Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Neonatal heads
front 1 Reasons for ultrasound exam of the neonatal head | back 1 hemorrhages around lateral ventricle |
front 2 What happen in neonates under 34 weeks? | back 2 intraventricular and subependymal hemorrhages |
front 3 How often do intraventricular and subependymal hemorrhages occur? | back 3 40 to 70% in neonates under 34 weeks |
front 4 What is the most common ischemic lesion in a premie brain? | back 4 Periventricular leukomalacia |
front 5 What is another name for Periventricular leukomalacia? | back 5 multifocal white matter necrosis |
front 6 What is Periventricular leukomalacia? | back 6 when blood vessels burst, blood clots can collect in the white matter |
front 7 What is Periventricular leukomalacia a predictor of? | back 7 Cerebral palsy |
front 8 How often does Periventricular leukomalacia occur? | back 8 12 to 20% in infants weighing less than 2000g |
front 9 Which lobe controls motor function? | back 9 frontal |
front 10 Which lobe controls sensory function? | back 10 parietal |
front 11 Which lobe controls audibility and olfactory function? | back 11 temporal |
front 12 Which lobe controls vision function? | back 12 occipital |
front 13 What controls balance? | back 13 cerebellum |
front 14 Name the fontanelles | back 14 anterior posterior lateral |
front 15 When does the anterior fontanelle close? | back 15 commonly around 6 months |
front 16 What connects the 3rd and 4th ventricle? | back 16  Aqueduct of Sylvius |
front 17 What connects the 4th ventricle and the spinal cord? | back 17  Foramen of Magendie |
front 18 What connects the 4th ventricle and the subarachnoid space? | back 18 foramen of Luschka |
front 19 What forms the roof of the lateral ventricles? | back 19 corpus callosum |
front 20 What is below the corpus callosum and forms the medial walls of the lateral ventricles? | back 20 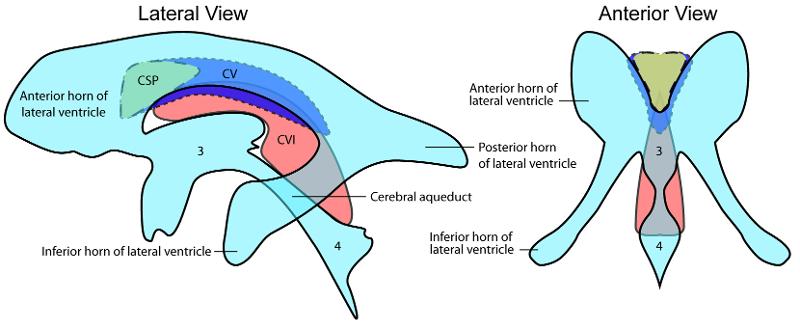 Cavum septum pellucidum CSP |
front 21 Where do all horns of the lateral ventricles merge? | back 21 trigone/atrium region |
front 22 What connects the lateral ventricles and the 3rd ventricle? | back 22  Foramen of Monroe |
front 23 What is the connection between the two hemispheres? | back 23 Messa intermedius |
front 24 What makes up the floor of the 3rd ventricle? | back 24 hypothalamus. |
front 25 What is the narrow subarachnoid space surrounding the brain and spinal cord? | back 25 Cistern |
front 26 What is the largest of the cisterns? | back 26 cisterna magna |
front 27 What does the narrow subarachnoid space surrounding the brain and spinal cord contain? | back 27 CSF |
front 28 The _______, along with the cavum septum pellucidum (CSP) is a persistence of the embryological fluid-filled space between the leaflets of the septum pellucidum | back 28 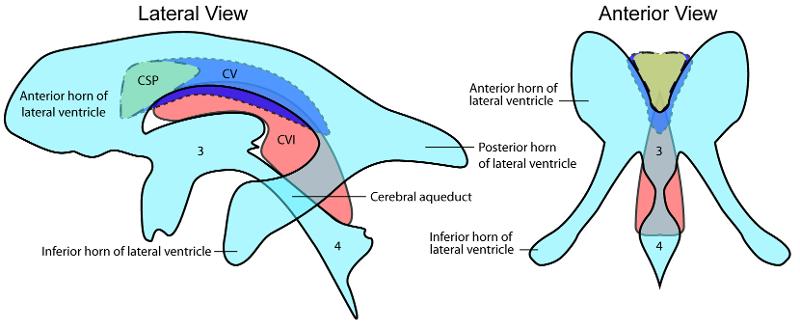 Cavum Vergae |
front 29 What forms the lateral borders of the frontal horns? | back 29 caudate nucleus |
front 30 What does the caudate nucleus consist of? | back 30 head, body and tail |
front 31 Where is a common site for hemorrhage on the caudate nucleus? | back 31 head |
front 32 What does the brain stem consist of? | back 32 midbrain pons medulla oblongata |
front 33 What is the cerebral peduncles responsible for? | back 33 communication between cerebellum and the sensory nerves thalami and cerebellum |
front 34 How is the midbrain divided? | back 34 into two cerebral peduncles |
front 35 Thalami > cerebellum > sensory & balance | back 35 no data |
front 36 Explain the circle of willis. | back 36 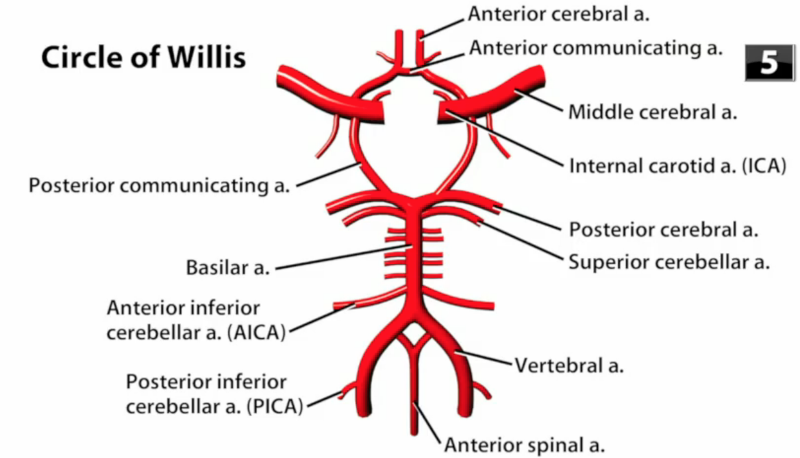 the two vertebral arteries come together to form the basilar artery the basilar divides posterior cerebral artery the internal carotid artery turns into the middle cerebral artery the posterior communicating artery connects the posterior cerebral and the middle cerebral arteries the anterior cerebral artery branches off the middle cerebral artery the anterior communicating artery connects the two anterior cerebral arteries |
front 37 Where does the middle cerebral artery extend? | back 37 into the sylvian fissure Y |
front 38 Why is ultrasound the exam of choice when there is an open fontanelle? | back 38 portable inexpensive non-invasive requires no sedation |
front 39 Which transducer should be used for a neonate head scan? | back 39 5 MHz to 10 MHz phased array is optimal small linear array may also be used |
front 40 Where is the notch pointing during a neonate head scan? | back 40 toward the patients nose |
front 41 In what is the orientation of a sagittal view image of a neonate head scan? | back 41 top - superior - superficial bottom - inferior - deep right - anterior left - posterior |
front 42 In what is the orientation of a coronal view image of a neonate head scan? | back 42 top - superior - superficial bottom - inferior - deep right - left left - right |
front 43 Explain the coronal view image of a neonate head scan. | back 43 slowly angle through the coronal plane beginning rostrally at the frontal lobes angle posteriorly |
front 44 What is the patient prep for a neonatal cranial exam? | back 44 The infant should be disturbed as little as possible. The exam should be done in the neonatal unit. Transducer gel should be body temperature. |
front 45 How do you explain the cranial exam? | back 45 If the parents or guardians are available the sonographer should explain the exam is being performed to visualize the structures of the cranium for possible defects or problems that might arise in the premature infant. |
front 46 How should the patient dress for the exam? | back 46 Keep the infant as warm as possible. |
front 47 What transducer should be used for an infant weighing less than 1500 grams or less than 32 weeks? | back 47 7.5 MHz sector is a good choice but a curve linear transducer may also be used. |
front 48 What transducer should be used when examining a full term infant? | back 48 3 – 5 MHz sector is a good choice but a curve linear transducer may also be used. |
front 49 Explain the cranial procedure. | back 49 Begin doing a full sweep through the anterior fontanelle. Starting perpendicularly with a coronal view, slowly angle the transducer toward the face, scanning through the anterior horns and through the frontal lobes. Then slowly angle toward the occipital lobes and the posterior portion of the cranium and back to perpendicular. Change to a sagittal view, once again beginning perpendicular sweep the transducer toward the right lateral horn and through the temporal lobe and back to perpendicular. Repeat on the left side through the left lateral horn and temporal lobe. Finish back at a perpendicular position. Look for:
After scanning through the brain start taking images. Document the normal anatomy and any pathology found, including measurements and vascularity if indicated |
front 50 What medical history is pertinent to a Neonate cranial exam? | back 50 Sex Gestational Age Weight Family History Anomalies previously found |
front 51 What is the patient position during a neonate cranial exam? | back 51 Supine with the head facing up Prone with head facing the side may be used as necessary |
front 52 What are the scan planes for a neonatal cranial exam? | back 52 Coronal & Sagittal |
front 53 Explain the coronal plane in a neonatal cranial exam? | back 53 Begin perpendicular to the anterior fontanelle, angle the transducer toward the face return midline and sweep the posterior. |
front 54 Explain the sagittal plane in a neonatal cranial exam? | back 54 Begin perpendicular to the anterior fontanelle, Angle the transducer to the right return midline and sweep the left |
front 55 What are the techniques used for a neonatal cranial exam? | back 55 Scanning a baby while they sleep is easier on the patient and easier for scanning |
front 56 Explain the neonatal anatomy | back 56 After the fourth week after conception the neural tube separates into three main structures that will form the brain. These structures include the prosencephalon (forebrain) , mesencephalon (midbrain) and rhombencephalon (hindbrain). The forebrain consists of the cerebrum, thalamus, hypothalamus and the diencephalon. The midbrain will develop into ventricles and the cerebral peduncles. The hindbrain will develop into the cerebellum and the brain stem including the medulla oblongata and pons |
front 57 What is the purpose of the ventricles? | back 57 Four ventricles circulate cerebral spinal fluid around the brain. |
front 58 Explain the anatomy of the lateral ventricles. | back 58 divided into the frontal, occipital and temporal temporal horns. All horns converge at the trigone region. They are filled with cerebral spinal fluid. |
front 59 Explain the anatomy of the third ventricles. | back 59 The third ventricle is a midline structure containing cerebral spinal fluid. It is connected with the lateral ventricles by the foramen of Monroe and to the forth ventricle by the aqueduct of sylvius. |
front 60 Explain the anatomy of the fourth ventricles. | back 60 The fourth ventricle is also filled with cerebral spinal fluid. |
front 61 Explain the anatomy of the Corpus Callosum. | back 61 Lies midline and consists of connective fibers connecting the two hemispheres. It creates the roof of the lateral ventricles and sits superior to the cavum septum. |
front 62 Explain the anatomy of the Cavum Septum Perdiculum and Vergae. | back 62 A midline structure that creates the floor of the corpus callosum. It is filled with cerebral spinal fluid. It sits between the lateral ventricles. It is present at birth but closes around 4 months. |
front 63 Explain the anatomy of the Thalamus. | back 63 The thalamus is an egg-shaped structure. It sits within the 3rd |
front 64 Explain the anatomy of the Cerebellum. | back 64 The cerebellum takes up most of the posterior fossa. The connection between each lobe is called the vermis. |
front 65 Explain the anatomy of the Cisterna Magna. | back 65 Lies posteroinferior to the cerebellum. |
front 66 Explain the anatomy of the Choroid Plexus. | back 66 Consists of two curved structures that wrap around the thalamus. It is responsible for absorbing cerebral spinal fluid. |
front 67 Explain the anatomy of the Aqueduct of Sylvius. | back 67 channels that connects the 3rd and 4th ventricle |
front 68 Explain the anatomy of the Foramen of Monroe. | back 68 channels connecting the lateral ventricle with the 3rd ventricle |
front 69 Explain the anatomy of the Brain Stem. | back 69 Consists of the midbrain, pons and medulla oblongata. This structure connects the spinal cord to the brain. |
front 70 Explain the anatomy of the Interhemispheric Fissure. | back 70 A midline structure where the falx lies between the two hemispheres. |
front 71 Explain the anatomy of the Massa Intermedia. | back 71 A pea-shaped structure within the 3rd |
front 72 Explain the anatomy of the Hippocampal Gyrus (Choroid Fissure). | back 72 spiral-like fold covering the temporal horns. |
front 73 Explain the anatomy of the Cerebral Peduncles. | back 73 Column like structures connected to the pons and the thalamus |
front 74 Explain the anatomy of the Sulci. | back 74 fissures of the brain that separate the folds. |
front 75 Explain the anatomy of the Tentorium. | back 75 echogenic covering that separates the cerebellum from the cerebral. It is part of the dura mater. |
front 76 Explain the anatomy of the Sylvian Fissure. | back 76 A fissure located laterally between the temporal and frontal lobes. The middle cerebral artery lies in this fissure. |
front 77 Explain the anatomy of the Caudate Nucleus. | back 77 located within the concavity of the lateral angles of each ventricle. |
front 78 Explain the anatomy of the Germinal Matrix/Caudothalmic Groove. | back 78 A vascular network located near the caudate nucleus. This is a common site for hemorrhage in the neonate infant. |
front 79 Explain the anatomy of the Quadrigeminal Plate. | back 79 Immediately superior to the superior aspect of the tentorium. |
front 80 What are appropriate reasons for a neonate cranial exam? | back 80 Evaluate the cranial anatomy of a neonate infant for pathology including: anomalies, intracranial hemorrhage, and ventricular dilation Premature Delivery Abnormal posturing Low birth weight Seizers Apnea coma |
front 81 What are the required coronal images? | back 81 Anterior: orbits Anterior: anterior horns and lateral ventricles Middle: lateral ventricles, cavum septum pellucidum, 3rd ventricle, and corpus callosum Posterior: ambient wings of the cisterna magnum Posterior: tentorium and cisterna magnum Posterior: choroid plexus Posterior: glomus of choroids Posterior: occipital lobe |
front 82 What are the required sagittal images? | back 82 Midline: cavum septum pellucidum, corpus callosum, 3rd ventricle and foramen of Monroe, aquaduct of slyvius, 4th ventricle, tentorium, cisterna magna Left Thalamus Left Caudothalamic groove Left Lateral ventricle: anterior, body, and occipital (temporal is hydrocephalic Left Angle slightly lateral from lateral ventricle to show the white matter Left very lateral: Sylvain fissure/ middle cerebral artery Repeat on left side |
front 83 What is the sonographic appearance of the ventricles? | back 83 Two Lateral Ventricles: filled with cerebral spinal fluid and appear as echogenic slits. Third Ventricle: Midline structure, echogenic walls and the center appears anechoic. Forth Ventricle: Midline structure inferior to the third ventricle, echogenic walls and the center appears anechoic. |
front 84 What is the sonographic appearance of the Corpus Callosum? | back 84 midline, echogenic structure, midgray and has medium to low level echoes. |
front 85 What is the sonographic appearance of the Cavum Septum Perdiculum and Vergae? | back 85 appears anechoic, fluid filled structure. Anterior to the corpus callosum |
front 86 What is the sonographic appearance of the Thalamus? | back 86 midline, echogenic structure within the 3rd ventricle |
front 87 What is the sonographic appearance of the Cerebellum? | back 87 vermis is echogenic and the surrounding parenchyma appears midgray |
front 88 What is the sonographic appearance of the Cisterna Magna? | back 88 fluid filled, anechoic structure lays posteroinferior to the cerebellum |
front 89 What is the sonographic appearance of the Choroid Plexus? | back 89 echogenic structures that wrap around the thalamus |
front 90 What is the sonographic appearance of the Aqueduct of Sylvius? | back 90 rarely seen during ultrasound unless dilated |
front 91 What is the sonographic appearance of the Foramen of Monroe? | back 91 channels connecting the lateral ventricle with the 3rd ventricle |
front 92 What is the sonographic appearance of the Brain Stem? | back 92 appears midgray with low echogenicity |
front 93 What is the sonographic appearance of the Interhemispheric Fissure? | back 93 echogenic area separating the two hemispheres |
front 94 What is the sonographic appearance of the Massa Intermedia? | back 94 mid-gray, best seen with ventricular dilatation |
front 95 What is the sonographic appearance of the Hippocampal Gyrus (Choroid Fissure)? | back 95 echogenic, spiral-like fold coving the temporal horn. |
front 96 What is the sonographic appearance of the Cerebral Peduncles? | back 96 Column like structures connected to the pons and the thalamus |
front 97 What is the sonographic appearance of the Sulci? | back 97 echogenic spider- like fissures of the brain that separate the folds. |
front 98 What is the sonographic appearance of the Tentorium? | back 98 echogenic covering that separates the cerebellum from the cerebral. |
front 99 What is the sonographic appearance of the Sylvian Fissure? | back 99 A fissure located laterally between the temporal and frontal lobes. It appears as a Y shape. The middle cerebral artery lies in this fissure. |
front 100 What is the sonographic appearance of the Caudate Nucleus? | back 100 appears midgrey |
front 101 What is the sonographic appearance of the Germinal Matrix/Caudothalmic Groove? | back 101 small echogenic area at the junction of the caudate and the thalamus . hemorrhages are common here. |
front 102 What is the sonographic appearance of the Quadrigeminal Plate? | back 102 echogenic area superior to the tentorium. |
front 103 What is Arnold-Chiari Malformations? | back 103 Congenital anomaly associated with spina bifida. The brain stem and cerebellum are pulled toward the spinal cord, secondary hydocephus develops. |
front 104 What is the sonographic appearance of Arnold-Chiari Malformations? | back 104 Small posterior fossa Myelomeningocele decompression of the ventricle Small cerebellum Absence of the cisterna magna 4th ventricle in low position Absence of the septum pellucidum Widening of the 3rd ventricle Cerebellar tonsil herniation into enlarged foramen magna Displacement of pons and medulla Elongation of 4th ventricle Enlarged massa intermedia 3rd ventricle slightly larger Small anterior horns Enlargement of posterior horns Wide interhemispheric fissure Small posterior fossa Low tentorium Hydrocephalus |
front 105 What are the presenting symptoms of Arnold-Chiari Malformations? | back 105 40 to 75% aqueductal stenosis |
front 106 What is Agenesis of the Corpus Callosum? | back 106  Partial or complete agenesis is often seen with heterotopias and polymicrogyria. |
front 107 What is the sonographic appearance of Agenesis of the Corpus Callosum? | back 107  Narrow frontal horns Separation of the anterior horns Widening of the occipital horns Widening of the 3rd ventricles 3rd ventricles have pointed upper corners (bat-wings) |
front 108 What are the presenting symptoms of Agenesis of the Corpus Callosum? | back 108  poor muscle tone porencephaly hydrocephalus microgyria Arnold-Chiari fusion of the hemispheres. |
front 109 What is Dandy-Walker Malformation? | back 109 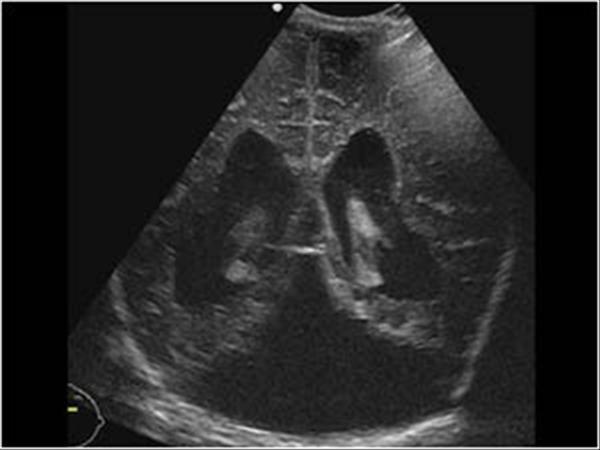 A congenital anomaly in which a 4th ventricle cyst occupies the cerebellar space. |
front 110 What is the sonographic appearance of Dandy-Walker Malformation? | back 110 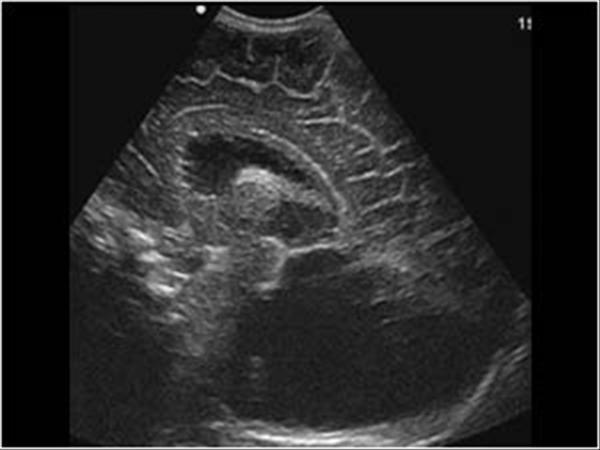 Hydroplasia of cerebellar vermis Enlarged 4th ventricle Cysts in posterior fossa Small brain stem Hydrocephalus Atresia of the Luschka and Magendie 4th ventricle communicates directly to cysts Obstruction above and below 4th ventricle Absence of Corpus Callosum |
front 111 What are the presenting symptoms of Dandy-Walker Malformation? | back 111 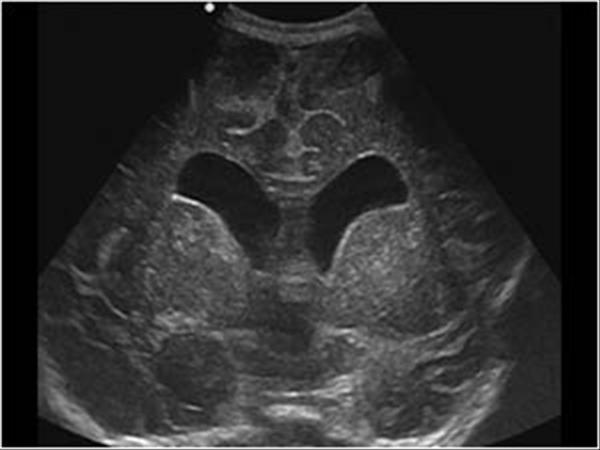 hydrocephalus agenesis of the corpus callosum encephalocele holoprosencephaly microcephaly infundibular hamartomas brain stem lipomas. |
front 112 What is Holoprosencephaly? | back 112  Complex abnormality from failure of cleavage of the prosencephalon *Must obtain modified coronal studies of the whole frontal lobe to determine if frontal horns are present |
front 113 What is Alobar Holoprosencephaly? | back 113 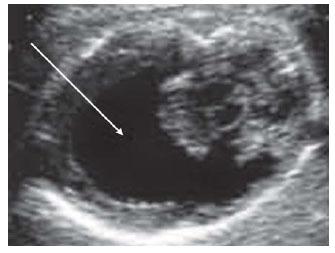 The most severe form of Holoprosencephaly |
front 114 What is the sonographic appearance of Alobar Holoprosencephaly? | back 114 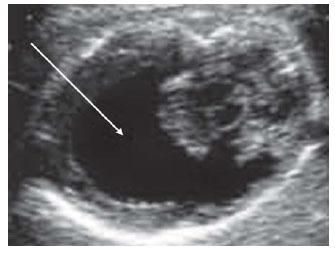 Single midline ventricle Thin, primitive cerebral cortex Fused Thalami and hemispheres , hyper echogenic choroid plexus Absent corpus callosum & interhemiphermic fissure, 3rd ventricle Large dorsal cyst |
front 115 What are the presenting symptoms of Alobar Holoprosencephaly? | back 115 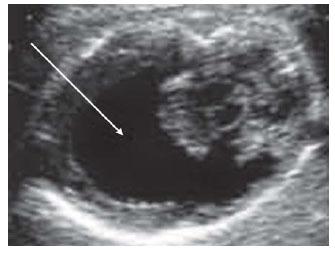 Multiple facial abnormalities
|
front 116 What is Semilobar Holoprosencephaly? | back 116  Characterized by the abnormal storage and collection of glycogen in the tissue of the liver and kidneys. |
front 117 What is the sonographic appearance of Semilobar Holoprosencephaly? | back 117  Single ventricle More brain parenchyma present Posterior faux and interhemispheric fissure Splenium and genu seen midline 3rd ventricle is small |
front 118 What are the presenting symptoms of Semilobar Holoprosencephaly? | back 118  Mild facial
|
front 119 What is lobar Holoprosencephaly? | back 119  Least severe form |
front 120 What is the sonographic appearance of lobar Holoprosencephaly? | back 120 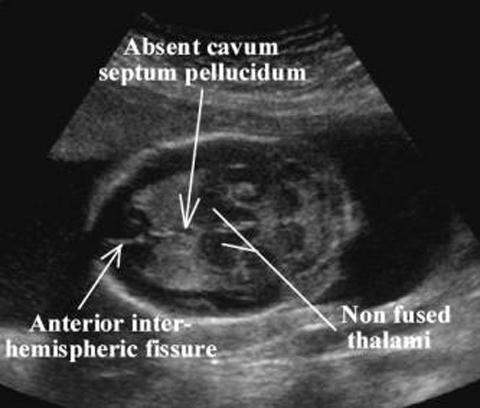 Nearly complete separation of hemispheres Faux and interhemispheric fissure development Some front lobe fusion Absent septum pellucidum Anterior horns fused Occipital horns separation 3rd ventricle separates the thalami Absent genu |
front 121 What are the presenting symptoms of lobar Holoprosencephaly? | back 121  mild facial abnormalities |
front 122 What is Ischemic Lesions: ? | back 122 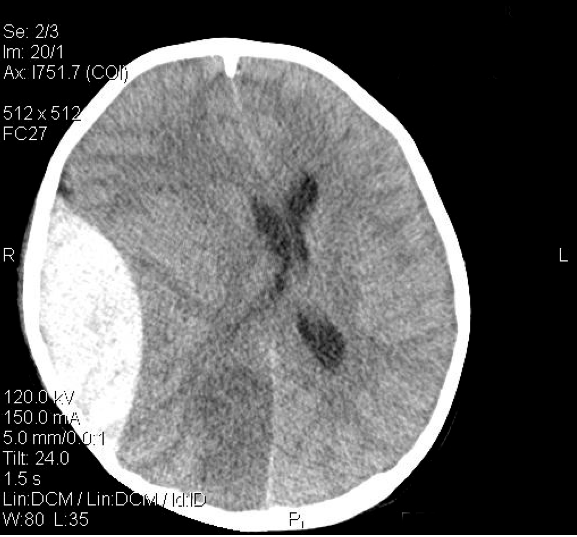 Lesions in the midline that induce malformations of the telencephalon |
front 123 What is the sonographic appearance of Ischemic Lesions: ? | back 123  Single ventricle cavity Absent corpus callosum * Presence frontal horns helps differentiate between Holoprosencephaly |
front 124 What are the presenting symptoms of Ischemic Lesions: ? | back 124 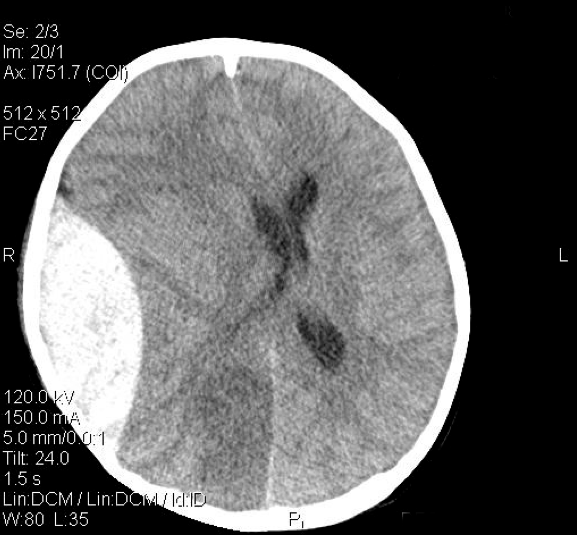 Gastrointestinal bleeding blood in the stools vomiting of blood Encephalopathy |
front 125 What is Porencephalic? | back 125 Also known as porencephaly, is a cyst filled with cerebral spinal fluid. May be caused by hemorrhage , infarction, trauma, inflammation of the nervous system. |
front 126 What is the sonographic appearance of Porencephalic? | back 126 Cyst without mass Reduction of hemisphere Midline shift Contralateral ventricular enlargement |
front 127 What is Hydranencephaly? | back 127 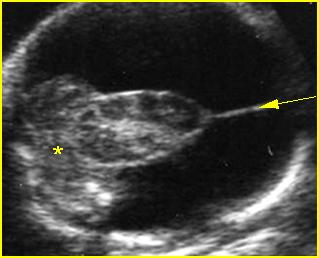 Brain development is destroyed and preplaced with cerebral spinal fluid. May be caused by bilateral occlusion of the internal carotid |
front 128 What is the sonographic appearance of Hydranencephaly? | back 128 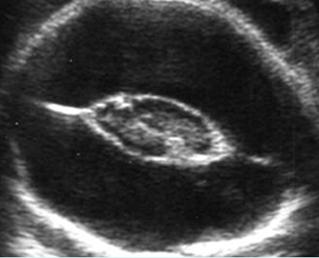 Midbrain, basal ganglia, choroid plexus, and thalamus sparing Presence of cerebral spinal fluid Absent Doppler flow in carotid Possible absent falx cerebri |
front 129 What is Congenital Hydrocephalus? | back 129 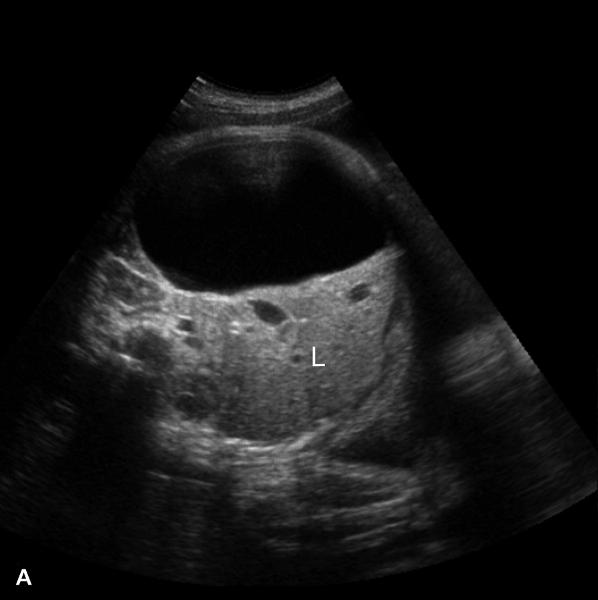 An imbalance of production and absorption of cerebral spinal fluid. There are three types: obstruction to outflow, decreased absorption, or rarely overproduction. |
front 130 What is the sonographic appearance of Congenital Hydrocephalus? | back 130  Blunting of the lateral angles of the lateral ventricle Widening of the ventricle system Rare choroid plexus cyst |
front 131 What are the presenting symptoms of Congenital Hydrocephalus? | back 131  enlargement of head, bulging fontanelles |
front 132 What is Obstructive Hydrocephalus? | back 132 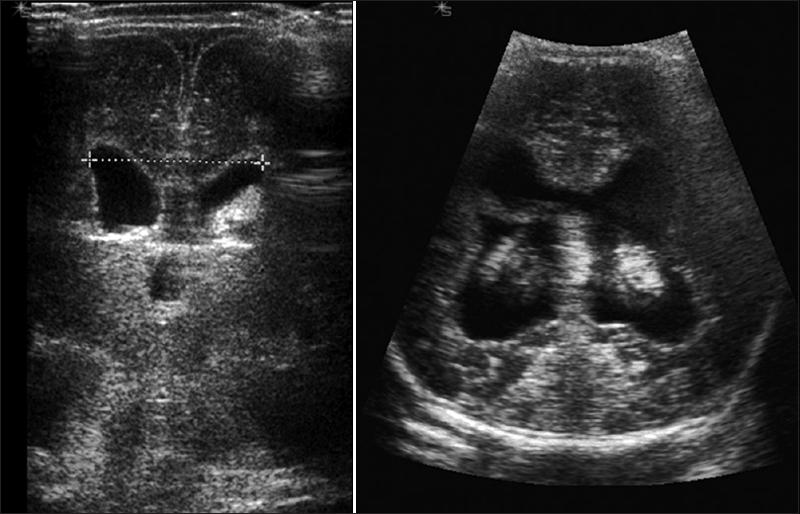 interference of cerebral flow |
front 133 What is the sonographic appearance of Obstructive Hydrocephalus? | back 133 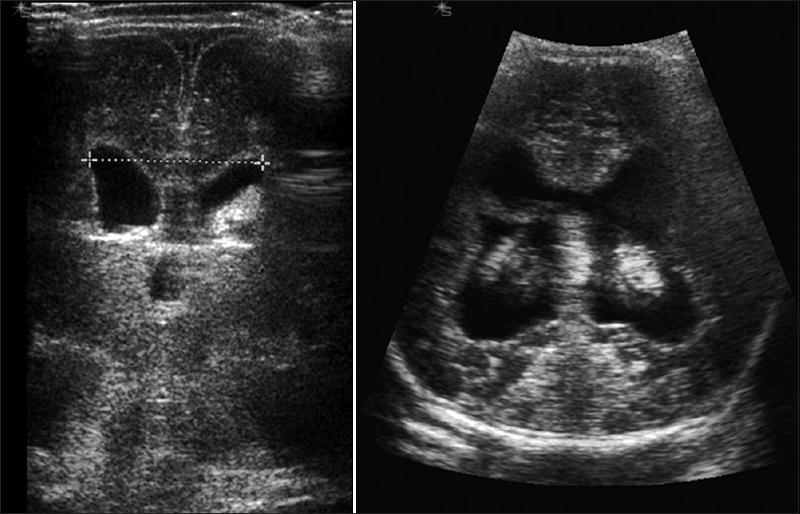 Enlargement of proximal ventricle cavity |
front 134 What is Communicating Hydrocephalus? | back 134 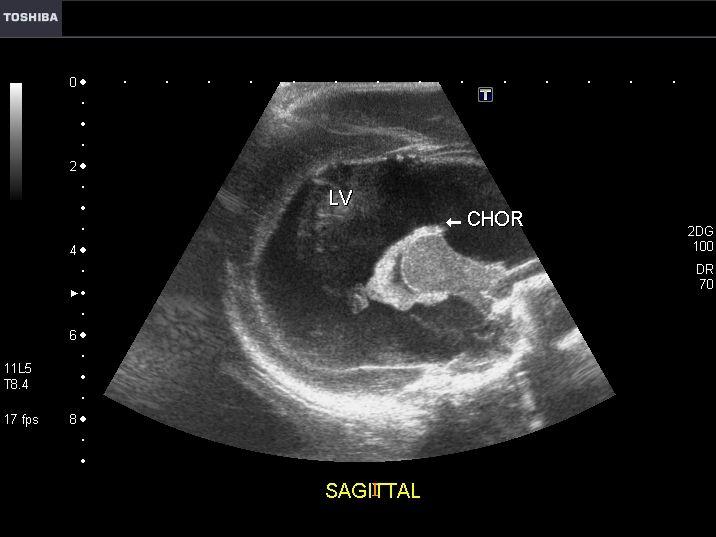 pathway of cerebral fluid are open but there is a decrease in absorption. The ventricular system becomes uniformly distended. The most common cause is aquaduct stenosis. |
front 135 What is the sonographic appearance of Communicating Hydrocephalus? | back 135 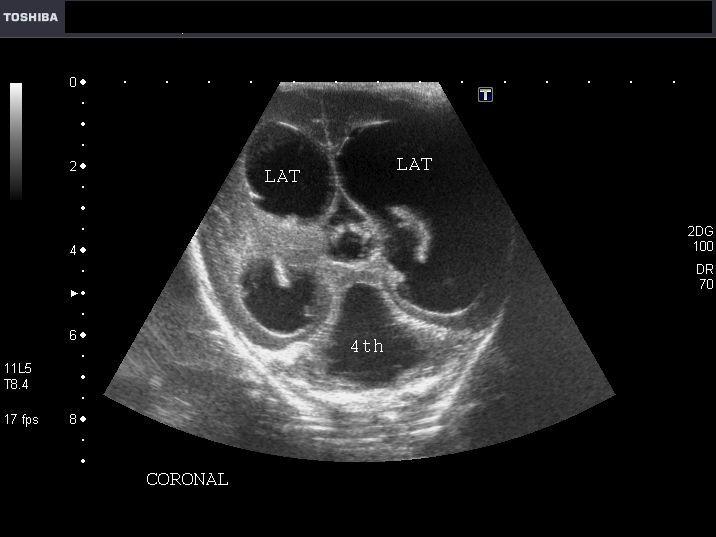 Narrow aqueduct of Slyvius may be replaced by small network Widening of lateral ventricles Normal size 4th ventricle Small posterior fossa Cerebellum displaced posteriorly Absent cisterna magna |
front 136 What is Subarachnoid Cysts? | back 136  lined by arachnoid tissue and contain cerebral spinal fluid. |
front 137 What is the sonographic appearance of Subarachnoid Cysts? | back 137 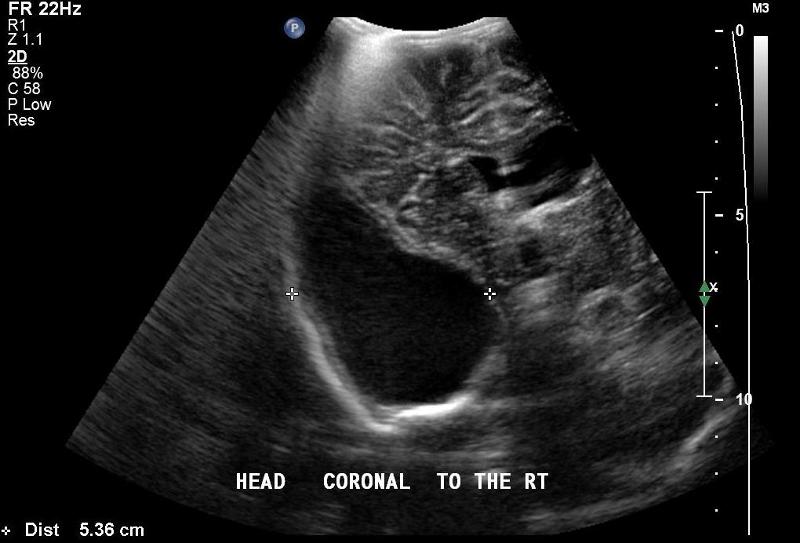 Normal vermis (Not Dandy- Walker) Sonolucent Verify with color Doppler Interhemispheric cysts Suprasellar cysts Cerebral convexity cysts |
front 138 What is Choroid Plexus cysts? | back 138  A hepatic cyst is usually a solitary, non-parasitic cyst of the liver. solitary or multiple. |
front 139 What is the sonographic appearance of Choroid Plexus cysts? | back 139  Common and single Well-defined Anechoic mass Unilateral Left larger than right 4 to 7 mm *Rare Multiple cysts larger than 10 mm associated with trisomy 18 |
front 140 What is Subependymal cysts? | back 140 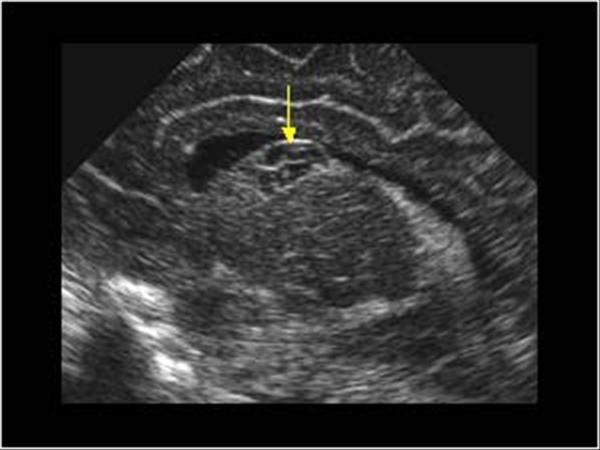 Discrete in the lining of the ventricle. Commonly the result of sequel of germinal matrix |
front 141 What is the sonographic appearance of Subependymal cysts? | back 141 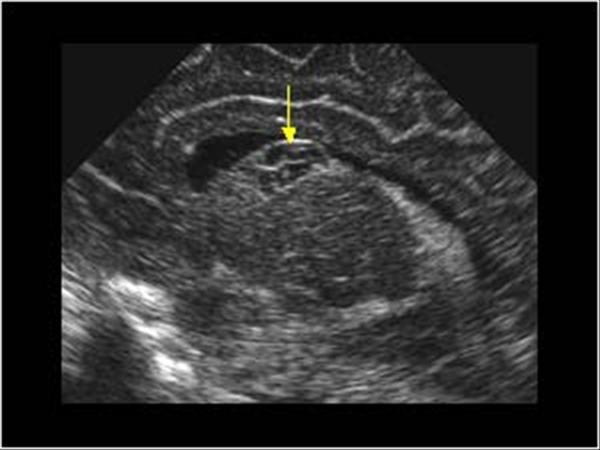 Smooth walled Spherical Located in lateral ventricle |
front 142 What is Galenic Venous Malformation? | back 142 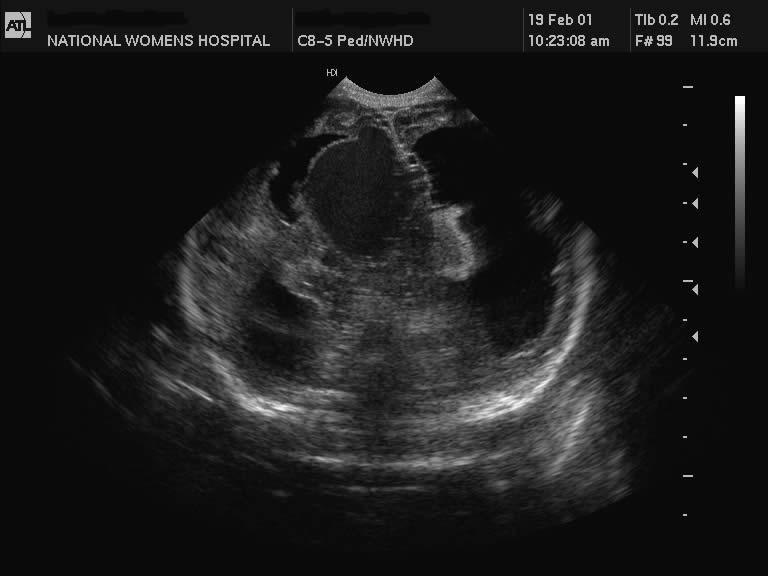 Dilation of the vein of Galen, caused by vascular malformation off the posterior cerebral. |
front 143 What is the sonographic appearance of Galenic Venous Malformation? | back 143  Anechoic cystic Between lateral ventricles Calcification Hydrocephaly with possible thrombus |
front 144 What is Subependymal-Intraventricular Hemorrhages? | back 144 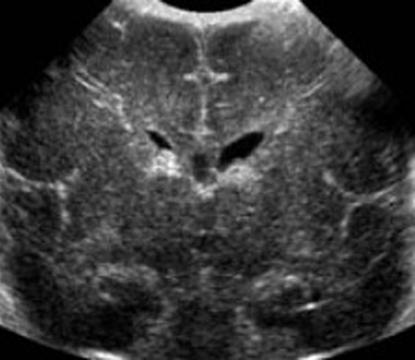 Most common hemorrhage in preterm, affecting 30 to 50% of infants born before 32 weeks. The most common site is the interthalmic groove. Can cause obstruction in the choroid plexus. |
front 145 What is the sonographic appearance of Subependymal-Intraventricular Hemorrhages? | back 145 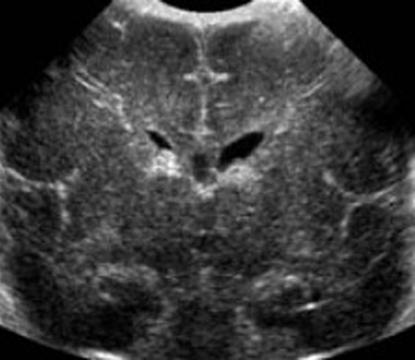 Fluid Echogenic structure in white matter Become cystic and are absorbed leaving cavity |
front 146 What is Intraparenchymal Hemorrhages? | back 146 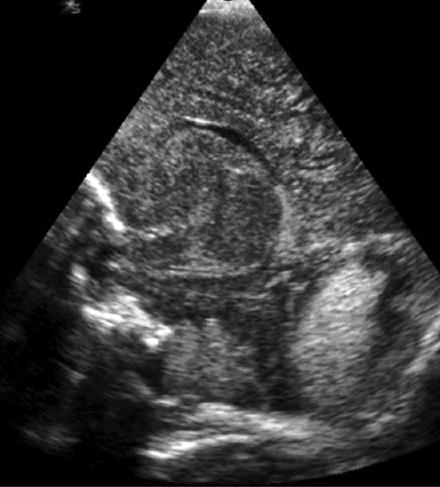 Complicate Subependymal hemorrhage, meaning brain tissue has been |
front 147 What is Intracerebellar Hemorrhages? | back 147 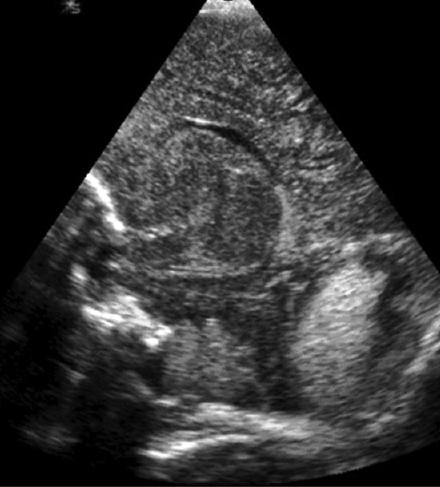 Difficult to find in live infants. Primmary: intracerebellar, venous infarction, traumatic laceration – resulting from occipital diastasis, extension to the cerebellum of a large SHE-IVH |
front 148 What is the sonographic appearance of Intracerebellar Hemorrhages? | back 148 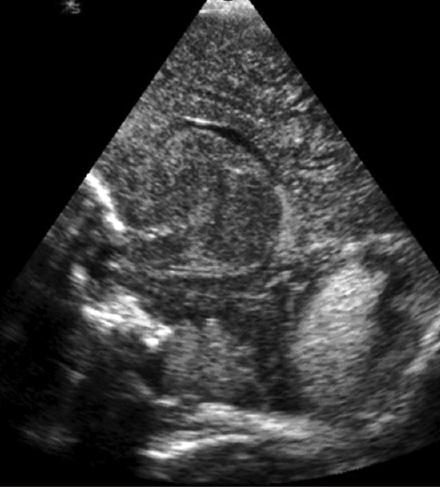 Echogenic structures Within the less echogenic cerebellar parenchyma Become cystic with time leaving cavity lesions |
front 149 What is Epidural Hemorrhages? | back 149 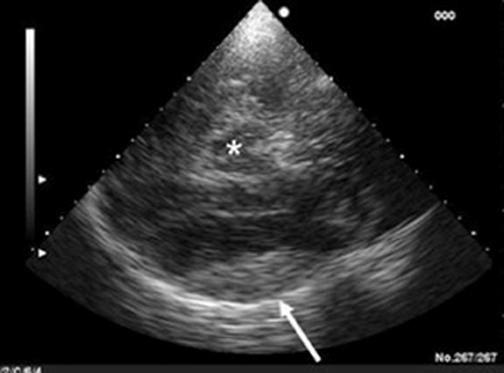 Better diagnosed with CT. located peripherally along the surface of the brain. |
front 150 What is the sonographic appearance of Epidural Hemorrhages? | back 150 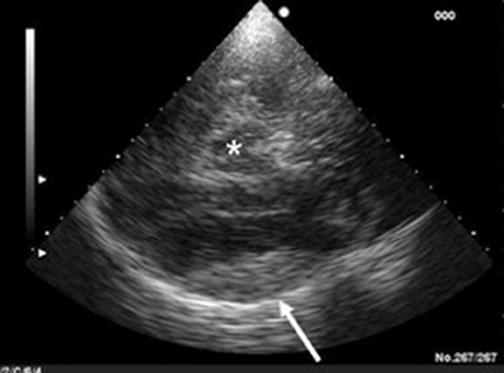 Nonechogenic spaces Between the echogenic calvarium and the cortex |
front 151 What are the presenting symptoms of Epidural Hemorrhages? | back 151 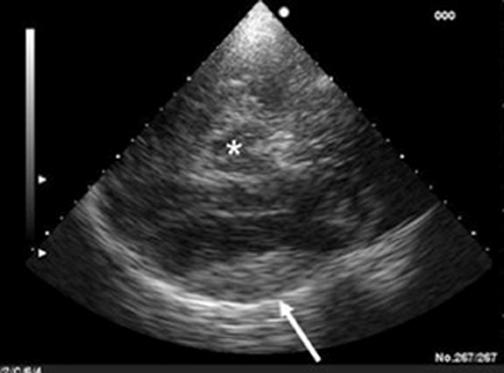 persistent |
front 152 What is Periventricular Leukomalacia? | back 152  Also called Multifocal White Matter Necrosis, most common ischemic lesion in the immature brain. Highly echogenic areas in the white matter. |
front 153 What is the sonographic appearance of Periventricular Leukomalacia? | back 153  echolucencies in white matter |
front 154 What are the presenting symptoms of Periventricular Leukomalacia? | back 154 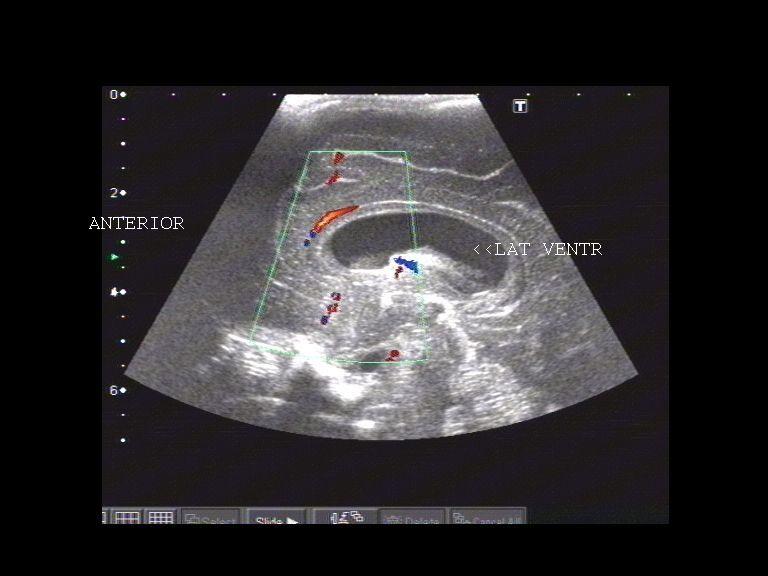 Associated with Cerebral Palsy |
front 155 What is Focal Brain Necrosis? | back 155  occur within large arteries. Early on cause destruction of cerebral tissue and leave cavitary lesions. These lesions correspond to cerebral infarction. |
front 156 What is the sonographic appearance of Focal Brain Necrosis? | back 156  Echogenic localized lesions Sonolucencies appear after few days |
front 157 What is Ventriculitis? | back 157  A common complication of purulent meningitis. This is probably caused by infection spreading to the choroid plexus. Stents and other objects placed the body can cause this infection. Can lead to hydrocephalon |
front 158 What is the sonographic appearance of Ventriculitis? | back 158  Thin septations extending from lateral ventricles. Septations thicken |