Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
SWM MODULE 13: Assessing the Wound - Pressure Injuries
front 1 What does DTPI stand for in woundcare? | back 1 Deeper Tissue Injuries |
front 2 What does PI stand for in woundcare | back 2 Pressure Injury |
front 3 Which mechanical force could potentially cause tunneling and undermining in a PI? | back 3 Shear Force * it acts in combination w/or independently of pressure and friction to damage deep tissue planes and separate skin from underlying structures. |
front 4 ___ ___ can cause tunneling and undermining in a PI due to stretching and tearing of blood vessels, reducing blood flow, and deforming tissue. Friction mostly affects the outermost layer of the skin and does not typically cause tunneling or undermining. Pressure leads to tissue compression and ischemia but does not directly cause tunneling and undermining. Tensile forces are related to the stretching of tissues but do not typically cause tunneling or undermining in PIs. | back 4 Shearing forces |
front 5 What type of patient do you think would be MOST at risk for developing a PI? A 55-year-old with a knee injury who can reposition themselves in bed A 68-year-old with a hip fracture who is confused and incontinent of urine A 75-year-old with a minor skin abrasion and broken ankle who uses a walker A 45-year-old with a mild fever and nausea who is eating little | back 5 A 68-year-old with a hip fracture who is confused and incontinent of urine |
front 6 Slough: | back 6 Thick, stringy yellow or white tissue, indicating the presence of dead tissue |
front 7 Eschar: | back 7 Black or brown necrotic tissue that is hard or leathery |
front 8 Epithelial tissue: | back 8 New skin growing over a wound bed |
front 9 Deeper structures: | back 9 In severe cases, the wound bed may expose deeper structures like bones, ligaments, or tendons. |
front 10 Tunneling: | back 10 Narrow channels extending from the wound into deeper tissue layers. |
front 11 Undermining: | back 11 Areas where the tissue under the wound edges erodes, creating a pocket. |
front 12 Abscess: | back 12 Localized collections of pus indicating infection. |
front 13 Bone Palpation: | back 13 Exposed bone indicates a more advanced stage. |
front 14 Fistulas: | back 14 Abnormal connections between the wound and other body parts or organs. |
front 15 Non-blanchable erythema: | back 15 Redness that does not turn white when pressed, indicating a Stage 1 PI. |
front 16 Redness that does not turn white when pressed, indicating a Stage __ PI. | back 16 1 PI |
front 17 Periwound Area Deepening of natural color: | back 17 Particularly noticeable in patients w/darker skin tones, this can indicate underlying damage. |
front 18 Periwound Area Signs of pressure and shear damage: | back 18 Look for evidence of undermining or tunneling. |
front 19 Documentation Describing the wound | back 19 Detailed notes on the wound's - size, depth, appearance, and changes over time |
front 20 Documentation Photographic records | back 20 Using photographs to visualy document the wound's condition and progression. |
front 21 Documentation Regular Reassessment | back 21 Regular reassessment to adjust care plans based on the wound's healing trajectory and any new developments. |
front 22  What stage is this PI | back 22 The appearance of a full thickness wound with some yellow tissue, granulation, epibole and maceration indicates it is a Stage 3 PI. It’s too deep to be a Stage 2 PI, there are no deeper structures exposed to make it a Stage 4 PI, and since we can see the wound base, it is stageable. |
front 23  What stage is this pressure injury? | back 23 The appearance of a partial thickness wound with pink tissue indicates a Stage 2 PI. If there were full tissue loss it would be a Stage 3 PI. There is a break in the skin, so it is not a Stage 1, and no deeper structures are exposed to make it a Stage 4 PI. |
front 24 You are caring for a patient with a PI who previously had full-thickness tissue damage involving subcutaneous tissue. The PI is showing signs of healing. What stage PI would this be considered? | back 24 Even though the PI shows signs of healing, it remains classified as a Stage 3 PI. The original severity of the injury is maintained in documentation to reflect the initial extent of tissue damage. Stage 1 PIs involve intact skin with non-blanchable erythema. Stage 2 PIs involve partial-thickness skin loss. Stage 4 PIs involve full-thickness skin loss extending through the subcutaneous tissue with exposed underlying structures, such as muscle or bone. |
front 25 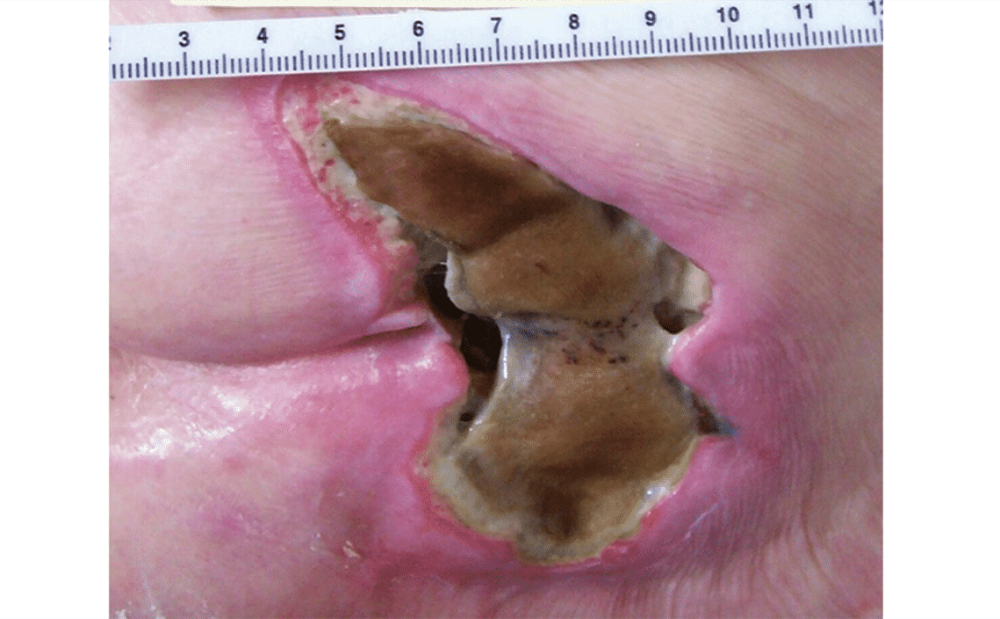 What stage is the PI? | back 25 Unstageable pressure injuries involve full-thickness tissue loss with the wound base obscured by slough or eschar, making it impossible to determine the true depth until these are removed (NPIAP, 2023). |
front 26 SORE® The SORE® mnemonic may be used to identify devices contributing to device-related PIs (Baranoski & Ayello, 2020). It stands for: | back 26 Stock Items Objects Required medical devices Electronic Equipment |
front 27 What does KTU stand for? | back 27 Kennedy Terminal Ulcer * Unique ulcers that occur at the end of live. * Typically form within a single day. |
front 28 KTU Characteristeics include: | back 28
|
front 29 KTU are a result of | back 29
|
front 30 ____ are considered an unavioidable Pi. There is no way to determine the risk of developing a _______ | back 30 KTU / KTU |
front 31 Once an ____ pressure injury is debrided and the wound bed is visible, the correct stage should be assigned based on the depth and severity of the tissue damage. This process accurately reflects the current condition of the wound and is not considered reverse staging. A Stage 1 DTPI is not appropriate nomenclature, leaving it classified as unstageable does not apply once the base of the wound is visible, and staging is never reversed or downgraded. | back 31 unstageable |
front 32  What stage is this injury? | back 32 Unstageable * The base of the wound is obscured by eschar, making it unstageable. There would be a visible wound base if it were a 2, 3, or 4 PI. |
front 33  Identify this lesion Mucosal Membrane Device-Related PI Device-Related PI Stage 3 PI Unstageable PI | back 33 Device-Related PI * The shape of the injury mirrors the shape of the g-tube’s fixation ring, making this a Device-Related PI. It is not on a mucosal membrane, and the other options are incorrect due to depth and visible wound bed. |
front 34 ____ involve full-thickness tissue loss obscured by slough or eschar, preventing accurate staging until debridement reveals the wound depth, at which point appropriate staging can be assigned. | back 34 Unstageable PIs |
front 35 __ __ __ are caused by sustained pressure from medical devices and often mirror the shape of the device. Regular skin checks and preventive measures, such as proper fitting and adjustment of devices, are essential to prevent these injuries. | back 35 Device-related pressure injuries |
front 36 ___ are rapidly developing ulcers that occur at the end of life, distinct from typical pressure injuries. They should be managed with a focus on patient comfort rather than aggressive treatment. | back 36 KTUs |
front 37 Braden Moisture Subscale Scores: 4 or 3 | back 37 Rarely or occasionally moist |
front 38 Braden Moisture Subscale Scores: 2 | back 38 Very Moist |
front 39 Braden Moisture Subscale Scores: 1 | back 39 Constantly Moist |
front 40 Braden Mobility Subscale Scores: 4 or 3 | back 40 No limitation or slightly limited
|
front 41 Braden Mobility Subscale Scores: 2 or 1 | back 41 Very limited or completely immobile *Reactive /CLP *Active w/AP feature |
front 42 Braden Mobility Subscale Scores: 2 | back 42
|
front 43 Braden Mobility Subscale Scores: 1 | back 43
|
front 44 Suggested support surface overlay or mattress selections for pressure injury prev. & treatment on Braden Mobility & Moisture Subscores | back 44 Note: Persons with multiple Stage 2, or large (of sufficient size to compromise a turning surface) or multiple Stage 3 or Stage 4 pressure injuries on the trunk or pelvis involving more than one available turning surface should be placed on a support surface with a low air loss or an air fluidized feature. |
front 45 Suggested Support Surface overlay or Mattress selections for PI prevention & treatment based on Braden Mobility & Moisture Subscores TABLE A In this table, the ________ refers to all types of Support Surfaces in this category with the exception of AMG sheep skin overlays, which are noted separately. | back 45 Reactive/CLP |