospitals are required to establish organ procurement protocols or lose Medicare and Medicaid funding.facility’s Gift of Life Coordinator determines the patient’s suitability for organ donation and organizes the process For patients who were not placed on or were removed from life support, various tissues can be recovered, including:
|
front 30 Prioritizing Needs (Maslow's Hierarchy) | back 30 Maslow (1968, 1971) constructed a model of human development. The developmental stages for human progression are expressed in terms of a hierarchy. The simple but powerful point of the hierarchical structure is that all the requisite needs of each prior level must be met in order to achieve the next leve |
front 31 Physiological Needs | back 31 The most basic needs are biological needs, such as the need for water, oxygen, food, and temperature regulation. |
front 32 Safety Needs | back 32 These needs refer to the perception on the part of the individual that his or her environment is safe. |
front 33 Love and belonging needs | back 33 These are basic social needs—to be known and cared for as an individual and to care for another. |
front 34 esteem needs | back 34 This level of need refers to a positive evaluation of oneself and others, a need to be respected and to respect others. |
front 35 Self Actualization | back 35 This is the need to fulfill what one believes is one’s purpose. |
front 36 Religion and Religious Values | back 36 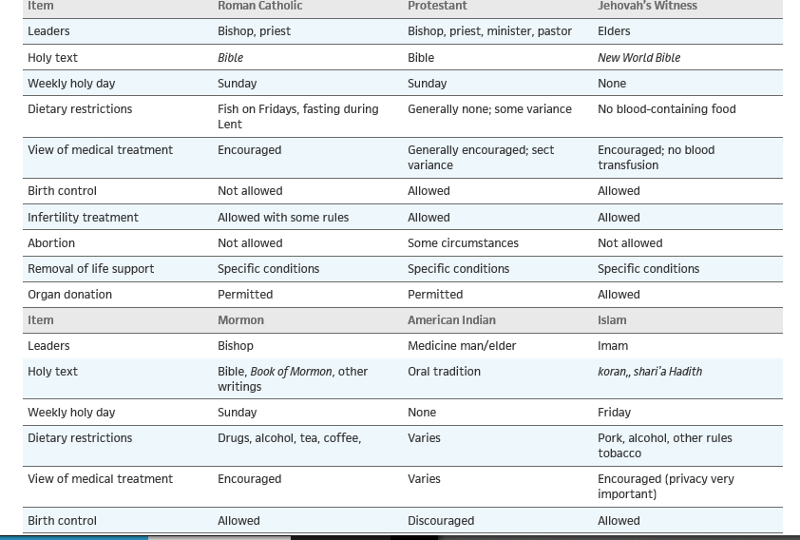 |
front 37 Religious Views and values | back 37 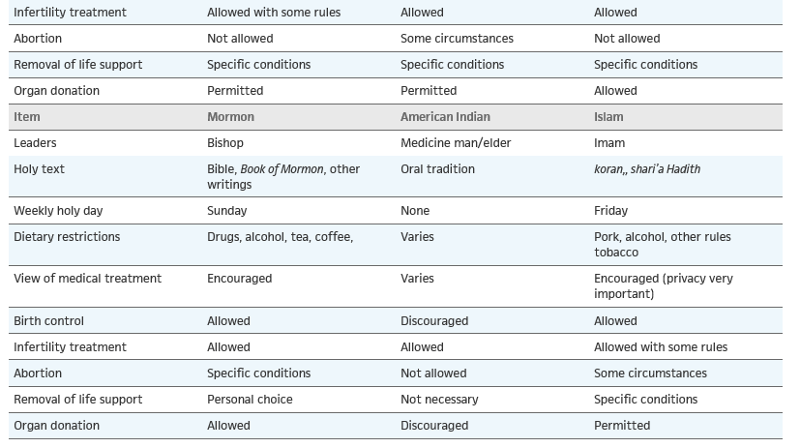 |
front 38 Common Causes for surgery | back 38 Genetic malformationCheiloschisis (cleft lip) Trauma Anterior cruciate ligament tear Nonmalignant neoplasm Uterine fibroid Malignant neoplasm Colon cancer Disease Cholecystitis (gallbladder infection) Condition Kidney stone Psychological stateRhytidectomy (facelift) |
front 39 Who is Sister Callista Roy and what did she do? | back 39 best known for the development of what is referred to as the Roy Adaptation Model. Roy’s model views the patient as a biopsychosocial individual that is constantly interacting with the environment with the ability to adapt by using coping skills in dealing with internal and external stressors. Roy then interprets the environment as “all conditions, circumstances, and influences that surround and affect the development and behaviour of the person |
front 40 most common type of stress | back 40 distress |
front 41 Who is Dr. Hans Selye | back 41 recognized expert in the study of stress, defines stress as a “nonspecific response of the body to a demand” (2006). |
front 42 Factors to be aware of for stressors | back 42
|
front 43 How age can be a stressor | back 43 Pediatric patients feel much more threatened, especially when taken from their parents to be transported to the operating room. Adolescents are much more conscious about their bodies and privacy, whereas older adults are worried about multiple concerns, such as death, infirmity, family, paying the bills, and job security. |
front 44 How environment can be a stressor | back 44 The hospital and surgical environment is definitely not the same as home, and the patient has to quickly adapt to a different schedule, such as waking up by 7:30 a.m. for breakfast, being constantly woken at night postoperatively to take vital signs, etc.How age of pt. can be a stressor |
front 45 how family role can be stressor | back 45 An individual who is the primary “money maker” may now be in a highly dependent role, relying on health care providers; postoperatively he or she may have to rely on other family members for care and assistance. |
front 46 how can economic factors be a stressor? | back 46 How will the bills be paid; how can we take our planned vacation; who is going to pay for the groceries; will I still have a job after a lengthy postoperative recovery? These are the patient’s concerns. |
front 47 how can religious beliefs be a stressor | back 47 Religion can affect attitudes and views of illness, life, and death, and how illness or trauma should be approached. Religious beliefs may determine the treatment options available to the patient. For example, Jehovah’s Witnesses do not believe in or permit the transfusion of whole blood or blood components. |
front 48 Common Types of coping mechanisms | back 48 Denial, rationalization, regression, repression |
front 49 denial | back 49 Patient does not want to accept the truth of what is occurring |
front 50 rationalization | back 50 Patient attempts to rationalize illness or disease. For example, a diabetic patient who is facing amputation of his or her foot due to a gangrenous ulcer may say “diabetes runs on my father’s side of the family.” |
front 51 regression | back 51 Patient regresses to an earlier stage of life, such as adolescence, and exhibits behaviors unique to that stage, such as assuming a fetal position, excessive crying, and pouting. This can also be associated with dependency on others. |
front 52 repression | back 52 Patient represses thoughts and feelings about illness or disease and does not want to hold any discussions concerning what is happening. This can also be associated with escaping or avoiding the situation. |
front 53 Different Types of Spiritual or religious practices and rituals | back 53 Roman Catholic ritual known as Anointing of the Sick may be performed on a seriously ill person. Last rites may be given to Catholic or Protestant patients before death. Muslim tradition might request that immediately after death, the patient’s body be turned east to face Mecca, their holiest city. If the patient is Jewish, the dying patient (goses) should not be left alone. The nurse cannot touch the body until the rabbi offers final rites. After death, a son or relative will close the eyes and mouth of the deceased and wash and dress the body. Buddhists believe in reincarnation and that the last thoughts of a person before death determine the rebirth condition. Hindus feel that cremation is the best way for the soul to begin its journey. |
front 54 Who introduced the stages of grief | back 54 Elizabeth Kubler Ross |
front 55 Living Will | back 55 allows patients to state in writing exactly what medical interventions they are willing to endure to sustain life |
front 56 Power of Attorney | back 56 is a legal way to appoint a health care proxy who will make medical decisions for the patient in the event that he or she cannot do so. |
front 57 A Do Not Resuscitate/Do Not Intubate (DNR/DNI) order | back 57 which is written by a physician, states that resuscitation should not be attempted if a patient suffers a cardiac or respiratory arrest. must be initiated by the patient. is recognized in the medical setting but a patient should re-emphasize if it is to be honored during surgical procedures. during surgery, so this should be discussed with the surgeon, anesthesia provider, and other surgical team members |
front 58 Maslow's Hierarchy of needs | back 58 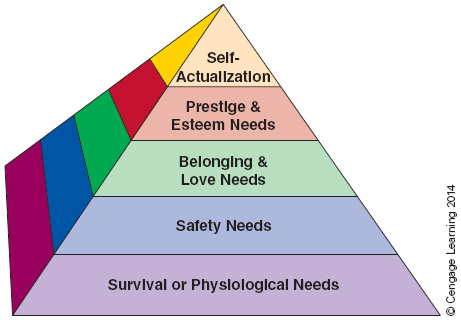 |