Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM Module 22: Wound Care — Pediatric and Neonatal Considerations
front 1 Which factor is MOST likely to impair collagen formation and cell proliferation in children? Vitamin C deficiency Incorrectly unselected Zinc deficiency Correctly unselected Protein deficiency Incorrectly selected Poor circulation | back 1 Vitamin C deficiency * Vitamin C, along with vitamins B and D, is essential for collagen synthesis and cellular proliferation. A deficiency in vitamin C directly impairs collagen formation, which delays wound healing. |
front 2 Affects from zinc deficiency | back 2 Primarily affects epithelialization, which helps close and cover a wound. While this delays wound closure, it does not directly impact collagen formation |
front 3 Affects from protein deficiency | back 3 Hinders overall tissue repair and cell growth, reducing the body’s ability to rebuild tissue. Although protein is important for wound healing, it is not specifically involved in collagen synthesis. |
front 4 How does poor circulation affect wound healing? | back 4 By restricting oxygen and nutrient delivery, which are necessary for all stages of wound healing, but it does not specifically interfere with collagen formation. |
front 5 For neonates what dressings would you avoid? | back 5 Hydrogels if they are in incubator setting Alignate dressings d/t entering system and compromising bloodstream |
front 6 What does IAD stand for in wound mgt. | back 6 Incontinence-associated dermatitis, or diaper dermatitis, has the highest incidence between 7 and 12 months of age (Lund & Singh, 2022). |
front 7 IAD Treatment | back 7 Use a non-irritating, pH-balanced wipe/cleanser, or tepid tap water to clean the diaper area gently without causing further irritation (Lund & Singh, 2022). Then, apply a zinc oxide or petrolatum-based barrier cream to create a protective layer. Keeping the damaged skin moist is essential to promoting healing, so do not fully remove the protective cream already applied. Remove only the layers contaminated with stool, and then generously reapply the cream. |
front 8  Candida albicans, | back 8 a pathogenic yeast, presents as bright red areas of dermatitis with distinct boundaries and surrounding satellite lesions, typically involving the inguinal folds. Treatment for Candida infections requires an antifungal agent, such as nystatin or imidazoles (e.g., miconazole [Lotrimin®]). |
front 9 The recommended treatment protocol for Candida infection with skin denuding includes: | back 9 
|
front 10 (MARSI) | back 10 medical adhesive-related skin injury |
front 11 MARSI Treatment | back 11 To treat MARSI, gently clean the area with a pH-balanced cleanser and carefully dry it. Next, apply a silicone-based dressing (e.g., Mepitel®), as it protects the wound without adhering to it and causes minimal tissue damage during removal. |
front 12 MARSI Prevention The prevention of MARSI includes the preferred use of the following: | back 12
|
front 13 Acrylic-based dressings | back 13  Such as 3M™ Tegaderm™, may be required for a stronger adhesion for critical tubes and are an acceptable alternative to silicone-based products. |
front 14 Hydrocolloid Dressings | back 14  Such as DuoDERM®, act as both an adhesive and barrier, allowing for better adherence to curved surfaces and moisture resistance. |
front 15 Precautions Avoid the following: | back 15
|
front 16 Intravenous Extravasation | back 16  occurs when vesicant fluids leak into the surrounding soft tissue from a cannula or vein, leading to blistering, sloughing, and necrosis. Premature infants are at higher risk for more severe skin damage due to the immature skin, less subcutaneous tissue, and small size of their blood vessels (Bryant & Nix, 2024). |
front 17 Common first signs of extravasation include | back 17 Swelling, redness or discoloration, pain, blanching, firmness, and coolness. |
front 18 Extravasation Treatment The initial steps for managing IV extravasation are as follows (Lippincott Williams & Wilkins, 2022; Tarpey, 2023): | back 18
|
front 19 Antidotes can be administered either through the catheter or directly into the extravasation site with a small-gauge needle (e.g., tuberculin syringe). The choice of antidote and the application of cool/warm compresses is complex and dependent on the properties of the extravasated drug, with antidotes including (Tarpey et al., 2023): | back 19
|
front 20 After antidote administration and venous access removal: | back 20
|
front 21 Extravasation Wound Treatment To treat extravasation wounds: | back 21 
|
front 22 Extravasation Prevention The following strategies help prevent intravenous extravasation (Lund & Singh, 2022): | back 22
|
front 23 In neonates and children, the _____ is the most common area for development of PIs (Caillouette & Quigley, 2020). Other high-risk areas include the ear and nose, with older children and adolescents having PI patterns more similar to those of adults (e.g., sacrum and heels). | back 23 occiput |
front 24 Staging for PIs in neonates and children follows the National Pressure Injury Advisory Panel (NPIAP). | back 24 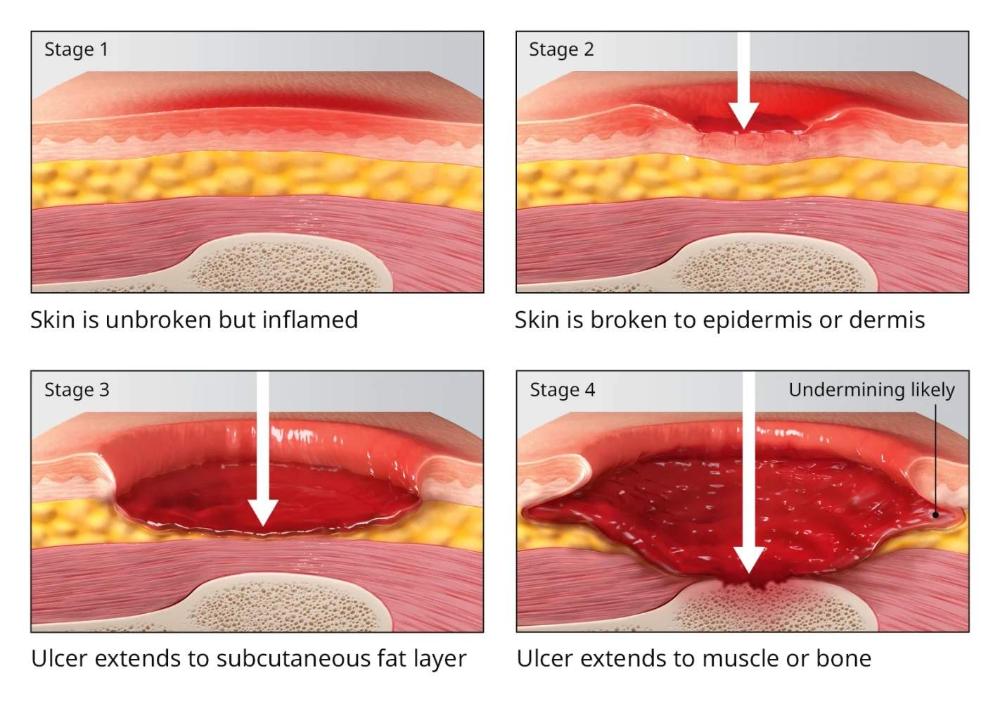 See image for all 4 stages |
front 25 PI Treatment The selection of products used for PI treatment in neonates and children must take into consideration the following: | back 25
|
front 26 PI Treatment Commonly used commercial products include (Caillouette & Quigley, 2020): | back 26 
|
front 27 The ___ ____ is the preferred PI risk assessment tool for pediatric patients (Caillouette & Quigley, 2020). | back 27 Braden QD Scale |
front 28 The Braden QD Scale assesses: | back 28
|
front 29 Best practices in the prevention of PI in neonates and children include: | back 29
|
front 30 What is the FIRST step to take when IV extravasation is suspected?. Elevate and immobilize the extremity Disconnect the IV tubing Stop infusing all medications and fluids Remove the IV catheter | back 30 Stop infusing all medications and fluids *To prevent further tissue damage. You should NOT remove the IV catheter as it is needed for attempting aspiration of the vesicant and administering an antidote. Disconnecting the IV tubing is important, but it follows the cessation of infusion. Elevating and immobilizing the extremity is a later step aimed at reducing swelling. |
front 31 Which intervention is recommended to prevent incontinence-associated dermatitis (IAD) in neonates? Applying antiseptic creams Daily application of talcum powder Cleaning with isopropyl alcohol Frequent diaper changes | back 31 Frequent diaper changes *reduce skin moisture exposure, helping prevent incontinence-associated dermatitis. Talcum powder is not recommended for use in neonates. Topical antiseptics can delay wound healing. Isopropyl alcohol should be avoided on neonatal skin due to its potential for toxicity and irritation |
front 32 Which dressing type is preferred for treating medical adhesive-related skin injuries (MARSI) in neonates? Acrylic-based dressings Silicone-based dressings Silver-impregnated dressings Medical grade honey | back 32 Silicone-based dressings * The treatment of MARSI includes applying a silicone-based dressing to protect the area such as Mepitel. Acrylic-based dressings are used to secure critical tubes. Silver-impregnated and medical grade honey dressings are used in neonatal and pediatric wound care but are not preferred for MARSI. |
front 33 Why is protein intake crucial for pediatric wound healing? Enhances fluid balance Aids in collagen synthesis Increases vascularity Promotes tissue repair | back 33 Promotes tissue repair *Protein primarily supports tissue repair and cell growth for wound healing. |
front 34 Why should products containing alcohol be avoided when treating neonatal wounds? Increases wound drainage Causes pH imbalance Potential toxicity Promotes epidermal thickening | back 34 Potential toxicity * Alcohol-containing products are potentially toxic to neonates, as their skin permeability allows higher absorption rates than in adults. |
front 35 Which treatment protocol is recommended for managing incontinence-associated dermatitis (IAD) complicated by Candida infection? Antifungal powder, skin protectant, zinc oxide cream Antifungal powder, zinc oxide cream, skin protectant Zinc oxide cream, antifungal powder, skin protectant Zinc oxide cream, skin protectant, antifungal powder | back 35 Antifungal powder, skin protectant, zinc oxide cream The treatment protocol recommended for managing incontinence-associated dermatitis (IAD) complicated by Candida infection is antifungal powder, skin protectant, and zinc oxide cream. |