Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Fluorescein Staining - Diagnostic Patterns
front 1 Fluorescein staining terms: | back 1 Epithelial staining after instillation of fluorescein is observed under cobalt blue light as a bright green fluorescence, which can be described as - punctate = spot-like - diffuse = spots merging together - coalescent = large regions of confluence |
front 2 Staining pattern descriptions: | back 2 The staining pattern may be described according to the following groups of type descriptors: - arcuate = arc-like pattern - linear - dimpled Locations: superior, inferior, temporal, nasal or central; and deep or superficial. |
front 3 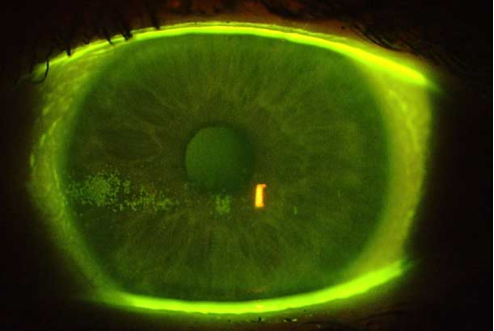 | back 3 Superficial Punctate Keratitis (SPK) Fluorescein staining shows isolated or diffuse dots across a larger area of the cornea. A diffuse pattern may indicate solution toxicity or an interaction between certain lens/solution combinations or dry eye syndrome. A contact lens that is too tight, has protein deposits or is over worn can cause peripheral SPK. |
front 4 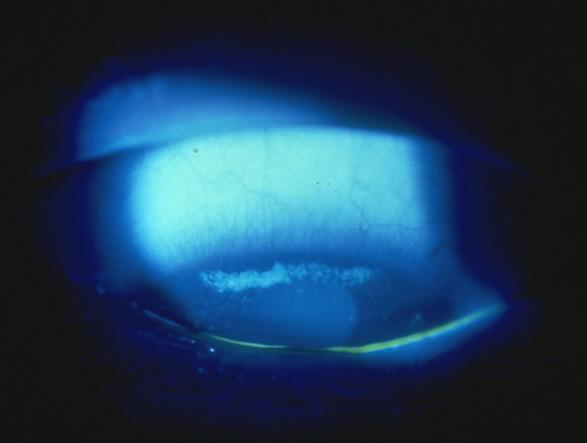 | back 4 Superior epithelial arcuate lesion (SEAL) Fluorescein stain present parallel to the superior limbus. Often due to mechanical chaffing by a contact lens (poor insertion or recentering techniques) on the superior cornea. The patient is usually asymptomatic. SEAL management: cease CL wear; change to a lower modulus material e.g. hydrogels, or consider RGPs. |
front 5 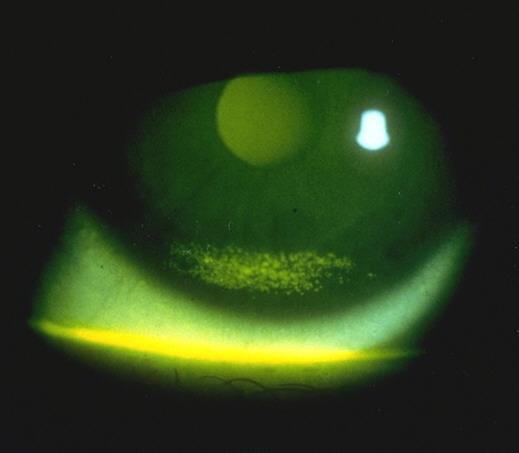 | back 5 Inferior arcuate staining (SMILE stain) Fluorescein staining is parallel to the inferior limbus, typically in the lower third of the cornea, and is often due to dehydrated contact lenses associated with insufficient post-lens tear film. Patients may have complaints of mild discomfort. |
front 6 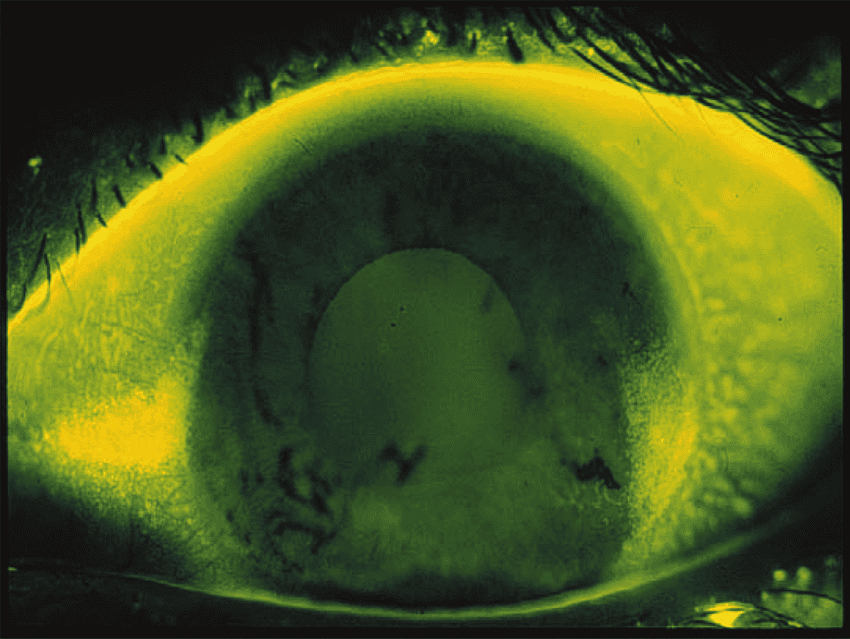 | back 6 Three and nine o'clock staining Fluorescein staining is parallel to the nasal and temporal limbus. This staining is associated with rigid contact lens wear and is due to inadequate spreading of the tear film over these areas as a result of incomplete and/or infrequent blinking (dry eye). Patients may experience mild discomfort. |
front 7 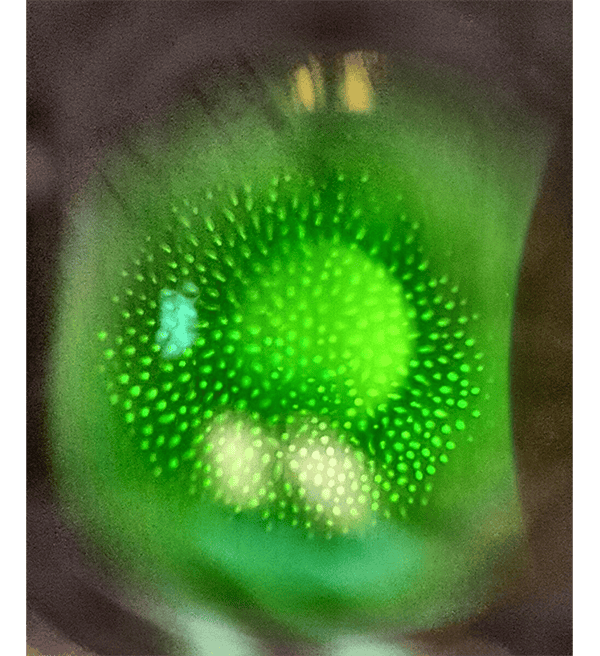 | back 7 Dimple veil staining not true staining, but rather pooling of the dye into corneal indention caused by trapped air bubbles under a poorly fitting rigid gas permeable contact lens. It presents as sharply demarcated, circular patterns of stain on the cornea. |
front 8 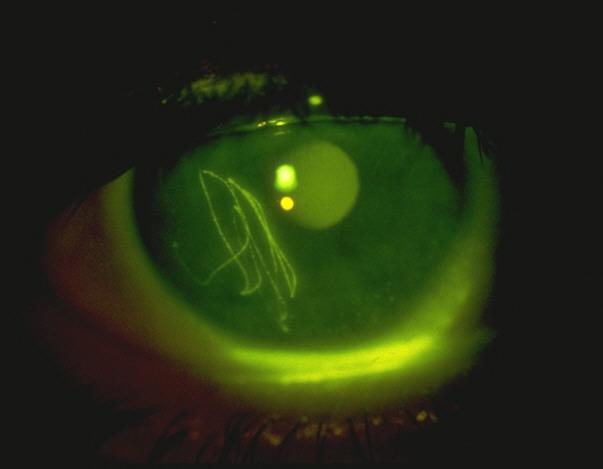 | back 8 Foreign body staining (corneal abrasions or scratches) Corneal abrasions staining can present in various ways, such as a zigzag-shaped abrasion or as the outline shape of an embedded foreign body. Scratches to the front window of the eye (cornea) are a very painful experience as there are many nerves in this area. The eye often becomes very watery, red and sensitive to light. If the scratch has happened in the middle of the cornea then vision can become blurred. |
front 9 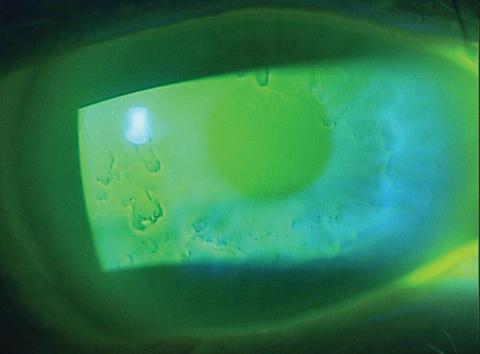 | back 9 Epithelial Basement Membrane Dystrophy (EBMD) Fluorescein staining with cobalt blue light shows mapping or fingerprint patterns or raised dots. EBMD patients have elevated regions on the corneal surface that appear darker or black when compared with the surrounding cornea because they are not adequately covered by the tear film. Most people with EBMD do not have symptoms and may not be aware they have EBMD. Those who do have symptoms may have mild to severe blurry vision and pain, sensitivity to light, excessive tearing, and a feeling that something is in the eye. The main cause of symptoms is recurring development of erosions in the cornea. |
front 10  | back 10 Herpetic Keratitis Fluorescein staining reveals dendritic lesions (linear branching patterns with terminal bulbs) or geographic ulcers associated with the herpes simplex virus (HSV). The edges may be slightly elevated due to swollen epithelial cells. Symptoms include eye pain, corneal injection, visual changes (blurry vision, decreased visual acuity), tearing, discharge, photophobia. |
front 11 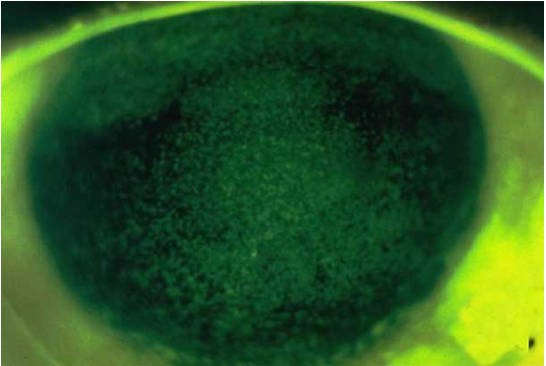 | back 11 Solution-Induced Corneal Staining or Solution Toxicity (diffuse pattern shown) Fluorescein staining will show localized disruption of the corneal epithelial surface (SPK) in either a diffuse or annular pattern. Symptoms include stinging or burning on lens insertion or removal. Effects are generally related to concentration and dosage of chemical preservative(s). Toxic effects of solution components potentially include hydrogen peroxide (inadequate neutralization), thimerosal, benzalkonium chloride, chlorhexidine |
front 12 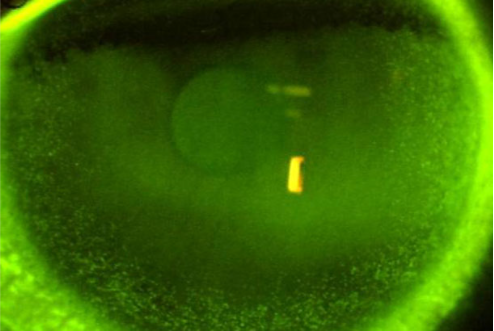 | back 12 Solution-Induced Corneal Staining or Solution Toxicity (annular pattern shown) Fluorescein staining will show localized disruption of the corneal epithelial surface (SPK) in either a diffuse or annular pattern. Symptoms include stinging or burning on lens insertion or removal. Effects are generally related to concentration and dosage of chemical preservative(s). Toxic effects of solution components potentially include hydrogen peroxide (inadequate neutralization), thimerosal, benzalkonium chloride, chlorhexidine |
front 13 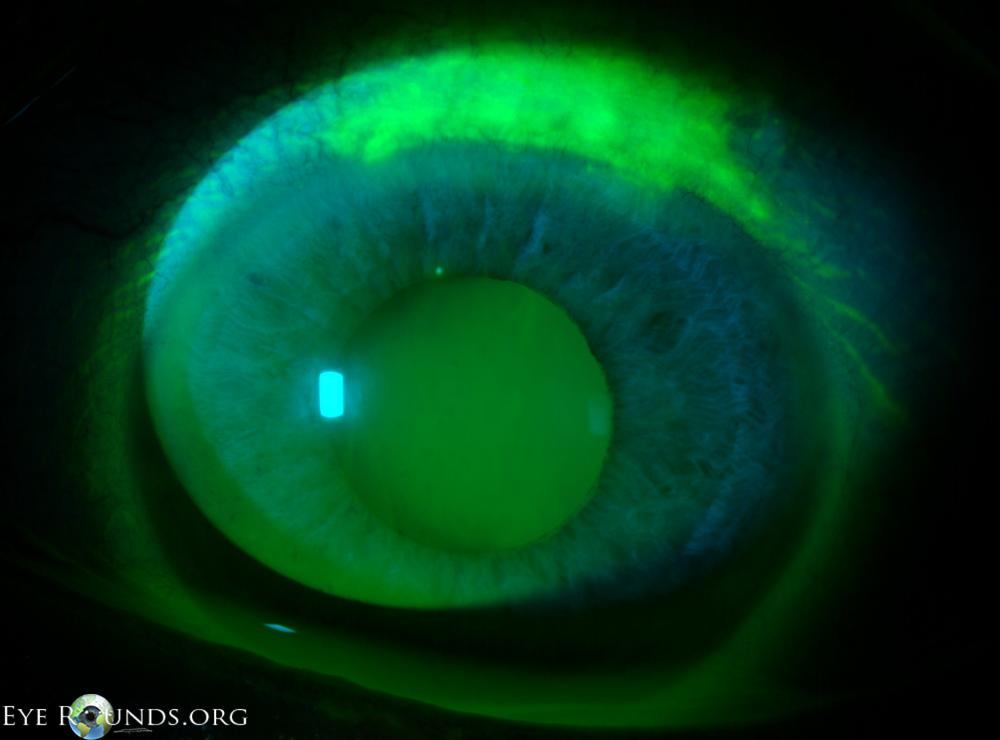 | back 13 Superior Limbic Keratoconjunctivitis Fluorescein shows fine punctate staining of the superior cornea, limbus, and conjunctiva. Superior Limbic Keratoconjunctivitis is disease characterized by
inflammation of the upper palpebral and superior bulbar conjunctiva,
keratinization of the |
front 14 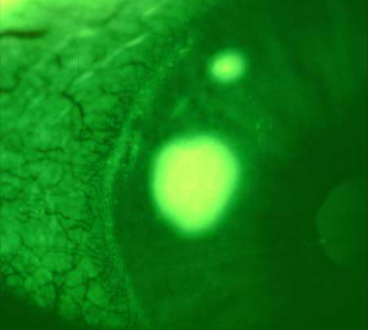 | back 14 Confluent Staining Corneal fluorescein staining over a substantial area; configurations vary. Indicates moderate to severe disruption of the epithelium. May result from abrasions, foreign body under the lens, major toxic response or severe metabolic insult. May also result from a bound rigid lens (after overnight wear). Symptoms include discomfort, which may persist for some time following lens removal. |
front 15  | back 15 Corneal Erosion Patch or area of coalesced sodium fluorescein staining, generally irregular shape. May be asymptomatic. Deeper erosions will result in discomfort, pain, photophobia, and/or foreign body sensation. |
front 16 Diagnose: Fluorescein staining with the aid of a blue cobalt filter shows isolated or diffuse dots across a larger area of the cornea. | back 16 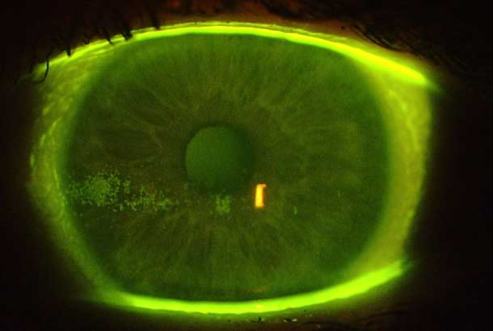 Superficial Punctate Keratitis (SPK) Fluorescein staining shows isolated or diffuse dots across a larger area of the cornea. A diffuse pattern may indicate solution toxicity or an interaction between certain lens/solution combinations or dry eye syndrome. A contact lens that is too tight, has protein deposits or is over worn can cause peripheral SPK. |
front 17 Diagnose: Fluorescein stain present parallel to the superior limbus on the superior cornea. | back 17 Superior epithelial arcuate lesion (SEAL) Fluorescein stain present parallel to the superior limbus. Often due to mechanical chaffing by a contact lens (poor insertion or recentering techniques) on the superior cornea. The patient is usually asymptomatic. SEAL management: cease CL wear; change to a lower modulus material e.g. hydrogels, or consider RGPs. . |
front 18 Diagnose: Patient complains of mild discomfort and dry contact lenses. Fluorescein staining appears in the lower third of the cornea and is parallel to the inferior limbus. | back 18 Inferior arcuate staining (SMILE stain) Fluorescein staining is parallel to the inferior limbus, typically in the lower third of the cornea, and is often due to dehydrated contact lenses associated with insufficient post-lens tear film or poorly blended secondary curves. Patients may have complaints of mild discomfort. |
front 19 Diagnose: Patient with rigid contact lenses complains of mild discomfort. Fluorescein shows staining on both sides of the limbus on the horizontal meridian. | back 19 Three and nine o'clock staining Fluorescein staining is parallel to the nasal and temporal limbus. This staining is associated with rigid contact lens wear and is due to inadequate spreading of the tear film over these areas as a result of incomplete and/or infrequent blinking (dry eye). Patients may experience mild discomfort. Solution: Reduce center and edge thickness and teach patient to blink completely |
front 20 Diagnose: Fluorescein staining shows sharply defined, circular patterns of stain on the cornea. | back 20 Dimple veil staining not true staining, but rather pooling of the dye into corneal indention caused by trapped air bubbles under a poorly fitting rigid gas permeable contact lens. It presents as sharply demarcated, circular patterns of stain on the cornea. |
front 21 Diagnose: Patient complains of a sudden onset of pain in their eye and is now sensitive to light. The eye is also red and watery. Fluorescein staining shows a zigzag-shaped abrasion. | back 21 Foreign body staining (corneal abrasions or scratches) Corneal abrasions staining can present in various ways, such as a zigzag-shaped abrasion or as the outline shape of an embedded foreign body. Scratches to the front window of the eye (cornea) are a very painful experience as there are many nerves in this area. The eye often becomes very watery, red and sensitive to light. If the scratch has happened in the middle of the cornea then vision can become blurred. |
front 22 Diagnose: Patient complains of mild blurry vision and watery eyes. Fluorescein staining with cobalt blue light shows mapping patterns. | back 22 Epithelial Basement Membrane Dystrophy (EBMD) Fluorescein staining with cobalt blue light shows mapping or fingerprint patterns or raised dots. EBMD patients have elevated regions on the corneal surface that appear darker or black when compared with the surrounding cornea because they are not adequately covered by the tear film. Most people with EBMD do not have symptoms and may not be aware they have EBMD. Those who do have symptoms may have mild to severe blurry vision and pain, sensitivity to light, excessive tearing, and a feeling that something is in the eye. The main cause of symptoms is recurring development of erosions in the cornea. |
front 23 Diagnosis: Fluorescein staining reveals linear branching patterns with terminal bulbs. | back 23 Herpetic Keratitis Fluorescein staining reveals dendritic lesions (linear branching patterns with terminal bulbs) or geographic ulcers associated with the herpes simplex virus (HSV). The edges may be slightly elevated due to swollen epithelial cells. Symptoms include eye pain, corneal injection, visual changes (blurry vision, decreased visual acuity), tearing, discharge, photophobia. |
front 24 Diagnose: Patient complains of a stinging/burning sensation during contact lens insertion. Fluorescein staining shows localized disruption of the corneal epithelial surface in a diffused pattern. | back 24 Solution-Induced Corneal Staining or Solution Toxicity (diffuse pattern shown) Fluorescein staining will show localized disruption of the corneal epithelial surface (SPK) in either a diffuse or annular pattern. Symptoms include stinging or burning on lens insertion or removal. Effects are generally related to concentration and dosage of chemical preservative(s). Toxic effects of solution components potentially include hydrogen peroxide (inadequate neutralization), thimerosal, benzalkonium chloride, chlorhexidine |
front 25 Diagnose: Patient complains of a stinging/burning sensation during contact lens insertion. Fluorescein staining shows localized disruption of the corneal epithelial surface in an annular pattern. | back 25 Solution-Induced Corneal Staining or Solution Toxicity (annular pattern shown) Fluorescein staining will show localized disruption of the corneal epithelial surface (SPK) in either a diffuse or annular pattern. Symptoms include stinging or burning on lens insertion or removal. Effects are generally related to concentration and dosage of chemical preservative(s). Toxic effects of solution components potentially include hydrogen peroxide (inadequate neutralization), thimerosal, benzalkonium chloride, chlorhexidine |
front 26 Diagnose: Fluorescein shows fine punctate staining of the superior cornea, limbus, and conjunctiva. | back 26 Superior Limbic Keratoconjunctivitis Fluorescein shows fine punctate staining of the superior cornea, limbus, and conjunctiva. Superior Limbic Keratoconjunctivitis is disease characterized by
inflammation of the upper palpebral and superior bulbar conjunctiva,
keratinization of the |
front 27 Diagnose: Patient complains of discomfort after contact lens removal. Fluorescein shows staining over a substantial area of the corneal. | back 27 Confluent Staining Corneal fluorescein staining over a substantial area; configurations vary. Indicates moderate to severe disruption of the epithelium. May result from abrasions, foreign body under the lens, major toxic response or severe metabolic insult. May also result from a bound rigid lens (after overnight wear) Symptoms include discomfort, which may persist for some time following lens removal. |
front 28 Diagnose: Patch or area of coalesced sodium fluorescein staining, generally irregular shape. | back 28 Corneal Erosion Patch or area of coalesced sodium fluorescein staining, generally irregular shape. May be asymptomatic. Deeper erosions will result in discomfort, pain, photophobia, and/or foreign body sensation. |