| back 1 smooth muscle- fibers are small and lack striations
cardiac muscle- fibers are striated, but they are smaller than skeletal, branched, and uninucleated
skeletal muscle- fibers are large, ,ultinucleate cells that appear striped or striated under a microscope |
| back 2 - fiber are small and lack striations
Internal organs and tubes
Stomach, bladder, blood vessels
Move materials in body
Lack of banding (striations) results from less organized arrangement of contractile fibers within the muscle cells |
| back 3 fibers are striated, but they are smaller, branched, and uninucleate
• Cells are joined in series by junctions called intercalated disks
• Found only in heart
• Controls blood movement through circulatory system |
front 4 2 properties in common in all muscle types | back 4 The signal to initiate muscle contraction is an intracellular calcium signal
Movement is created when myosin (a motor protein) uses energy from ATP to change its conformation |
front 5 skeletal muscle contraction | back 5 Contract only in response to a signal from a somatic motor neuron
• Cannot initiate their own contraction and not influenced by hormones |
front 6 antagonistic muscle groups | back 6 - contain pairs of flexors and extensors
• Flexion- moves bones closer together when the muscle contracts
• Extension- moves bones away from each other when the muscle contracts |
front 7 Sarcoplasmic Reticulum (SR) | back 7 - a form of modified endoplasmic reticulum that wraps around each myofibril like a piece of lace
o Concentrates and sequesters CA2+ in the SR membrane
o Ca2+ release from the SR creates calcium signals that play a key role in contraction in all types of muscle |
| back 8 highly organized bundles of contractile and elastic proteins that carry out the work of contraction and are the main intracellular structures in striated muscles
o > 1000 myofibrils per muscle fiber
o Made up of: contractile proteins, regulatory proteins, and giant accessory proteins
o Made up of thick filaments and thin filaments |
front 9 Myofibril thick and thin filaments | back 9 Thick filaments-250 myosin molecules joined together
Thin filaments- made up of actin proteins
Myosin Crossbridges form between filaments to connect thick and thin filaments
• 2 states of crossbridges: low force (relaxed muscles) and high force (contracting muscles) |
| back 10 - One repeat of a light and dark band
o Z disk – where thin filaments attach
o I band – only have thin filaments
o A band – length of thick filament
o H zone – only have thick filaments
o M line – proteins that form the attachment site where thick filaments attach |
front 11 skeletal muscle calcium signaling | back 11 Ca2+ levels increase in the cytosol
Ca2+ binds to troponin (TN)
troponin- Ca2+ complex pulls tropomyosin (turns muscle contraction on and off with Ca2+ signaling) away from actin's myosin-binding site
myosin binds strongly to actin and completes power stroke
actin filament moves |
| back 12 • Myosin bound to actin, no ATP bound to myosin
• Normally very short period of time because the muscle fiber has a sufficient supply of ATP the quickly binds to myosin once ADP is released by the myosin |
front 13 the muscle contraction cycle | back 13 ATP binds to myosin. Myosin releases actin
myosin hydrolyzes ATP. Energy from ATP rotates the myosin head to the cocked position. Myosin binds weakly to actin
power stroke begins when tropomyosin moves off the binding site
myosin releases ADP at the end of the power stroke |
front 14 excitation-contraction coupling in skeletal muscle(4 key events) | back 14 acetylcholine released (ACh) from somatic motor neuron
ACh initiates action potential (AP) in muscle fiber
AP triggers Ca2+ release from the sarcoplasmic reticulum
Ca2+ triggers muscle contraction
faster Ca2+ is pumped back to the SR the faster the muscle twitch |
| back 15 one contraction-relaxation cycle in a skeletal fiber |
| back 16 delay between action potential and contraction |
| back 17 reversible condition in which a muscle is no longer able to generate or sustain
• Perception of a decline in mental function
• Gradual decrease of force capacity of muscle
• Endpoint of sustained activity
• Highly variable
• Two fatigue mechanisms
o Central, Peripheral |
front 18 2 types of muscle fatigue | back 18 central- CNS
• Perception of a decline in mental function
Peripheral- between neuromuscular junction and contractile elements of the muscle
• Gradual decrease of force capacity of muscle |
front 19 3 muscle types appearance under a light microscope and fiber arrangement and tissue morphology | back 19 skeletal- striated, sarcomeres, multinucleate, large, cylindrical fibers
smooth- smooth, no sarcomeres, uninucleate, small spindle-shaped fibers
cardiac- striated, sarcomeres, uninucleate, shorter branching fibers |
| back 20 skeletal- attached to bones, a few sphincters close off hollow organs
smooth- forms the walls of hollow organs and tubes, some sphincters
cardiac- heart muscle |
front 21 3 muscle types fiber proteins | back 21 skeletal- actin, myosin, troponin, and tropomyosin
smooth- actin, myosin, tropomyosin
cardiac- actin, myosin, troponin, and tropomyosin |
| back 22 skeletal- Ca2+ and troponin, fibers independent of one another
smooth- Ca2+ and calmodulin, some fibers electrically linked via gap junctions; others independent
cardiac- Ca2+ and troponin, fibers electrically linked via gap junctions |
front 23 3 muscle types contraction speed and force | back 23 skeletal- fastest, not graded (all or nothing)
smooth- slowest, gradient
cardiac- intermediate, graded |
front 24 3 muscle types initiation of contraction | back 24 skeletal- requires ACh from motor neuron
smooth- stretch, chemical signals. can be autorhythmic
cardiac- autorhythmic |
front 25 3 muscle types neural and hormonal influence of contraction | back 25 skeletal- somatic motor neuron, no hormonal influence
smooth- autonomic neurons, multiple hormones
cardiac- autonomic neurons, epinephrine |
front 26 muscle fiber classification | back 26 • Muscle fiber classification
o Slow twitch(type I)= skeletal muscle (involved in posture)
Slow-twitch muscle fibers are much more resistant to fatigue than fast-twitch
o Fast twitch (type II)= explosive movements (jumping)
Oxidative-glycolytic (type IIA, Red muscle)
Glycolytic (type IIB, white muscle)
o Muscles are a mix of the 2 types |
front 27 muscle fiber type metabolism | back 27 slow twitch oxidative- oxidative, aerobic
fast twitch oxidative-glycolytic- glycolytic, but becomes more oxidative with endurance training
fast twitch glycolytic- glycolytic, more anaerobic than fast twitch oxidative-glycolytic type |
front 28 oxidative vs glycolytic muscle fibers | back 28 Oxidative- more Myoglobin, more capillaries, smaller in diameter, maintain a better supply of oxygen than glycolytic fibers
White muscle- glycolytic fibers with a lower myoglobin content |
| back 29 red oxygen-binding pigment with a high affinity for oxygen that helps facilitate the diffusion of oxygen into muscle fibers to reach the mitochondria
mostly found in slow-twitch muscle |
front 30 sarcomere length and tension (sliding filament theory) | back 30 o Resting length directly related to the tension
o Sliding filament theory- the tension a muscle fiber can generate is directly proportional to the number of crossbridges formed between the thick and thin filaments |
| back 31 - maximum level of contraction
o Single twitch does not represent the maximum force that a muscle fiber can develop
o Force generated by the contraction of a single muscle fiber can be increased by increasing the rate (frequency) at which the action potentials stimulate the muscle fiber |
front 32 types of muscle twitch/tetanus | back 32 single twitched- muscle relaxes completely between stimuli
summation- stimuli closer together do not allow the muscle to relax fully
summation leading to unfused tetanus- stimuli are far enough apart to allow muscle to relax slightly between stimuli
summation leading to complete tetanus- muscle reaches steady contraction. if muscle fatigues, tension decreases rapidly |
| back 33 - basic unit of contraction in an intact skeletal muscle
o Somatic motor neuron + all muscle fibers it innervates
o Made of same muscle fiber type (fast and slow twitch)
During embryonic development, somatic motor neuron secretes a growth hormone that dictates muscle fiber type
o You can change your proportion of slow and fast-twitch
o The force of contraction in a skeletal muscle can be increased by recruiting additional motor units |
| back 34 o Isotonic- shortening muscle fibers by contraction and causing movement
o Isometric- contracts muscle, but doesn’t shorten it and doesn’t cause movement |
front 35 skeletal muscle cotraction | back 35 Sarcomeres shorten
Elastic elements stretch
When the sarcomeres shorten in an isometric contraction, the elastic elements stretch allowing the fibers to maintain a relatively constant length even though the sarcomeres are shortening and creating tension |
| back 36 • Hyperexcitability of somatic motor neurons
• Stretching sends sensory info to CNS to inhibit somatic motor neuron |
front 37 smooth muscle contraction patterns | back 37 tonic- continuously contracted
phasic- cycles of contraction and relaxation |
front 38 smooth muscle communication | back 38 • Single-unit smooth muscle cells- connected by gap junctions and the cells contract as a single unit
• Multi-unit smooth muscle cells- not electrically linked and each cell must be stimulated independently |
front 39 smooth vs skeletal muscle differences | back 39 • Variable muscle length
• Muscle layers may run in different directions
• Contract & relax more slowly
• Uses less energy for contraction
• Sustained contractions without fatigue
• Cell morphology – small, spindle-shaped cells
• Contractile fibers are not arranged in sarcomeres
• Contraction can be stimulated by chemical or electrical signals
• Controlled by autonomic nervous system
• Lacks specialized receptor regions
• Ca2+ comes from ECF & from SR
• Ca2+ acts as a signaling molecule to start a cascade
• More actin
• Filaments run length of cell
• Longer myosin filaments with more heads |
front 40 smooth muscle contraction | back 40 • Increase in cytosolic Ca2+ from both ECF & SR
• Ca2+ binds to calmodulin in the cytosol
• Binding signals cascade ending in phosphorylation of myosin light chains
• Phosphorylation increases myosin ATPase activity causing contraction |
| back 41 consists of axon terminals, motor end plates on the membrane and Schwann cells |
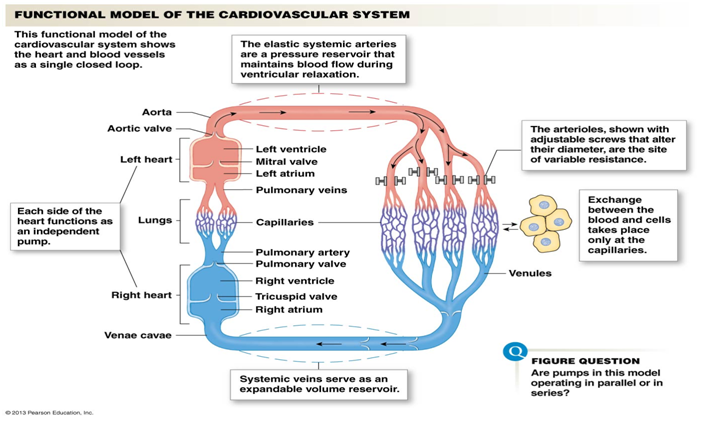
| back 42 right atrium to right ventricle to lungs, from lungs to left atrium to left ventricle to the aorta which branches into capillaries, leaves capillaries and flows into the venous side of circulation from small veins to larger veins, back to the right atrium |
| back 43 -larger artery that branches into a series of smaller arteries then to capillaries
where oxygen leaves the blood and diffuses into tissues |
| back 44 veins from the upper part of the body that join and empty into the right atrium |
| back 45 veins from the lower part of the body that join and empty into the right atrium |
| back 46 the blood vessels that carry blood from the left side of the heart to the tissues and back to the right side of the heart |
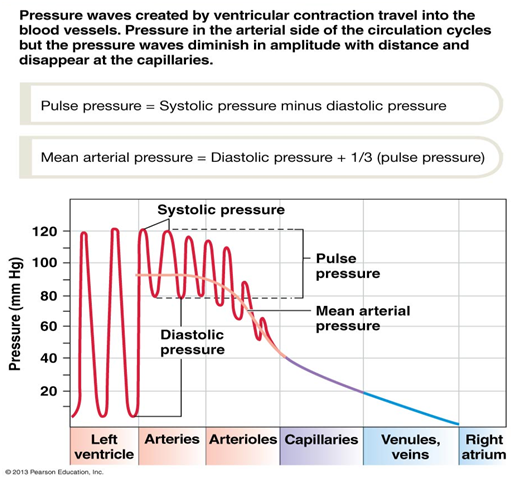
front 47 blood vessels ranked from high to low pressure | back 47 aorta, arteries, arterioles, capillaries, venules, veins, venus carvae (superior and inferior vena cava) |
front 48 types of pressure (hydrostatic and driving) | back 48 • Hydrostatic pressure – fluid is not moving, force is exerted equally in all directions
o Driving pressure- the pressure created in the ventricles that drives blood through the blood vessels |
| back 49 Flow is proportional to Pressure (P)/Resistance (R)
higher pressure gradient= more fluid flow
if resistance (opposition to blood flow) increases, flow decreases
R is proportional to Length of tube*viscosity of fluid/(radius (r) of tube)^4
R is proportional to 1/r^4 |
| back 50 heart lies in the center of the thorax inside the pericardium (fluid-filled sac for lubrication)
myocardium- cardiac muscle that comprises the heart
aorta and pulmonary trunk emerge from the base of the heart |
front 51 atrioventricular (AV) valve | back 51 o Between atria & ventricles
o During ventricular contraction, the AV valves remain closed to prevent blood flow backwards into the atria |
| back 52 o Between ventricles & arteries
o The semilunar valves prevent blood that has entered the arteries from flowing back into the ventricles during ventricular relaxation |
| back 53 o In between skeletal and smooth muscle
o Branched cells
o Striated, sarcomeres
o Single nucleus
o Attached by intercalated disks (gap junctions to pass electrical signals quickly)
o Generate force to be passed on to multiple cells
o Most of heart are cardiac muscle cells (myocardium)
o 1% of myocardial cells are specialized to generate action potentials |
front 54 autorhythmic/pacemaker cells | back 54 - set the rate of the heartbeat by speed and repolarization
• Smaller than contractile/myocardial cells and contain few contractile fibers
no rest, constantly cyclic
unstable membrane potential
spontaneously fire action potentials and depolarization spreads quickly to adjacent contractile cells through gap junctions |
front 55 cardiac and skeletal muscle differences | back 55 Smaller than skeletal muscles and have only one nucleus per fiber
Intercalated disks join cells together
Connected by gap junctions
Large t-tubules- Concern that all muscle fibers signal to go off at the same time
Smaller sarcoplasmic reticulum (SR)
Uses intra (from SR) & extracellular Ca2+ signaling
1/3 of cell volume = mitochondria
aerobic respiration drives cardiac cells |
front 56 excitation-contraction coupling in cardiac muscle | back 56 • Action potential enters and Ca2+ channels open and Ca2++ enters the cell
• Ca2+ induces a Ca2+ release through channels which causes a spark which sum to create a signal
• Ca2+ binding to Troponin initiates contraction until it unbinds and causes relaxation
• Ca2+ is pumped back to the SR for storage and is exchanged with Na+ to maintain the Na+ gradient |
front 57 cardiac muscle contraction gradient | back 57 contraction dependent on recruitment of active crossbridges (more Ca2_ in the cell, the more crossbridges will form)
also dependent on sarcomere length (based on tension) |
front 58 action potential of a cardiac contractile cell | back 58 Na+ channels open (potential increases, depolarization)
Na+ channels close (potential is at a peak, initial repolarization)
Ca2+ channels open, fast K+ channels close (potential decreases then levels out, the plateau)
Ca2+ channels close, slow K+ channels open (potential decreases, rapid repolarization)
resting potential |
front 59 refractory period in cardiac muscle | back 59 long refractory period (lasts almost as long as the entire muscle twitch) prevents tetanus |
front 60 primary functions of the cardiovascular system | back 60 transport
take in materials (from external environment, oxygen, nutrients)
move materials within the body (cell to cell, hormones, nutrients, white blood cells, antibodies)
cells remove wastes(CO2, metabolic wastes)
circulate heat |
| back 61 ventral wall that divides the heart into left and right halves |
| back 62 independent pump in each half of the heart
• Receives blood returning from the heart from the blood vessels |
| back 63 - independent pump on each side of the heart
• Pumps blood out into the blood vessels |
front 64 right vs left side of the heart | back 64 Right side of the heart- Receives blood from the tissues and sends it to the lungs for oxygenation
Left side of the heart- Receives newly oxygenated blood from the lungs and pumps it to the tissues throughout the body |
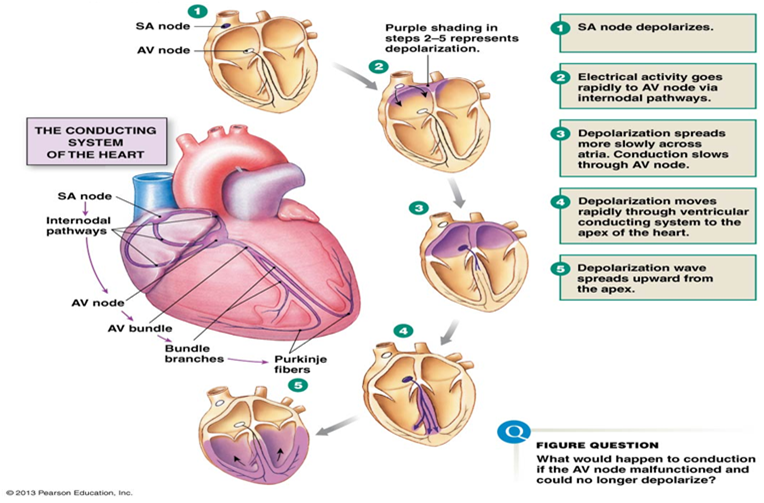
front 65 conducting system of the heart | back 65 SA node depolarizes
electrical activity goes rapidly to AV node via internodal pathways
depolarization spreads more slowly across atria. conduction slows through AV node
depolarization moves rapidly through ventricular conducting system to the apex of the heart
depolarization wave spreads upward from the apex |
| back 66 slow down the transmission of action potentials slightly to allow the atria to complete the contraction before ventricular contraction begins |
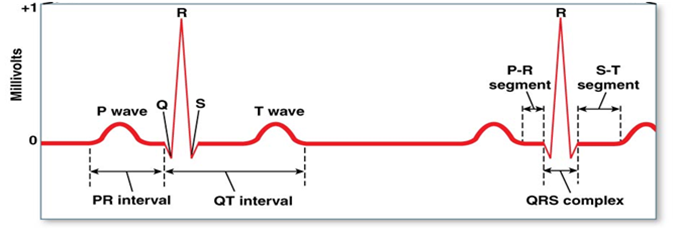
| back 67 • P wave- depolarization of the atria
• QRS complex- progressive wave of ventricular depolarization
o Includes atrial repolarization
• T wave- repolarization of the ventricles |
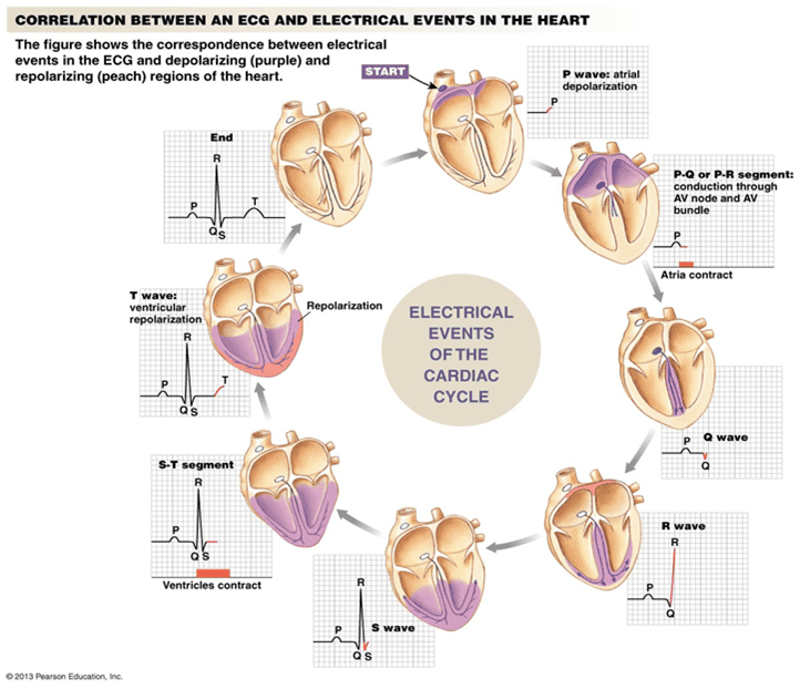
front 68 ecg and electrical events of the heart (image) | back 68 electrical events slightly preceding mechanical events |
front 69 heart contraction and relaxation cycle | back 69 contraction- systolic
relaxation- diastolic |
| |
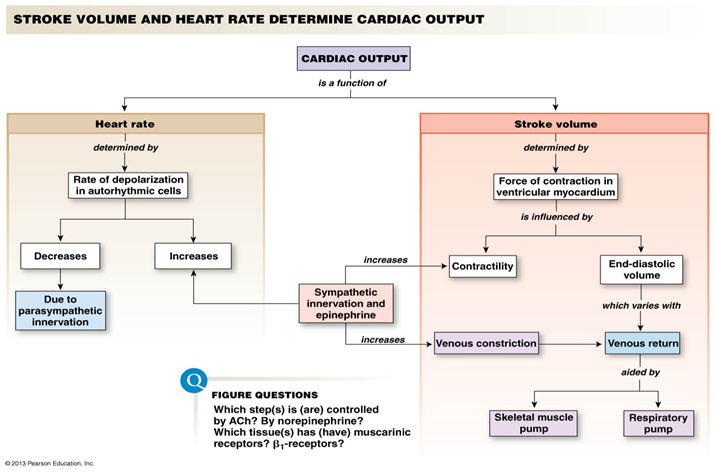
| back 71 amount of blood pumped by one ventricle during a contraction
more contraction force= increased stroke volume
longer muscle fiber or increase in end-diastolic volume= greater stroke volume |
| back 72 the volume of blood pumped by one ventricle in a given period of time
CO= heart rate* stroke volume
indicator of total blood flow throughout the body |
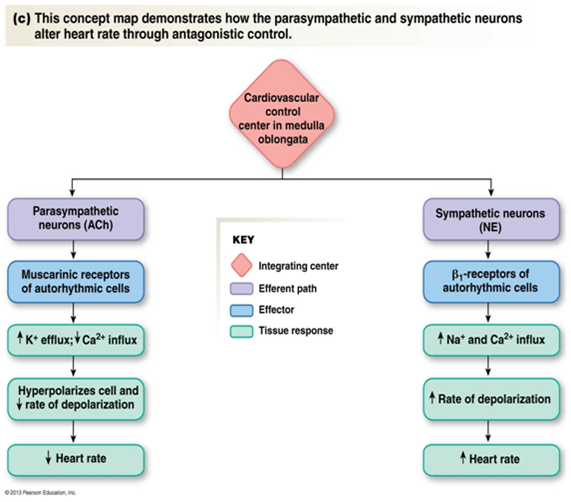
front 73 sympathetic and parasympathetic control of heart rate | back 73 antagonistic control
dominant control from autonomic control system |
front 74 autonomic heart regulation/control | back 74 • Parasympathetic branch is dominant for tonic control (dominant for heart rate)
o to speed up heart rate: Block parasympathetic branch or Increase sympathetic input
• Both affect conduction through AV node |
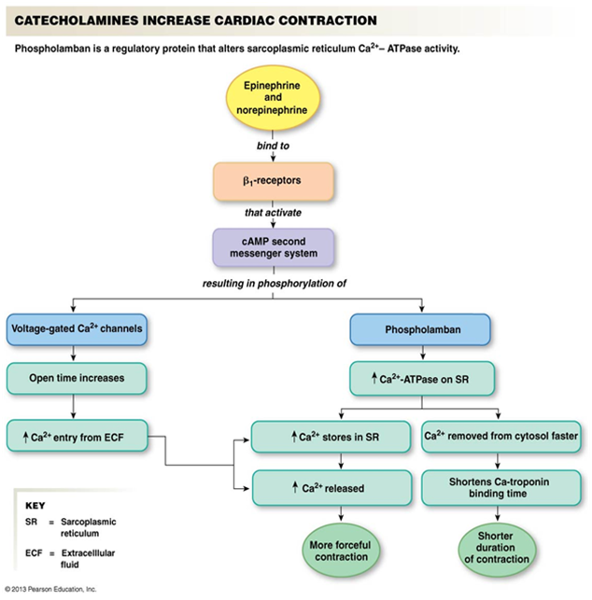
front 75 endocrine system effect on heart rate | |
front 76 cardiac output (summary image) | |
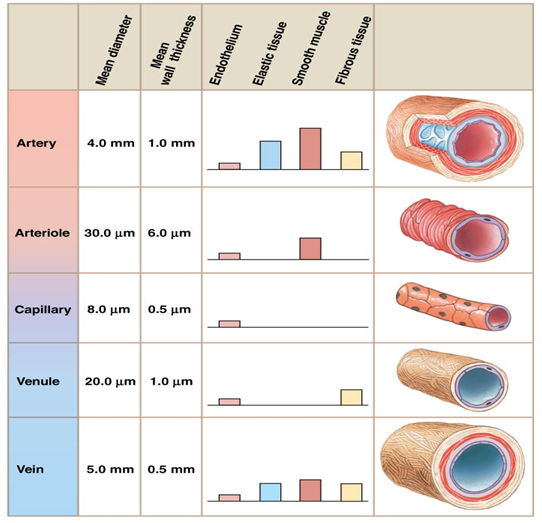
front 77 blood vessel size and composition | |
front 78 functional model of the cardiovascular system | |
| back 79 muscle rings
can close off capillaries in response to local signals
when they are relaxed, blood flows through all capillaries in the bed
if they constrict, blood flow bypasses capillaries completely and flows through the metarterioles (act as bypass channels) |
| back 80 - smallest vessels in the cardiovascular system
• One cell layer of endothelium thick (no smooth muscle or fibrous tissue reinforcement)
• Site of exchange between blood & interstitial fluid
• Relatively simple tissue compared to arteries and veins
• Contain pericytes
found in muscle, connective tissue, and neural tissue
continuous, varying degrees of leakiness (allow water and small, dissolved solutes to pass) |
| back 81 highly branched contractile cells
found in capillaries and form a mesh-like layer that limits the flow out of the capillary bed
o The more pericytes the less leaky the capillary endothelium
o Have the potential to become new smooth muscle cells or endothelial cells |
| back 82 - small vessels
o Small venules are similar to capillaries except they have their own convergent pattern of flow
o Larger venules begin to have smooth muscle |
| back 83 o More veins than arteries
o Veins are larger in diameter than veins
o Veins run closer to the surface |
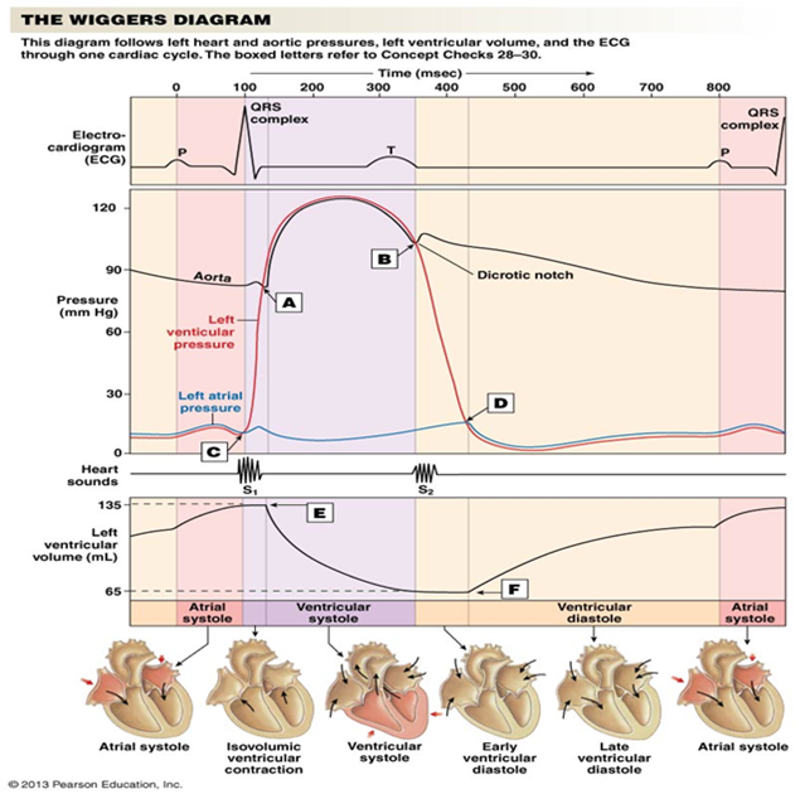
front 84 ventricular contraction and relaxation in arteries | back 84 ventricular contraction- contraction of the ventricles pushes open the semilunar valve and pushes blood into the elastic arteries, causing them to stretch and store pressure in their elastic walls
ventricular contraction- elastic recoil and a shut semilunar valve sends the blood forward into the rest of the circulatory system during isovolumic ventricular relaxation |
| |
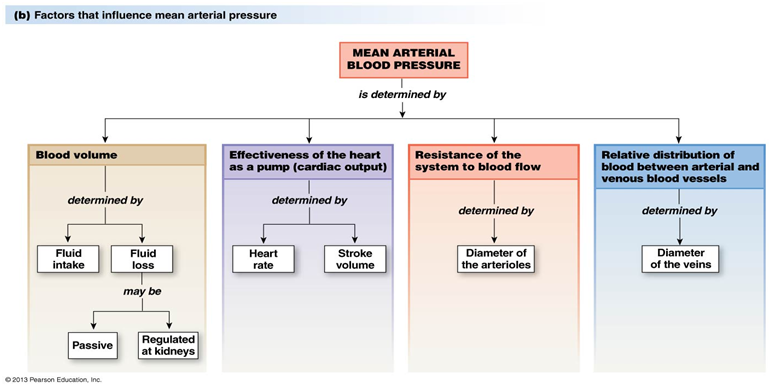
front 86 mean arteriole blood pressure | back 86 MAP= systolic + 1/3(systolic-diastolic)
o a single value that reflects the driving pressure created by the pumping action of the heart and reflects the ventricular pressure |
| back 87 • Vascular smooth muscle can autoregulate its contraction
Increased blood pressure normally à Increased blood flow
•Provide stimulus to stretch receptors in arterioles, increased blood brought in causes a response to vasoconstrict to keep the blood moving through the same (homeostasis)
o Voltage gated channels
• Within arteriole walls |
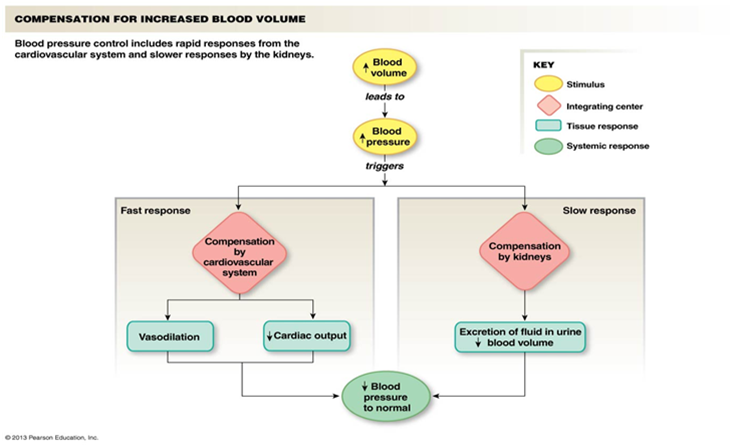
front 88 compensation for increased blood volume | |
| back 89 o Local
Precapillary sphincters, Myogenic autoregulation, Paracrine signals
o Long distance, Sympathetic branch, Epinephrine, CVCC (cardiovascular central control)
Goal: Keep adequate blood flow to brain & heart by maintaining sufficient mean arteriole pressure (maintain homeostasis)
Other Influences
• Chemoreceptors for low O2, Hypothalamus (temperature), cerebral cortex (emotion, thought), Fluid regulation in kidneys |
| |
front 91 Epinephrine and NE effects on arteriole diameter | back 91 Epinephrine from the adrenal medulla also affects arteriole diameter
• Binds to alpha receptors (highest affinity for NE, but Epinephrine also binds), but not with as high affinity as norepinephrine à vasoconstriction (vasodilation for epinephrine)
• Binds to beta receptors in the smooth muscle of heart, liver & skeletal muscle arterioles à vasodilation |
| back 92 - stretch sensitive mechanoreceptors located in the walls of the carotid arteries and aorta, where they monitor the pressure of blood flowing to the brain and the body
o Change in pressure, etc act as signals
o Acts very quickly (ex. 2 heartbeats can produce a change in pressure) |
| back 93 have large pores (fenestrae) that allow bigger molecules to pass through unchecked
found in kidney and intestine |
| back 94 Modified vessels that act like capillaries
Found in bone marrow & liver
Large, wide vessels
Very leaky- 5x as wide as normal capillaries
Little or no regulation in exchange |
| back 95 • Water and gases (small molecules) can pass relatively freely
• Chemical equilibrium (proteins, water fluids) is developed in the capillaries
• Larger molecules (including selected proteins) are transported across the endothelium by transcytosis
velocity slows in capillaries and total area is larger to allow time for exchange |
| back 96 • Functions of the lymphatic system:
o Returns fluid & proteins filtered out of capillaries to circulatory system
o Picking up fat absorbed at the small intestine and transferring it to the circulatory system
o Serving as a filter to help capture and destroy foreign pathogens |
| back 97 • Plasma- fluid matrix of the blood, within which cellular elements are suspended
o Water (92%), Proteins (7%), Other (1%)
o Plasma is identical to interstitial fluid except for the presence of plasma proteins
Albumins are the most common type
source of all plasma proteins is the liver |
| back 98 red blood cells (erythrocytes)- transport a lot of O2 and CO2
white blood cells (leukocytes)- immune response within tissues
platelets (thrombocytes)- wound healing and clotting |
front 99 categories of white blood cells | back 99 • Phagocytes- engulfing foreign particles
• Immunocytes- responsible for specific immune response directed against invaders
• Granulocytes- contain cytoplasmic inclusions that give them a granular appearance
• All blood cell types have relatively short half lives (especially leukocytes) |
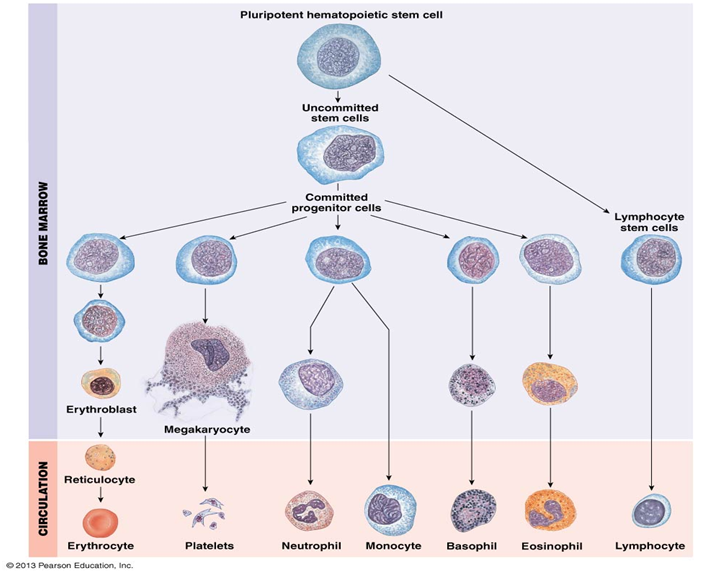
front 100 pluripotent hematopoietic stem cells | back 100 - a blood stem cell that can differentiate into more committed cells
o Found primarily in bone marrow
• Self renewal- cell produces at least one offspring
• Expansion of a population of cells
o Instead of just replacing the one cell, the population will grow via cell division
• Keep creating these stem cells throughout life |
front 101 cytokines involved in hematopoiesis | back 101 erythropoletin (EPO)- produced in kidney cells and influences the growth of red blood cells (abused by lance armstrong)
thrombopoietin (TPO)- produced in liver and influences the growth of megakaryocytes (become platelets) |
| back 102 most abundance cell in your body
no nucleus (cannot make new proteins or replace them as they degrade
• Shape needs to be flexible to get through capillary beds
• Hypertonic- shrink in, get spiky appearance
• Hypotonic- become a sphere
contain thousands of hemoglobin |
| back 103 contain 4 heme groups, each with an iron center that can bind to an O2
each hemoglobin can bind to 4 O2
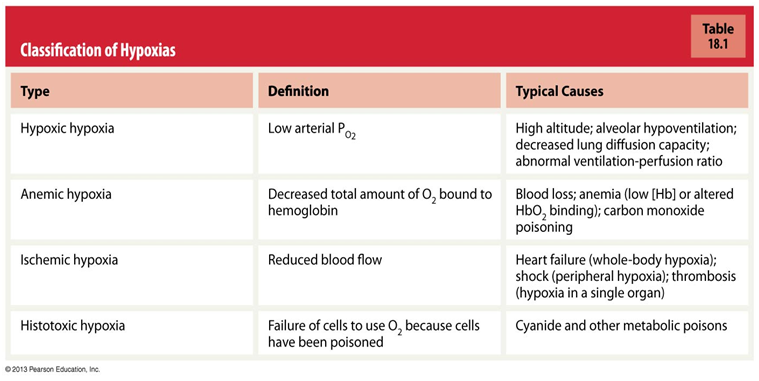
anemia- low hemoglobin |
| back 104 giant cells with multiple copies of DNA in the nucleus
the edges break off to form cell fragments called platelets |
| back 105 - process of keeping blood within a damaged blood vessel
• Steps:
o Vasoconstriction
o Temporary blockage of a break by a platelet plug
o Coagulation- the formation of a clot that seals the hole until tissues are repaired
• Active platelets bind together and cause other platelets to come as well which forms an initial clot
• Fibers join in to make a better clot and allow repair |
front 106 platelet rich plasma (PRP) therapy | back 106 o Helps the tissue that get relative little blood flow and thus have slow healing to get more platelets to them
o Collect blood from patient, concentrate sample
Raises platelet level to 2-6X normal levels
o Platelet granules contain:
Growth factors
Serotonin, histamine, dopamine, calcium
o PRP delivered as a clot
Must be a clot in order for it to stick |
front 107 4 main functions of the respiratory system | back 107 exchange of gases between the atmosphere and body
homeostatic regulation of pH
protection from inhaled pathogens and irritants
vocalization |
front 108 bulk flow (basic principles) | back 108 how the respiratory system carries out functions by exchanging air between the environment and the interior air spaces of the lungs
• Similar to cardiovascular system
• Flow moves from high pressure to lower pressure
• Muscular pump creates those pressure gradients
• Resistance is driven by tube size |
front 109 external respiration (steps) | back 109 the movement of gases between the external environment and the body’s cells
4 steps:
o Exchange gases between atmosphere and the lungs (ventilation)
o Exchange gases from the lungs to the blood
o Transport of the gases in the blood
o Exchange the gas to the target cells |
| back 110 conducting pathways that connect the lungs to the main airways, the trachea
the trachea branches into t2 primary bronchi. the primary bronchus divides 22 more times, terminating in a cluster of alveoli |
| back 111 Air enters through the mouth or nose, passes into the pharynx (throat), flows through the larynx into the trachea (windpipe) which divides into a pair of primary bronchi which divided repeatedly until the smallest bronchi become bronchioles |
| back 112 series of interconnected sacs and their associated pulmonary capillaries
o Form the exchange surface where O2 moves from inhaled air to the blood
CO2 moves from the blood to air that is about to exhaled
2 types of cells present
• Type I- performs gas exchange
• Type 2- not frequent
o Create surfactant which help type I with gas exchange and aid the lungs as they expand during breathing |
front 113 upper and lower respiratory tracts | back 113 Trachea is dividing line between upper and lower
• Upper respiratory tract- consists of the mouth, nasal cavity, pharynx, and larynx
Lower respiratory system- consists of the trachea, 2 primary bronchi, their branches, and the lungs |
| back 114 • Each lung sits in a pleural sac and a very thin pleural cavity that is filled with pleural fluid which allows the lungs to expand and contract smoothly
o Only 25-30ml of pleural fluid in an averaged size man
o Pleural fluid adds lubrication to the surface of the lungs and holds the lungs tight against the thoracic wall |
front 115 respiratory air conditioning | back 115 Warm air to body temperature
Add water vapor to inhaled air to reach 100% humidity
Filter out foreign material
• Cilia line the airways of the trachea and bronchi and are bathed in a Mucous layer plays a key role in keeping out foreign particles |
| back 116 o Pulmonary circulation
Low oxygen blood comes from right ventricle
Oxygenated blood returns to left atrium
Rate of blood flow to pulmonary system is same as the rest of the body
Normal blood pressure in the right ventricle is 25/8 |
| back 117 • PV=nRT
Boyle’s law
• V=1/P
• P1V1=P2V2
• Decreasing volume increases likelihood of collisions between gas molecules
Dalton’s Law
• Total pressure = sum of individual gas pressures |
front 118 lung volumes and capacities (image) | |
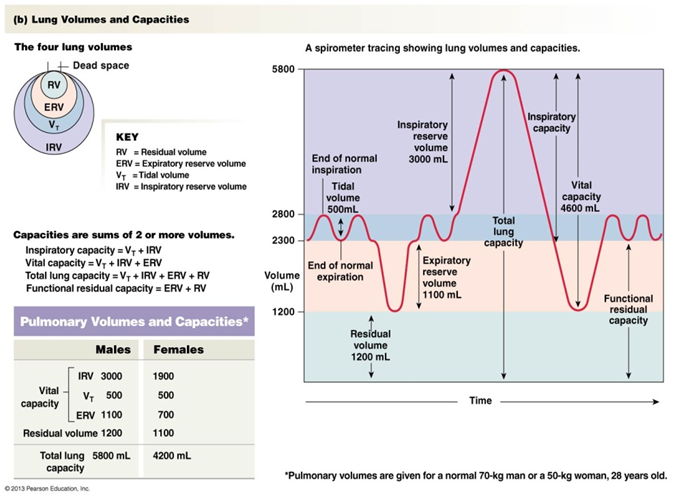
| back 119 o The air moved during breathing can be divided into 4 lung volumes, tidal volume, inspiratory reserve volume, expiratory reserve volume, and residual volume
Tidal volume- normal amounts of respiration
Inspiratory reserve volume- the additional volume you inspire above the tidal volume
Expiratory reserve volume- The amount of air forcefully exhaled after the end of a normal expiration
• Averages about 1100 mL
Respiratory reserve volume- The volume of air in the respiratory system after maximal exhalation |
| back 120 o Maximum amount of air you can breathe in or out
o Sums of lung volumes |
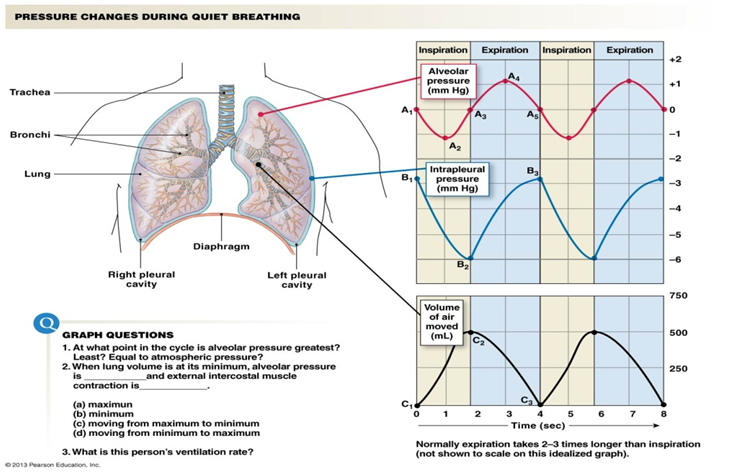
front 121 inspiration-alveolar pressure decreases | back 121 o Need lower pressure in alveoli than atmospheric pressure for air to move in
o Increase volume (diaphragm contracts and flattens) à decreased pressure
o Inspiration à increased thoracic volume |
front 122 pressure changes during quiet breathing | |
| back 123 Heavy breathing
Ventilation exceeds 30-40 breaths per minute
Activates abdominals & internal intercostals which are not used during inspiration |
| back 124 Ability of lungs to stretch
High compliance = easy to stretch
reciprocal factor of elastance |
| back 125 Ability to resist being deformed
High elastance = snaps back into place quickly/easily = low compliance
o Reciprocal factors (high Elastance= low compliance) |
front 126 emphysema and pulmonary fibrosis | back 126 o Emphysema- high compliance, low Elastance
Inhale easily struggle to exhale
o Pulmonary fibrosis- stiff, fibrous scar tissue that restricts lung inflation |
| back 127 o Less surface tension forces= easier to breathe
o Normally, surface tension arises via water molecules (from hydrogen bonds)
o Surfactants break up cohesive forces between water molecules
decreases the work necessary for breathing |
| back 128 increases the resistance to air flow and decreases the amount of fresh air that reaches the alveoli
• shut down bronchioles to avoid foreign particles and bacteria from entering, asthma |
front 129 total pulmonary ventilation | back 129 - estimation of the effectiveness of ventilation
The volume of air moved into and out of the lungs each minute
Total Pulmonary Ventilation= ventilation rate x tidal volume (VT)
• Total pulmonary ventilation= 12 breaths/min x 500 mL/breath= 6000 mL/min= 6 L.min
Amount of air you breath in is not the same as the amount of air that reaches the alveoli due to "dead space"
should always be larger than alveoli ventilation |
| back 130 conducting airways that do not exchange gases with the blood
• 150 mL gets trapped in your trachea and never make it to the alveoli (fresh air)
• 150 mL are sitting in your lungs at all times (stale air) |
| back 131 • Alveolar ventilation= ventilation rate x (VT- dead space volume VD)
• Alveolar ventilation= 12 breaths/min x x(500-150 mL/breath)= 4200 mL/min
should always be smaller than total pulmonary ventilation |
front 132 matching of blood flow and air flow | back 132 • Matching the ventilation rate into groups of alveoli with blood flow past those alveoli is a 2 part process involving local regulation of both air flow and blood flow
o Mostly depends on local factors such as concentrations of oxygen and CO2 in the lung tissue
• Normally perfusion of blood past alveoli is matched to alveolar ventilation to maximize gas exchange
• Local control mechanisms try to keep ventilation and perfusion matched |
| back 133 If pressure changes dictate it, the lungs can block off alveoli
• Regulated the diameters of the arterioles and bronchioles
• Little neural control |
| |
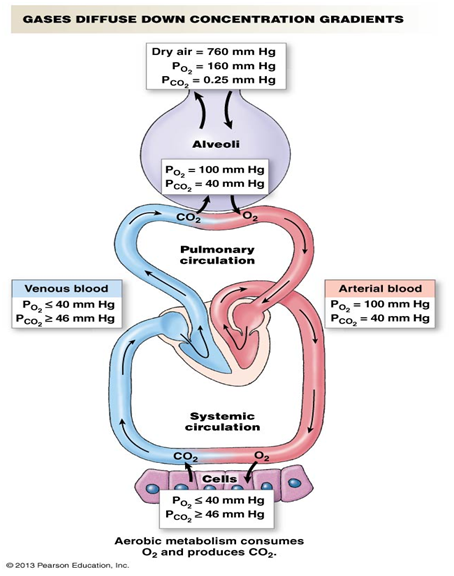
front 135 gas pressure gradients (values, image) | |
| back 136 Diffusion rate α surface area x concentration gradient x barrier permeability
Diffusion rate α 1/distance2
Under most circumstances, diffusion distance, surface area, and barrier permeability in the body are constants and are maximized to facilitate diffusion
• Concentration gradient between the alveoli and blood is the primary factor affecting gas exchange in healthy people |
| back 137 o Surface Area
Lower surface area -> reduced diffusion
o Permeability
Lower permeability -> reduced diffusion
o Distance
Increased distance -> reduced diffusion |
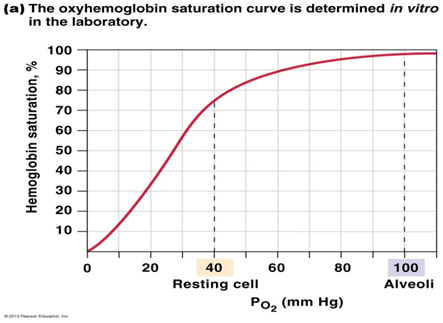
front 138 changes in concentrations of hemoglobin | back 138 • Increase cellular metabolism= decrease in hemoglobin percentage
o • Changes in pH
o Low pH= lower saturation (less O2) = decrease the affinity of hemoglobin for O2
• Temperature
o Higher temp= lower saturation= decrease the affinity of hemoglobin for O2
• Metabolic byproducts (PCO2)
o Increase byproduct concentration= lower saturation= decrease the affinity of hemoglobin for O2
Increase in the frequency of hemoglobin deposits |
| back 139 o Dissolve (7% gets dissolved)
o Use hemoglobin (23% uses hemoglobin)
o Change CO2 to bicarbonate (HCO3-)by combining CO2 with water
Makes a buffer
Used more frequently for transport |
front 140 somatic motor ventilation | back 140 Medulla controls ventilation muscles
Pons integrates sensory info & signals medulla
Central pattern generators create rhythmic breathing |
front 141 peripheral sensory receptors | back 141 located in the carotid and aortic arteries and sense changes in the PO2, pH, and PCO2 of the plasma
include glomus cells |
| back 142 - cells in the carotid and aortic bodies that are activated by a decrease in PO2 or pH or by an increase in PCO2
• Triggers increase in ventilation
• Similar to signal transduction in taste buds
• CO2 & H+ are primary indicators
peripheral sensory receptors |
| back 143 receptors in the brain that respond to changes in the concentration of CO2 in the cerebrospinal fluid
• Co2 can pass though the cerebral spinal fluid
o Drop in pH could also cause that change |