Instructions for Side by Side Printing
- Print the notecards
- Fold each page in half along the solid vertical line
- Cut out the notecards by cutting along each horizontal dotted line
- Optional: Glue, tape or staple the ends of each notecard together
Chapter 9: Allergies and Immunologic Diseases
front 1 Clinical Features
Histopathologic Features
| back 1 transient lingual papillitis |
front 2  Tender, yellow-pink papule on the dorsum of the tongue. | back 2 transient lingual papillitis, localized |
front 3 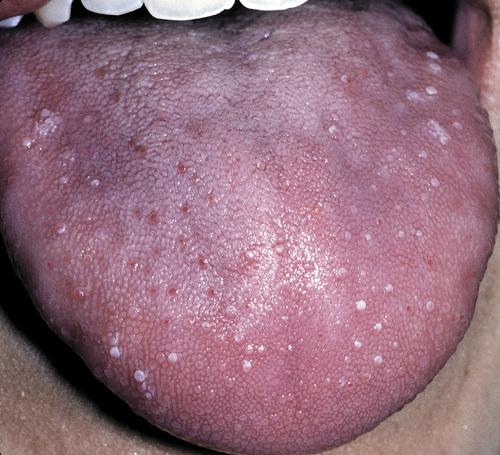 Multiple painful white papules on the lateral dorsum and tip of tongue. | back 3 transient lingual papillitis, generalized |
front 4  Clusters of asymptomatic, elevated, yellow papules on the dorsolateral surface of the tongue. | back 4 transient lingual papillitis, papulokeratotic |
front 5 What is the treatment and prognosis for transient lingual papillitis? | back 5
|
front 6 Clinical Features
Histopathological Features
| back 6 recurrent aphthous stomatitis |
front 7 Clinical Features
| back 7 minor aphthous ulceration |
front 8 Clinical Features
| back 8 major aphthous ulceration |
front 9 Clinical Features
| back 9 herpetiform aphthous ulceration |
front 10  Erythematous halo encircling a yellowish ulceration of the soft palate on the left side. | back 10 minor aphthous ulceration |
front 11  Two ulcerations of different sizes located on the maxillary labial mucosa. | back 11 minor aphthous ulceration |
front 12  Single ulceration of the anterior buccal mucosa. | back 12 minor aphthous ulceration |
front 13  Large, deep, and irregular ulceration of the posterior buccal mucosa. Note extensive scarring of the anterior buccal mucosa from previous ulcerations. | back 13 major aphthous ulceration |
front 14  Large, irregular ulceration of the soft palate. | back 14 major aphthous ulceration |
front 15  Numerous pinhead ulcerations of the ventral surface of the tongue, several of which have coalesced into larger, more irregular areas of ulceration. | back 15 herpetiform aphthous ulceration |
front 16 Aphthous ulcerations that heal within 1 to 2 weeks and recur infrequently. | back 16 simple aphthosis |
front 17 Aphthous ulcerations that occur in multiples and develop continuously. | back 17 complex aphthosis |
front 18 How is recurrent aphthous stomatitis diagnosed? | back 18 No laboratory procedure provides definitive diagnosis; the diagnosis is made from the clinical presentation and from exclusion of other diseases. |
front 19 What is the treatment and prognosis for recurrent aphthous stomatitis? | back 19
|
front 20 
| back 20 major aphthous ulceration |
front 21 Clinical Features
Histopathological Features
| back 21 Behçet syndrome |
front 22  Diffuse erythema surrounding numerous irregular ulcerations of the soft palate. Oral ulcerations often herald the onset of this disease. | back 22 Behçet syndrome |
front 23  Numerous irregular ulcerations of the labia majora and perineum as part of a disease characterized by chronic ocular inflammation and orogenital ulcerations. | back 23 Behçet syndrome |
front 24  Sterile pustule of the skin that developed 1 day after injection of saline. This reaction is termed cutaneous pathergy. | back 24 Behçet syndrome |
front 25 From a diagnostic standpoint, one of the most important skin manifestations in Behçet syndrome is the presence of positive “pathergy.” What does this refer to? | back 25 One or 2 days after the oblique insertion of a needle under sterile conditions, a tuberculin-like skin reaction or sterile pustule develops. |
front 26 No laboratory finding is diagnostic of Behçet syndrome. What In an attempt to standardize diagnoses, five definitive criteria have been developed. What are they? | back 26
|
front 27 What is the treatment and prognosis for Behçet syndrome? | back 27
|
front 28 Clinical Features
Histopathological Features
| back 28 sarcoidosis |
front 29  Violaceous indurated plaques of the right malar area and bridge of nose. | back 29 lupus pernio (sarcoidosis) |
front 30  Multiple erythematous macules of the hard palate. Oral lesions are uncommon in this disease, but may be normal in color, brown-red, violaceous, or hyperkeratotic. | back 30 sarcoidosis |
front 31  Erythematous macules with central hyperkeratosis of the lower labial mucosa. Oral lesions are uncommon in this disease. | back 31 sarcoidosis |
front 32 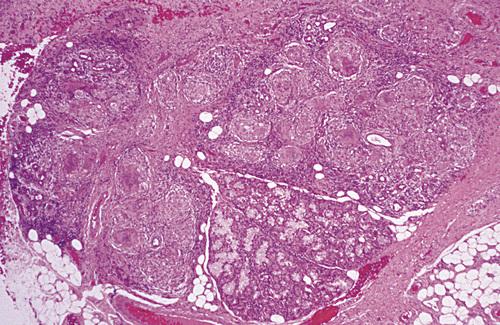 Labial minor salivary gland demonstrating granulomatous inflammation characterized by circumscribed collections of histiocytes, lymphocytes, and multinucleated giant cells. | back 32 sarcoidosis |
front 33 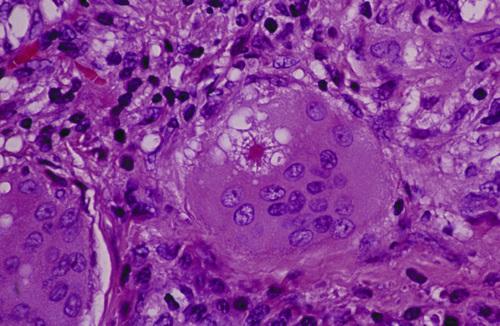 Multinucleated giant cell with intracytoplasmic asteroid body, a stellate inclusion consisting of entrapped fragments of collagen. | back 33 sarcoidosis |
front 34 A clinical syndrome associated with acute sarcoidosis consisting of erythema nodosum, bilateral hilar lymphadenopathy, and arthralgia. | back 34 Löfgren syndrome |
front 35 A clinical syndrome associated with acute sarcoidosis consisting of parotid enlargement, anterior uveitis of the eye, facial paralysis, and fever. | back 35 Heerfordt syndrome (uveoparotid fever) |
front 36 How is sarcoidosis diagnosed? | back 36
|
front 37 What is the treatment and prognosis for sarcoidosis? | back 37
|
front 38 Clinical Features
Histopathological Features
| back 38 orofacial granulomatosis |
front 39 The variant of orofacial granulomatosis in which there is nontender, persistent swelling of the lips combined with facial paralysis and a fissured tongue. | back 39 Melkersson-Rosenthal syndrome |
front 40 The variant of orofacial granulomatosis in which there is nontender, persistent swelling of the lips in isolation. | back 40 cheilitis granulomatosa (of Miescher) |
front 41  Nontender, persistent enlargement of the upper lip. This patient did not present with facial paralysis nor a fissured tongue. | back 41 cheilitis granulomatosa (orofacial granulomatosis) |
front 42  Persistent enlargement of the lower lip. This patient also presented with numerous furrows on the dorsal surface of the tongue. | back 42 Melkersson-Rosenthal syndrome (orofacial granulomatosis) |
front 43  Note numerous furrows on the dorsal surface of the tongue. This patient also presented with persistent enlargement of the lower lip. | back 43 Melkersson-Rosenthal syndrome (orofacial granulomatosis) |
front 44  Hyperplastic mucosa noted bilaterally in the mandibular mucobuccal fold with elongated ulcerations in the base of these folds. | back 44 orofacial granulomatosis |
front 45 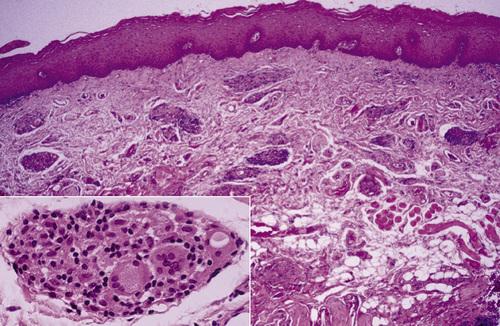 Clusters of granulomatous inflammation around scattered vessels. The inset illustrates the histiocytes and multinucleated giant cells within the granulomas. | back 45 orofacial granulomatosis |
front 46 How is orofacial granulomatosis diagnosed? | back 46 Based on histopathologic demonstration of granulomatous inflammation that is associated with negative special stains for organisms and no foreign material. |
front 47 What is the treatment and prognosis for orofacial granulomatosis? | back 47
|
front 48 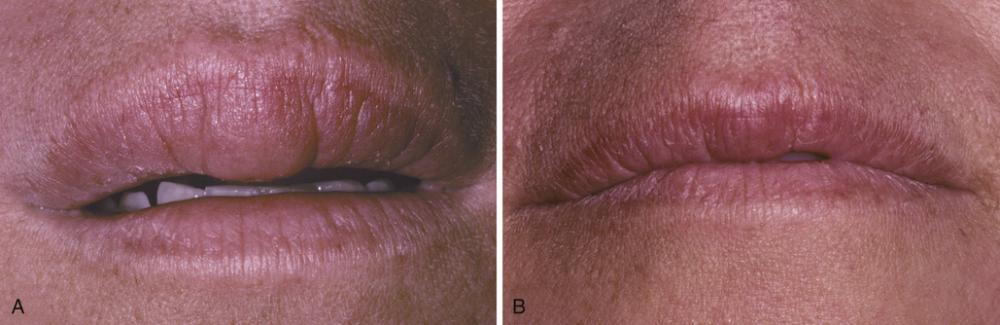
| back 48 orofacial granulomatosis |
front 49 
| back 49 orofacial granulomatosis |
front 50 Clinical Features
Histopathological Features
| back 50 Wegener granulomatosis |
front 51  Florid and granular gingival hyperplasia with hemorrhagic and friable bulbous projections ("strawberry gingivitis"). | back 51 Wegener granulomatosis |
front 52  Hyperplastic and hemorrhagic mucosa of the facial mandibular gingiva on the left side. This red, bumpy surface is responsible for the strawberry-like appearance | back 52 Wegener granulomatosis |
front 53  Deep, irregular ulceration of the hard palate on the left side. These represent late-stage disease; more than 60% of patients will have renal involvement. | back 53 Wegener granulomatosis |
front 54 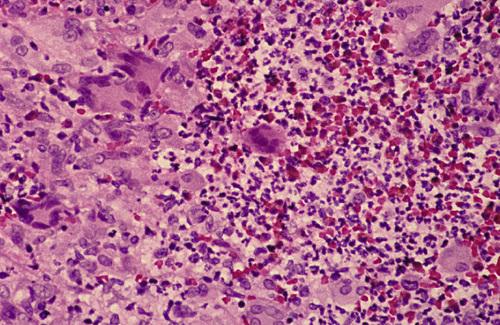 Connective tissue containing proliferation of numerous vascular channels and a heavy inflammatory infiltrate consisting of lymphocytes, neutrophils, eosinophils, and multinucleated giant cells. | back 54 Wegener granulomatosis |
front 55 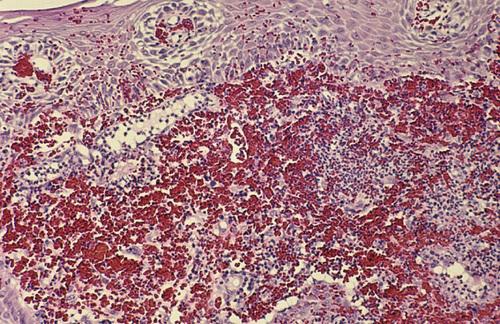 Gingival biopsy specimen showing a mixed inflammatory cellular infiltrate obscured by extensive extravasation of red blood cells. | back 55 Wegener granulomatosis |
front 56 The American College of Rheumatology proposed four diagnostic criteria with a minimum of two required for a diagnosis of Wegener granulomatosis. What are these criteria? | back 56
|
front 57 What marker is the most useful in the diagnosis of Wegener granulomatosis, seen in 90% to 95% of generalized cases and 60% of the early or localized cases? | back 57 antibodies against proteinase-3 (PR3-ANCA) |
front 58 What is the treatment and prognosis for Wegener granulomatosis? | back 58
|
front 59 The risk of an adverse reaction is approximately ___% with the use of two medications, ___% with five drugs, and almost ___% with eight or more. | back 59 6%, 50%, 100% |
front 60 What is a Type A drug reaction? | back 60 An exaggerated but otherwise expected pharmacologic action of the prescribed medication (e.g. bleeding associated with warfarin). |
front 61 What is a Type B drug reaction? | back 61 An idiosyncratic reaction that is not expected, usually arising from immune-mediated effects (e.g. hypersensitivity reactions). |
front 62 A reaction of the oral mucosa to the systemic administration of a medication. | back 62 stomatitis medicamentosa |
front 63 Several different patterns of stomatitis medicamentosa exist. What are the seven classes of mucosal reactions to systemic drug administration? | back 63
|
front 64 Clinical Features
Histopathological Features
| back 64 mucosal reactions to systemic drug administration |
front 65 
| back 65 allergic mucosal reaction to systemic drug administration |
front 66  Irregular area of superficial erosion of the left buccal mucosa. Lesions were also present on the contralateral buccal mucosa and bilaterally on the lateral borders of the tongue. Lesions disappeared after discontinuing allopurinol. | back 66 lichenoid drug reaction |
front 67  Large irregular erosion of the right ventral surface of the tongue. The lesion arose secondary to use of oxaprozin, a nonsteroidal antiinflammatory drug (NSAID). | back 67 allergic mucosal reaction to systemic drug administration |
front 68 How are mucosal reactions to systemic drug administration diagnosed? | back 68
|
front 69 What is the treatment for mucosal reactions to systemic drug administration? | back 69
|
front 70 Clinical Features
| back 70 allergic contact stomatitis |
front 71  Mucosal erythema and vesicles of the lower labial mucosa caused by use of aluminum chloride on gingival retraction cord. | back 71 allergic contact stomatitis |
front 72  Erythematous mucosa with superficial epithelial desquamation. This patient reported recently changing brands of toothepaste. | back 72 allergic contact stomatitis |
front 73 How is allergic contact stomatitis diagnosed? | back 73
|
front 74 What is the treatment and prognosis for allergic contact stomatitis? | back 74
|
front 75 Clinical Features
Histopathologic Findings
| back 75 perioral dermatitis |
front 76  Multiple erythematous papules of the skin surrounding the vermilion border of the lips. Note similar involvement around the nasal orifices. | back 76 perioral dermatitis |
front 77 What is the treatment for perioral dermatitis? | back 77
|
front 78 Clinical Features
Histopathologic Findings
| back 78 contact stomatitis from cinnamon flavoring |
front 79 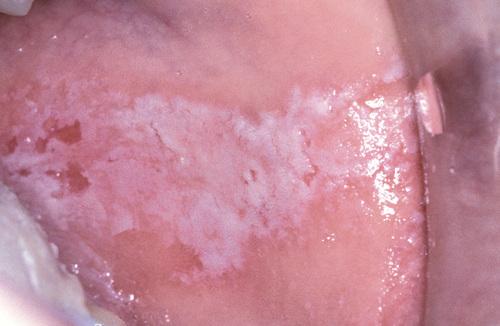 Oblong area of sensitive erythema with overlying shaggy hyperkeratosis. Buccal mucosal lesions often are aligned along the occlusal plane. | back 79 contact stomatitis from cinnamon flavoring |
front 80  Sensitive and thickened hyperkeratosis of the lateral and dorsal surface of the tongue on the right side. | back 80 contact stomatitis from cinnamon flavoring |
front 81  Left lateral border of the tongue demonstrating linear rows of hyperkeratosis that resemble oral hairy leukoplakia (OHL). | back 81 contact stomatitis from cinnamon flavoring |
front 82 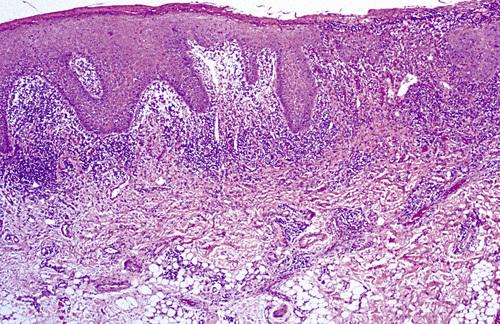 Oral mucosa demonstrating significant interface mucositis and deeper perivascular inflammation. Heavy inflammatory cell infiltrate often obscures the epithelium and connective tissue interface. | back 82 contact stomatitis from cinnamon flavoring |
front 83 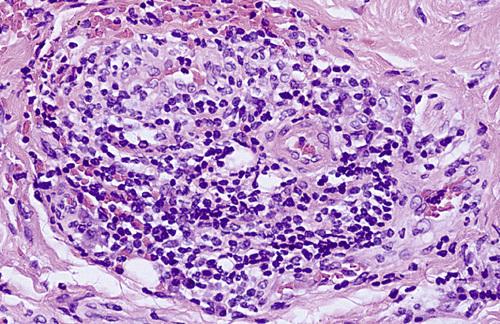 Perivascular inflammatory infiltrate consisting predominantly of lymphocytes and plasma cells, a characteristic feature in localized cases. | back 83 contact stomatitis from cinnamon flavoring |
front 84 How is contact stomatitis from cinnamon flavoring diagnosed? | back 84 Based on the clinical appearance and the history of cinnamon use; often biopsies are performed for atypical or extensive cases. |
front 85 What is the treatment and prognosis for contact stomatitis from cinnamon flavoring? | back 85
|
front 86 The vast majority of hypersensitivity reactions to dental restorative materials are to dental amalgam. What component is largely responsible? | back 86 mercury |
front 87 Although rare acute reactions to mercury may be seen following placement of amalgam, the vast majority of adverse alterations are associated with older and corroded amalgams. What type of hypersensitivity reactions are these? | back 87 type IV hypersensitivity reaction |
front 88 Clinical Features
Histopathologic Findings
| back 88 lichenoid contact reaction to dental restorative material |
front 89 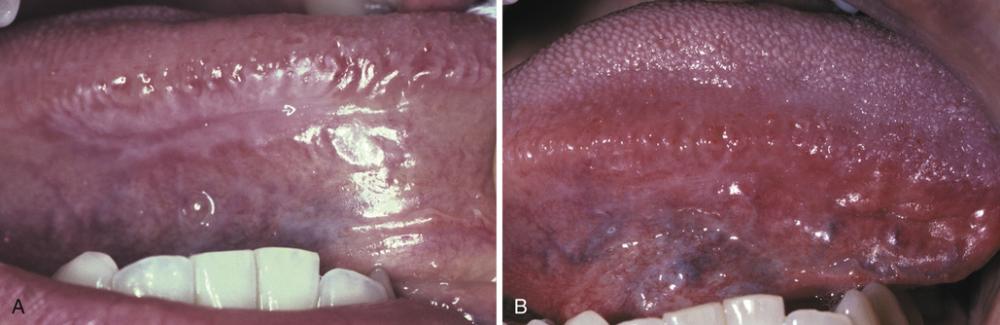
| back 89 lichenoid contact reaction to dental amalgam |
front 90  Radiating pattern of hyperkeratotic striae on the posterior buccal mucosa that contacts a large distobuccal amalgam of the permanent mandibular second molar. | back 90 lichenoid contact reaction to dental amalgam |
front 91 How is lichenoid contact reaction to dental amalgam diagnosed? | back 91 Based on (a) the clinical appearance of the lesion, (b) the lack of lesional migration, and (c) the correlation to adjacent dental metal. |
front 92 What is the treatment and prognosis for lichenoid contact reaction to dental amalgam? | back 92
|
front 93 A diffuse edematous swelling of the soft tissues, which has also been referred to historically as Quincke disease. | back 93 angioedema |
front 94 Angioedema is a diffuse edematous swelling of the soft tissues. What are the potential causes of angioedema? | back 94
|
front 95 An unusual pattern of drug reaction that can produce severe forms of angioedema that are not mediated by IgE is the type associated with ACE inhibitors. What is thought to be the cause of this reaction? | back 95 excess bradykinin (ACE degrades bradykinin) |
front 96 Clinical Features
| back 96 angioedema |
front 97 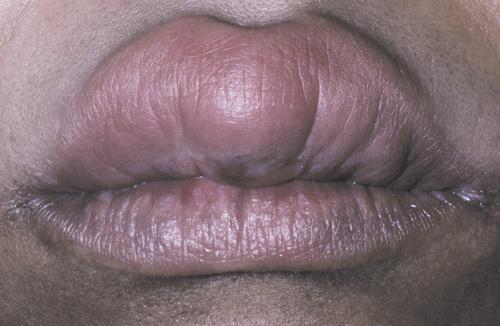 Diffuse upper lip swelling that arose rapidly. | back 97 angioedema |
front 98 
| back 98 angioedema |
front 99 How is angioedema diagnosed? | back 99
|
front 100 What is the treatment and prognosis for angioedema? | back 100
|