Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM Module 26: Assessing the Wound — Time to Practice
front 1 Importance: Lower extremity wounds are a significant clinical concern, particularly among patients with chronic health conditions such as diabetes, peripheral artery disease (PAD), and chronic venous insufficiency. Common wounds found on the lower extremities include: | back 1
|
front 2 Mixed venous and arterial ulcers | back 2 Features both poor oxygen delivery (arterial) and fluid congestion (venous), they often appear as deep, irregular wounds with moderate to heavy drainage, located on the lower leg or ankle |
front 3  Let's start with a warm-up to get you thinking about wound presentation. Can you tell which of these images is a DFU? * See next card for second picture | back 3  If you guessed the first image on front of this card, you are correct. *The image above is NOT a DFU, it's a trauma wound. |
front 4  What type of ulcer does John MOST likely have? Venous ulcer Arterial ulcer Mixed ulcer DFU | back 4 Venous ulcer * Based on John's symptoms, history, and the wound's characteristics, a venous ulcer is the most likely diagnosis. Venous ulcers are usually found on the lower legs, with symptoms like swelling and discomfort that worsen by day's end. Other options like arterial ulcers and diabetic foot ulcers (DFUs) typically present with different features, such as dry, punched-out wounds for arterial ulcers and ulcers on pressure points for DFUs. Mixed ulcers would show both arterial and venous characteristics. |
front 5 What is the first step when assessing John’s lower extremity ulcer? Checking for tunneling Cleaning the wound Assessing the need for debridement Applying topical antibiotics | back 5 Cleaning the wound * The first step is to clean the wound to clear contaminants and allow for an accurate assessment of the wound bed (The Royal Children’s Hospital [RCH], 2023). Tunneling, debridement, and topical antibiotics are important but should be considered after the wound is clean to ensure accurate assessment and subsequent treatments. |
front 6 What arterial perfusion assessment should be performed before applying compression for a venous insufficiency ulcer? Checking for the degree of pitting edema Culturing the wound to determine the presence of bacteria Palpating pedal pulses Ankle-brachial index test (ABI) | back 6 Ankle-brachial index test (ABI) * The ABI test is key to assessing arterial perfusion before compression therapy (Alagha et al., 2021). Given John's diabetes, alternative methods should be considered if ABI results are unreliable. Checking for pitting edema assesses venous outflow, not arterial perfusion. Wound cultures do not assess perfusion. Palpating pedal pulses can indicate arterial flow but is less comprehensive than the ABI test (Alagha et al., 2021). |
front 7 Before starting compression therapy, check the ___ to assess arterial perfusion and avoid further injury while allowing wound healing to proceed. In patients like John with diabetes, results may be unreliable due to arterial calcification. | back 7 ABI |
front 8 An ABI ___ suggests calcification—use alternative tests such as toe-brachial index (TBI). If ABI <0.5, blood flow is insufficient to support healing, and a vascular referral is needed before applying compression (Stanford Medicine, 25, n.d.). | back 8 >1.4 |
front 9 This symbol means? < | back 9 (Less Than): Indicates the value on the left is smaller than the value on the right (e.g., 3 < 5). |
front 10 This symbol means? > | back 10 > (Greater Than): Indicates the value on the left is larger than the value on the right (e.g., 10 > 7). |
front 11 If ABI ___, blood flow is insufficient to support healing, and a vascular referral is needed before applying compression (Stanford Medicine, 25, n.d | back 11 <0.5 |
front 12  Based on Mary's history and the examination findings, what type of wound does she MOST likely have? Pressure injury (PI) Venous leg ulcer (VLU) Mixed ulcer Diabetic Foot Ulcer (DFU) | back 12 Diabetic Foot Ulcer (DFU) |
front 13 Exammination: The wound on José's heel has a large necrotic area with black eschar and yellow slough. The wound bed appears moist, with significant slough covering a portion of the wound. The edges are irregular, and there are signs of surrounding erythema, which could indicate inflammation or early infection. You also notice that José has developed drop foot on the affected side. Based on your assessment, what type of wound does José have? | back 13 PI, including a large necrotic area with black and yellow tissue, a moist appearance, and significant slough (European Pressure Ulcer Advisory Panel [EPUAP], 2019). PIs often occur over bony prominences such as the heel, where sustained pressure impairs blood flow, leading to tissue necrosis. With the jagged edges and foot drop, there appears to be significant shearing associated with this PI. |
front 14 What factor must be assessed first to determine whether a wound is capable of healing? Presence of necrotic tissue Amount of exudate Blood supply to the area Patient's pain level | back 14 Blood supply to the area |
front 15 After verifying adequate perfusion to the wound, what step would stimulate healing? Applying a splint for his foot drop Initiating antibiotic therapy Performing a culture and sensitivity test Debridement of necrotic tissues | back 15 Debridement of necrotic tissues * Removing necrotic tissue via debridement stimulates healing by removing the wound from a chronic inflammatory state. It promotes a clean, healthy wound bed for cells to develop new tissue and allows for accurate staging (EPUAP et al., 2019). Applying a splint for foot drop is inappropriate as it can increase pressure and worsen the pressure injury. A culture and sensitivity test is indicated when infection is suspected and would direct you toward the appropriate antibiotic therapy. |
front 16 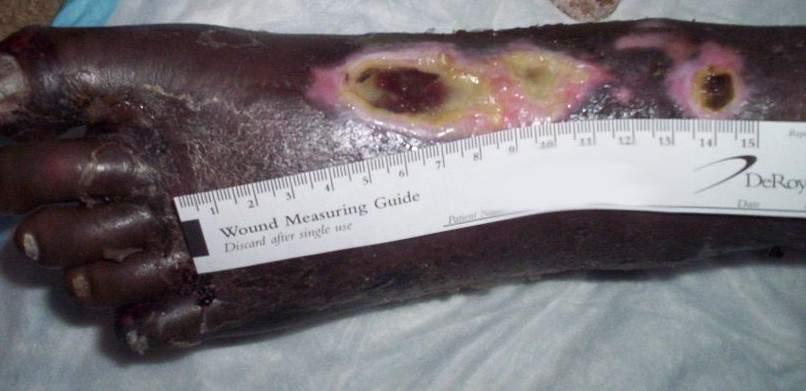 What type of ulcer does Mabel most likely have? Venous ulcer Arterial ulcer Mixed ulcer DFU | back 16 Arterial ulcer * Mabel’s symptoms and history, including Sickle Cell disease and severe PAD, strongly suggest an arterial ulcer. Sickle Cell disease can contribute to arterial insufficiency by causing vaso-occlusion, leading to ischemia and increased risk of tissue damage. Mabel’s symptoms do not indicate venous insufficiency, and she does not have diabetes, so a venous ulcer, mixed ulcer, or DFU is less likely. |
front 17 When performing an ABI to assess Mabel’s arterial perfusion, which of the following results should you be most concerned about? ABI 0.5 ABI of 0.8 ABI of 0.95 ABI of 1 | back 17 ABI 0.5 You should be MOST concerned about an ABI result of 0.5, as this indicates severe ischemia, which is a critical issue in managing Mabel’s arterial ulcer. An ABI of 0.5 suggests significant arterial insufficiency, where blood flow is severely compromised, increasing the risk of tissue necrosis and poor wound healing (Weller et al., 2019). While an ABI of 0.8 indicates arterial insufficiency, it reflects a less severe condition. ABIs between 0.9 and 1 are considered normal, reflecting adequate blood flow without significant arterial disease. |
front 18 Norma ABI values are | back 18 Ranges between 1.0 and 1.4 |
front 19  On examination, the underside of James's foot shows severe tissue damage, particularly around the toes and the ball of the foot. The affected areas have dark, necrotic tissue with black discoloration, indicating advanced tissue death. There are also areas of red and purple discoloration around the toes, with dry and scaly surrounding skin, showing signs of compromised blood flow and possible early gangrene. What is the most likely etiology of these areas on James’s foot? | back 19 This is most likely related to arterial insufficiency. The necrotic tissue on his toes, and the sole of his foot, along with cold feet, severe pain at rest, and a history of atherosclerosis, strongly support this diagnosis |
front 20  What type of ulcer do you MOST likely suspect? Venous ulcer Arterial ulcer Mixed ulcer DFU Robert’s wound is a mixed ulcer, which presents characteristics of both venous and arterial ulcers (WOCN, 2019). The presence of necrotic tissue and significant pain, especially at night, suggests arterial involvement. The swelling, edema, and extensive ulceration are indicative of venous insufficiency. Robert's medical history of both peripheral PAD and chronic venous insufficiency supports the diagnosis of a mixed ulcer. | back 20 Mixed ulcer * Robert’s wound is a mixed ulcer, which presents characteristics of both venous and arterial ulcers (WOCN, 2019). The presence of necrotic tissue and significant pain, especially at night, suggests arterial involvement. The swelling, edema, and extensive ulceration are indicative of venous insufficiency. Robert's medical history of both peripheral PAD and chronic venous insufficiency supports the diagnosis of a mixed ulcer |
front 21 On examination, the ulcer is extensive, covering a large portion of the dorsum of his foot and lower leg. The wound produces moderate serosanguineous exudate, and significant edema is present. Different types of tissue are present in the wound bed. How would you describe the types of tissue in the wound bed? Granulation tissue, slough, tendon, and necrotic tissue Granulation tissue, epithelial tissue, and healthy skin Slough, hypergranulation tissue, and infected tissue Necrotic tissue, epithelial tissue, and fibrous tissue | back 21 Granulation tissue, slough, tendon, and necrotic tissue * The wound bed in Robert’s ulcer shows areas of red, granulating tissue, exposed tendon, significant yellow slough, and black, dry necrotic tissue. Granulation tissue indicates healing, slough is devitalized tissue, and necrotic tissue represents dead tissue. The wound bed does not contain epithelial tissue (new skin), hypergranulation, or infected tissue. |
front 22  What type of wound would you suspect George to have? Venous ulcer Arterial ulcer PI DFU | back 22 DFU |
front 23 The provider feels around the periwound and the bottom of George’s feet. George does not appear to have much feeling or pain in the surrounding tissue. What does the lack of feeling MOST likely indicate? Reduced arterial perfusion Peripheral sensory neuropathy Venous insufficiency Severe edema | back 23 Peripheral sensory neuropathy |
front 24  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 24 Did you notice the Charcot deformity? That is your first clue that these wounds are related to diabetes. Additionally, they have well-defined, calloused edges, a dry wound bed, and pale, pink bases consistent with DFUs (WOCN, 2019). |
front 25  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 25 This wound has characteristics of a deep tissue PI, due to its location on the heel and bluish-purple fluid-filled blister, indicating blood (Baranoski & Ayello, 2020). The skin may be intact, but significant damage exists beneath the surface, often involving muscle and other deeper tissues. |
front 26  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 26 This is a venous ulcer due to the irregular wound edges, a moist wound bed, and surrounding skin changes such as thickening, darkening, edema, and erythema due to chronic venous insufficiency (WOCN, 2019). |
front 27  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 27 Pressure Injury * These wounds are characteristic of PIs, with one showing black necrotic tissue and the others with open areas of damage (EPUAP et al., 2019). |
front 28  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 28 This wound is characteristic of a (unstageable) PI--the location on the heel, necrotic tissue covering most of the wound, and macerated edges. Staging can occur after debridement of the necrotic tissue. |
front 29  Looking at the above image, what type of wound is this? Arterial DFU Venous Pressure Injury | back 29 The characteristics of this wound indicates venous stasis ulceration, with its location around the medial malleolus, irregular shape, superficial appearance, red granulation tissue and surrounding skin changes with thickening, darkening, and erythema |
front 30 Which of the following characteristics is MOST indicative of a venous ulcer? Necrotic tissue with dry wound edges Irregular wound edges with a moist wound bed Bluish-purple fluid-filled blister Well-defined ulcer on the plantar surface | back 30 Irregular wound edges with a moist wound bed |
front 31 Which assessment finding would be MOST concerning in a patient with a suspected diabetic foot ulcer (DFU)? Loss of sensation around the wound Presence of granulation tissue Moderate exudate Erythema around the wound | back 31 Loss of sensation around the wound |
front 32 What type of lower extremity wound is associated with cold feet and intense pain at rest that is relieved by dangling the leg off the edge of the bed? Venous ulcer Arterial ulcer Pressure injury Diabetic foot ulcer | back 32 Arterial ulcer |
front 33 What is the primary concern when an ABI test shows a result of 0.5 in a patient with an arterial ulcer? Severe ischemia Mild arterial disease Normal blood flow Venous insufficiency | back 33 Severe ischemia |
front 34 The patient states that they have decreased sensitivity around a wound on the top of their toe. What does this MOST likely indicate? Reduced arterial perfusion Peripheral sensory neuropathy Venous insufficiency Severe edema | back 34 Peripheral sensory neuropathy |
front 35 What is the primary purpose of performing an ankle-brachial index (ABI) test in patients with lower extremity wounds? To evaluate arterial blood flow To determine the level of infection To assess venous insufficiency To measure tissue perfusion | back 35 To evaluate arterial blood flow |
front 36 What is the significance of granulation tissue in a wound bed? It indicates the presence of infection. It requires immediate debridement. It represents dead tissue that must be removed. It signifies the formation of new tissue. | back 36 It signifies the formation of new tissue. |