The thoracic cage consists of what four structures?
- The Sternum
- 12 Pairs of ribs
- 12 Thoracic vertebrae
- The Diaphragm, which forms the floor.
Which ribs are attached to the sternum via their costal cartilages?
Ribs 1-7.
Which ribs are attached to the costal cartilage above?
Ribs 8-10
Which ribs are "free floaters"?
The 11th and 12th ribs. And they have palpable tips.
On the anterior thorax, what surface landmarks do you look for?
- The suprasternal notch.
- The sternum (or breastbone).
- The sternal angle (or angle of Louis).
- The costal angle.
Where is the Suprasternal Notch and how can you identify it?
It feels like a hollow U-shaped depression just above the sternum, between the clavicles.
Where is the Sternum and how can you identify it?
- It's made of three parts:
- The manubrium
- The body
- The xiphoid process.
- Walk your fingers down the manubrium a few centimeters (cm) until you feel a distance bony ridge = the sternal angle.
Where is the Sternal Angle, what else is it called, and how can you identify it?
- Angle of Louis (AoL)
-
It's articulation of the manubrium and body of the sternum,
and is continuous with the 2nd rib.
- It's useful place to start counting ribs, localizing the respiratory finding horizontally.
- Once AoL is identified, palpate lightly to the second rib and slide down to the 2nd intercostal space (ICS).
What does the Angle of Louis mark for the respiratory system and the cardiac system?
- It marks the site of tracheal bifurcation into the right and left main bronchi.
- It corresponds with the upper border of
the atria of the heart.
- It lies above the 4th Thoracic vertebra on the back.
Where is the Costal Angle and why is it important?
- It's where the right and left costal margins meet at the xiphoid process, usually forming a 90 degrees angle, or less.
- This angle increases when the rib cage is
chronically overinflated.
- Ex. Emphysema (a condition in which the air sacs of the lungs are damaged and enlarged, causing breathlessness; or a condition in which air is abnormally present within the body tissues).
What are the four surface landmarks on the posterior thorax?
- The V ertebra Prominens.
- The Spinous Processes.
- The Inferior Border of the
Scapula
- Usually the lower tip is at the seventh or eighth rib.
- The 12th rib.
What are the references lines on the anterior chest?
- The Midsternal line.
- The Midclavicular line.
Describe the position of the midclavicular line.
This line bisects the center of each clavicle at a point halfway between the palpated sternoclavicular and acromioclavicular joints.
What are the references lines on the posterior chest?
- The Vertebral (midspinal) line.
- The Scapular line.
Describe the position of the scapular line.
This line extents through the inferior angle of the scapula when the arms are at the side of the body.
Lift up the person's arm at 90 degrees, and the lateral chest can be divided in three reference lines. What are they?
- The Anterior Axillary line.
- The Posterior Axillary line.
- The Midaxillary line.
Describe the anterior axillary line.
This line extends down from the anterior axillary fold where the pectoralis major muscle inserts.
Describe the posterior axillary line.
This line continues down from the posterior axillary fold where the latissimus dorsi muscle inserts.
Describe the mid axillary line.
This line runs down from the apex of the axilla and lies between and parallel to the other two.
The mediastinum is the middle section of the thoracic cavity and contains, what?
Contains the:
- Esophagus
- Trachea
- Heart
- Great vessels.
What do the right and left pleural cavities on either side of the mediastinum contain?
Contains the:
- Lungs
Anteriorly, where does the apex (highest point) of the lungs lie?
They lie 3 or 4 centimeters above the inner third of the clavicles
Where does the base (lower border) of the lungs rest?
They rest on the diaphragm at about the fifth intercostal space in the right midclavicular line and at the 6th rib in the left midclavicular line.
Laterally, the lungs extend from the apex of the axilla to what?
Extends to the 7th or 8th rib.
Posteriorly, C7 marks the 1. and T10 usually corresponds to the 2. On deep inspiration, the base descends to 3.
- Apex
- Base
- T12
The right lung is shorter than the left lung, and has how many lobes?
It has three lobes.
The left lung is narrower than the right lung, and has how many lobes?
It has two lobes.
Why is the right lung shorter than the left lung?
Because the liver lies underneath it.
Why left lung narrower than the right lung?
Because the heart bulges to the left.
On the anterior chest, where does the oblique (major or diagonal) fissure lie and terminate?
This fissure crosses the 5th rib in the midaxillary line and terminates at the 6th rib in the midclavicular line.
Anteriorly, the right lung also contains the horizontal (minor) fissure, which divides the right upper and middle lobes. Describe where it lies.
This fissure extends from the 5th rib in the right midaxillary line to the third intercostal space (ICS), or the 4th rib at the right sternal border.
Posteriorly, what is the most remarkable thing about the lungs?
It's almost all lower lobe of the lungs on both sides.
Posteriorly, the upper lobes' apices lies where?
They begin at T1 and reach down to T3 or T4.
At what level do the lower lobes begin posteriorly and where do they end?
They begin at T3 or T4 and reach down to level of T10 (or T12).
When would the posterior lungs reach T10? And T12?
- During Expiration.
- During Inspiration.
Laterally, the lungs extend from where to where?
The lung tissue extends from the apex of the axilla down to the 7th or 8th rib.
Laterally, the right upper lobe extends from where to where?
It extends from the apex of the axilla down to the horizontal fissure at the 5th rib.
Laterally, the right middle lobe extends from where to where?
It extends from the horizontal fissure down and forward to the 6th rib at the midclavicular line.
Laterally, the right lower lobe extends from where to where?
It continues from the 5th rib to the 8th rib in the midaxillary line.
Laterally, the left upper lobe extends from where to where?
It extends from the apex of the axilla down to the 5th rib at the midaxillary line.
Laterally, the left lower lobe extends from where to where?
It continues down to the 8th rib in the midaxillary line.
The anterior chest contains mostly...?
Upper and middle lobe with very little lower lobe.
The posterior chest contains...?
Almost all lower lobe.
What are the four major functions of the respiratory system?
- Supplying O2 to the body for energy production.
- Removing CO2 as a waste product of energy reactions (rxns).
- Maintaining homeostasis (acid-base balance) of arterial blood.
- Maintaining heat exchange (less important in humans).
Hypoventilation (slow, shallow breathing) causes what to build up in the blood?
Carbon dioxide (CO2)
Hyperventilation (rapid, deep breathing) causes what to be blown off?
Carbon dioxide (CO2)
What mediates the involuntary control mechanism of respiration?
The Pons and Medulla in the brainstem.
What is the normal stimulus that causes us to breathe?
Hypercapnia: an increase of CO2 in the blood.
What also causes an increase of respiration, but is less effective than hypercapnia?
Hypoxemia: a decrease of O2 in the blood.
In inspiration, increasing the size of the thoracic container creates 1. what kind of pressure in relation to the atmosphere and 2. what occurs because of it?
- Slightly negative pressure.
- Causes air to rush in to fill the partial vacuum.
What major muscle(s) is responsible for the lengthening of the vertical diameter?
Diaphragm
What major muscle(s) is responsible for the lengthening of the horizontal diameter?
Intercostal muscles lift the sternum and elevates the ribs.
Together, the diaphragm and the intercostal muscles increase what?
The anteroposterior (A-P) diameter of the thoracic cavity.
Expiration is primarily passive. As the diaphragm relaxes, elastic forces within the lung, chest cage, and abdomen cause it to dome up. All this squeezing creates what kind of pressure and what occurs?
Relatively positive pressure within the alveoli, and air flows out.
To obtain subjective data, what kind of questions should be asked?
- About Cough.
- Shortness of breath.
- Chest pain with breathing.
- History of respiratory infections.
- Smoking history ("pack year": packs per year).
- Environmental exposure, especially on the job.
-
Self-care behaviors
- Such as pneumonia or influenza immunizations.
When can shortness of breath (SOB) be related to heart failure?
- If the patient has orthopnea, "two pillow orthopnea," and/or paroxysmal nocturnal dyspnea.
Define Orthopnea.
Difficulty breathing while supine (laying down).
Define the meaning of "Two pillow orthopnea."
Needs 2+ pillows supporting them in order to be comfortable.
Define Paroxysmal Nocturnal Dyspnea.
Awakening from sleep with SOB (caused by an unknown source) and needs to be upright to achieve comfort.
Some conditions of cough have characteristic sputum production. What could white or clear mucoid indicate?
- Colds
- Bronchitis
- Viral infections
Some conditions of cough have characteristic sputum production. What could yellow or green mucoid indicate?
- Bacterial infections
Some conditions of cough have characteristic sputum production. What could rust-colored mucoid indicate?
- Tuberculosis
- Pneumococcal pneumonia
Some conditions of cough have characteristic sputum production. What could pink, frothy mucoid indicate?
- Pulmonary edema
- Some sympathomimetic medications' side effect (pink-tinged mucus).
Some conditions have a characteristic cough. What could a hacking cough indicate?
- Mycoplasma pneumonia
Some conditions have a characteristic cough. What could a dry cough indicate?
- Early heart failure
Some conditions have a characteristic cough. What could a barking cough indicate?
- Croup (aka Laryngotracheobronchiti)
- A
respiratory condition that is usually triggered by an acute
viral infection of the upper airway.
- The infection leads to swelling inside the throat, which interferes with normal breathing and produces the classical symptoms of a "barking" cough, stridor, and hoarseness.
- A
respiratory condition that is usually triggered by an acute
viral infection of the upper airway.
Some conditions have a characteristic cough. What could a congested cough indicate?
- Cold
- Bronchitis
- Pneumonia
To obtain objective data, inspect the posterior and anterior chest.
- Note the shape, configuration, and symmetry of the thoracic cage, including...
- Assess the quality of the...
- Also observe the skin color and condition and the patient’s...
- Anteroposterior ratio, placement of the scapulae, angle of the ribs, and development of the neck and trapezius muscles.
- Respirations.
- Position for breathing, facial expression, and level of consciousness.
The anteroposterior (AP) ratio should be...1. than the transverse (TV) diameter. The ratio of AP to TV diameter is from...2.
- Less than
- 1:2 to 5:7
Describe the characteristics of Barrel Chest.
- AP = TV diameter.
- Costal angle > 90 degrees.
- Ribs are horizontal instead of the normal downward slope.
- Chest appears as if held in continuous inspiration.
- This occurs in chronic emphysema and asthma from hyperinflation of the lungs; and normal aging (see Table 18-3, p. 440).
Define symptoms of Chronic Obstructive Pulmonary Disease (COPD).
- Skinny legs.
- Barrel chest.
- Clubbed nails.
- Tense, strained tired facies.
- Pursed lips in whistling position.
The neck muscles and trapezius muscles should be normally developed for age and occupation. What is an abnormal finding?
Neck muscles are hypertrophied in COPD from aiding in forced respiration.
Note the position the person takes to breathe.
- What is a normal finding?
- Abnormal findings for people with COPD?
- Posture is relaxed and they have the ability to support their own weight with arms comfortably at the sides or in the lap.
- Sit in a tripod position, leaning forward with arms braced against their knees, chair, or bed.
Why do people with COPD assume a tripod position to breathe?
This gives them leverage so that their rectus abdominis, intercostal, and accessory neck muscles can all aid in expiration.
Why is it extremely important to monitor a person with COPD closely when they receive O2?
They can stop breathing when they get enough O2. This occurs because we normally breathe to get rid of CO2; but they breathe to get O2. Once they have enough O2, they stop breathing.
Palpate the thorax and lungs, assessing the entire chest wall, posterior and anterior. What are the three main things that need to be checked?
- Confirm symmetric chest expansion.
- Assess tactile (or vocal) fremitus.
- Check for any lumps, masses, or tenderness.
Define (Tactile/Vocal) Fremitus.
A palpale vibration because sounds generated from the larynx are transmitted through patent bronchi and through the lung parenchyma to the chest wall, where the vibrations are felt.
Fremitus varies among persons, but it should be?
Symmetrical; felt in the same corresponding areas on each side.
What are some normals that could affect the normal intensity of tactile fremitus?
- Relative location of bronchi to the chest wall.
- Normally most prominent between the scapulae and around the sternum; sites where the major bronchi are closest to the chest wall.
- It normally decreases with downward progression because more and more tissue impedes the sound transmission.
- Thickness go the chest wall.
- It feels greater over a thin chest wall than over an obese or heavily muscular one where thick tissue dampens the vibration.
- Pitch and intensity.
- A loud, low-pitched voice generates more vibration than a soft, high-pitched one.
What are some abnormals that could cause decreased fremitus?
- When anything obstructs transmission of vibrations (e.g., obstructed bronchus, pleural effusion or thickening, pneumothorax, or emphysema).
- Any barrier that comes between the sound and your palpating hand.
What are some abnormals that could cause increase fremitus?
- Occurs with compression or consolidation of lung tissue (e.g.,
lobar pneumonia).
- This is present only when the bronchus is patent and when the consolidation extends to the lung surface.
Define Rhonchal fremitus.
Palpable with thick bronchial secretions.
Define Pleural friction fremitus.
Palpable with inflammation of the pleura.
Define Crepitus.
A coarse, crackling sensation palpable over the skin surface. It occurs in subcutaneous emphysema when air escapes from the lungs and enters the subcutaneous tissue (as after open thoracic injury or surgery).
Percuss the posterior and anterior chest; over the 1. to determine the 2. Also percuss to map out the lower lung border and measure 3.
- Lung fields
- Predominant note
- Diaphragmatic excursion
What is the predominate sound heard in percussion over the lungs?
Resonance
- Define the percussion sound: Resonance.
- When (why) is it heard?
- Low-pitched, clear, hollow sound.
- Found in healthy lung tissue of adults.
- Define the percussion sound: Hyper-resonance.
- When/why is it heard?
- A lower-pitched booming sound.
- Found when too much air is present (such as emphysema or pneumothorax).
- Define the percussion sound: Dull.
- When/why is it heard?
- A soft, muffled thud.
- Signals abnormal density in the lungs (pneumonia, pleural effusion, atelectasis, or tumor).
Define Atelectasis.
A partial or complete collapsed lung.
When you auscultate the lobes of the lungs, what are two questions you should be asking yourself as you go?
- What AM I hearing in this spot?
- What should I EXPECT to be hearing?
What are the three types of normal breath sounds heard in an adult and older child during auscultation?
- Bronchial (aka tracheal or tubular)
- Bronchovesicular
- Vesicular
What are the characteristics of normal Bronchial (Tracheal) breathing sounds? List the pitch, amplitude, duration, quality, and normal location.
- Pitch: High
- Amplitude: Loud
- Duration: Inspiration < Expiration
- Quality: Harsh, hollow tubular
- Normal location: Trachea and larynx
What are the characteristics of normal Bronchovesicular breathing sounds? List the pitch, amplitude, duration, quality, and normal location.
- Pitch: Moderate
- Amplitude: Moderate
- Duration: Inspiration = Expiration
- Quality: Mixed
- Normal location: Over major bronchi where fewer alveoli
are located.
-
Posterior
- Between scapulae, especially on right.
-
Anterior
- Around upper sternum in 1st and 2nd ICS
-
Posterior
What are the characteristics of normal Vesicular breathing sounds? List the pitch, amplitude, duration, quality, and normal location.
- Pitch: Low
- Amplitude: Soft
- Duration: Inspiration > Expiration
- Quality: Rustling (like the sound of wind in the trees)
- Normal location: Over peripheral lung fields where air flows through small bronchioles and alveoli.
What are three reasons that would decreased or absent breath sounds?
- When the bronchial tree is obstructed at some point by secretions, mucus, plug, or a foreign body.
- In emphysema as
a result of loss of elasticity in the lung fibers and decreased
force of inspired air.
- Also, the lungs are already hyper inflated so the inhaled air doesn't make as much noise.
- When anything obstructs transmission of sound between the lung and your stethoscope, such as pleurisy or pleural thickening, or air (pneumothorax) or fluid (pleural effusion) in the pleural space.
A silent chest means no air is moving in or out, which is an ominous sign.
What are some reasons for increased breath sounds?
- The sounds are louder than they should be (e.g., bronchial sounds are abnormal when they are heard over an abnormal location, the peripheral lung fields).
- They have a high-pitched, tubular quality, with a prolonged expiratory phase and a distinct pause between inspiration and expiration.
- They sound very close to your stethoscope; occur when consolidation (e.g., pneumonia) or compression (e.g., fluid in the intrapleural space) yields a dense lung area that enhances the transmission of sound from the bronchi.
- When inspired air reaches the alveoli, it hits solid lung tissue that conducts sound more efficiently to the surface.
Define Adventitious sounds.
- They are sounds that are not normally heard in the lungs.
- If present, they are heard as being superimposed on the breath sounds.
- They are caused by moving air colliding with secretions in the tracheobronchial passageways or by the popping open of previously deflated airways.
What are discontinuous sounds?
Discrete, crackling sounds.
What are continuous sounds?
Connected, musical sounds.
Describe Fine Crackles (or Rales).
-
Description
- Discontinuous, high-pitched, short crackling, popping sounds heard during inspiration that are not cleared by coughing.
- Sound can be simulated by rolling a strand of hair between your fingers near your ear, or by moistening your thumb and index finger and separating them near your ear.
-
Mechanism
- Inspiratory crackles:
- Inhaled air collides with previously deflated airways.
- Airways suddenly pop open, creating explosive crackling sound.
- Expiratory
crackles:
- Sudden airway closing.
- Inspiratory crackles:
-
Clinical Example
- Late inspiratory crackles
- Occur with restrictive disease: pneumonia, heart failure, and interstitial fibrosis.
- Early inspiratory crackles
- Occur with obstructive disease: chronic bronchitis, asthma, and emphysema.
- Posturally induced crackles (PICs)
- Fine crackles that appear with a change from sitting to the supine position or with a change from supine to supine with legs elevated.
- Late inspiratory crackles
Describe Coarse Crackles (Coarse Rales)
-
Description
- Loud, low-pitched, bubbling and gurgling sounds that start in early inspiration and may be present in expiration.
- May decrease somewhat by suctioning or coughing but will reappear shortly - sounds like opening a Velcro fastener.
-
Mechanism
- Inhaled air collides with secretions in the trachea and large bronchi.
-
Clinical Example
- Pulmonary edema, pneumonia, pulmonary fibrosis, and the terminally ill who have a depressed cough reflex.
Describe Atelectatic Crackles (Atelectatic Rales).
-
Description
- Sounds like fine crackles but do not last and are not pathologic.
- Disappear after the first few breaths.
- Heard in axillae and bases (usually dependent) of lungs.
-
Mechanism
- When sections of alveoli are not fully aerated, they deflate and accumulate secretions.
- Crackles are heard when these sections re-expand with a few deep breaths.
-
Clinical Example
- In aging adults.
- In bedridden persons.
- In persons just aroused from sleep.
Describe Pleural Friction Rub.
-
Description
- A very superficial sound that is coarse and low pitched.
- It has a grating quality as if two pieces of leather are being rubbed together.
- Sounds just like crackles, but close to the ear.
- Sounds louder if you push the stethoscope harder onto the chest wall.
- Sound is inspiratory and expiratory.
-
Mechanism
- Caused when pleurae become inflamed and lose their normal lubricating fluid.
- Their opposing roughened pleural surfaces rub together during respiration.
- Heard best in anterolateral wall where greatest lung mobility exists.
-
Clinical Example
- Pleuritis, accompanied by pain with breathing (rub disappears after a few days if pleural fluid accumulates and separates pleurae).
Describe Wheeze (Sibilant).
-
Description
- High-pitched, musical squeaking sounds that sound polyphonic (multiple notes as in a musical chord).
- Predominate in expiration but may occur in both expiration and inspiration.
-
Mechanism
- Air squeezed or compressed through passageways narrowed almost to closure by collapsing, swelling, secretions, or tumors.
- The passageway walls oscillate in apposition between the closed and barely open positions.
- The resulting sound is similar to a vibrating reed.
-
Clinical Example
- Diffuse airway obstruction from acute asthma or chronic emphysema.
Describe Wheeze (Sonorous Rhonchi).
-
Description
- Low-pitched, monophonic single note, musical snoring, moaning sounds.
- They are heard throughout the cycle, although they are more prominent on expiration.
- May clear somewhat by coughing.
-
Mechanism
- Airflow obstruction as described by the vibrating reed mechanism from the high-pitched wheezing.
- The pitch of the wheeze cannot be correlated to the size of the passageway that generates it.
-
Clinical Example
- Bronchitis, single bronchus obstruction from airway tumor.
Are atelectatic crackles an adventitious sound? Why or why not?
- Not an adventitious sound.
- They are short, popping, crackling sounds (fine crackles), but do not last beyond a few breaths.
- In older adults or people who are asleep, sections of alveoli are not fully aerated, since they deflate slightly and accumulate secretions.
- Crackles are heard when these secretions are expanded by a few deep breaths.
- They are only heard in the periphery, usually in dependent portions of the lungs, and disappear after the first few breaths or after a cough.
Normally there should be no retraction or bulging of the interspaces during inspiration. What could be indicated if the abnormal findings of retraction and bulging are seen?
- Retraction suggests obstruction of respiratory tract or increased inspiratory effort is needed (as with atelectasis).
- Bulging indicates trapped air as in forced expiration associated with emphysema or asthma.
Describe the characteristics of Scoliosis.
- A lateral S-shaped curvature of the thoracic and lumbar spine.
- Usually involves vertebrae rotation.
- Note:
- Unequal shoulder
- Scapular height
- Unequal hip levels
- Rib interspaces flared on convex side.
- More prevalent in adolescent age-groups, especially girls.
- If severe (> 45 degrees), it may reduce lung volume and person is at risk for impaired cardiopulmonary function.
Describe the respiratory pattern of a Normal Adult.
- Rate: 10-20 breaths per minute.
- Depth: 500-800 mL; air moving in and out with each respiration.
- Pattern: Even.
- The ratio of pulse to respiratory is fairly constant;
about 4:1.
- Both values increase as a normal response to exercise, fear, or fever.
Describe the respiratory pattern of a Sigh.
- Occasionally punctures the normal breathing pattern and purposefully expands alveoli.
- If frequent, it may indicate
emotional dysfunction.
- It may also lead to hyperventilation and dizziness.
Describe the respiratory pattern of a Tachypnea.
- Rapid, shallow breathing.
- Increased rate: > 24 per minute.
- Normal response to fever, fear, or exercise.
- Rate also increases with:
- Respiratory insufficiency
- Pneumonia
- Alkalosis
- Pleurisy
- Lesions in the pons.
Describe the respiratory pattern of a Bradypnea .
- Slow breathing.
- A decreased, but regular rate: < 10 per minute.
- As in:
- Drug-induced depression of the respiratory center in the medulla.
- Increased intracranial pressure
- Diabetic coma
Describe the respiratory pattern of a Hyperventilation.
- Increased rate and depth.
- Normally occurs with extreme exertion, fear, or anxiety.
- Also occurs with:
- Diabetic ketoacidosis (Kussmaul respirations).
- Hepatic coma.
- Salicylate overdose.
- Producing a respiratory alkalosis to compensate for the metabolic acidosis.
- Lesions in the midbrain.
- Alteration in blood gas concentration.
- Either an increase in CO2 or a decrease in O2.
- It blows off CO2, causing a decreased level in the blood (alkalosis).
Describe the respiratory pattern of a Hypoventilation.
- An irregular shallow pattern.
- Caused by an overdose of narcotics or anesthetics.
- May also occur with prolonged bedrest or conscious splinting of the chest to avoid respiratory pain.
Describe the respiratory pattern of a Cheyne-Stokes Respiration.
- Aka "Death breathing" or agonal breathing.
- A
cycle in which respiration gradually wax and wane in a regular
pattern.
- Increasing in rate and depth, then decreasing.
- The breathing periods last 30-45 seconds, with periods of apnea (20 seconds) alternating the cycle.
- The most common cause is severe heart failure, or:
- Renal failure
- Meningitis
- Drug overdose
- Increased intracranial pressure
- Occurs normally in infants and aging persons during sleep.
Describe the respiratory pattern of a Chronic Obstructive Breathing.
- Normal inspiration and prolonged expiration to overcome increased airway resistance.
- In a person with chronic obstructive lung disease, any situation calling for increased heart rate (ex. exercise) may lead to dyspneic episode (air trapping), because then the person doesn't have enough time for full expiration.
Describe the Assessment of the Common Respiratory Conditions of Lobar Pneumonia.
- Condition
- Infection in lung parenchyma leaves alveolar membrane edematous and porous, so RBCs and WBCs pass from blood to alveoli.
- Alveoli progressively fill up (become consolidated) with bacteria, solid cellular debris, fluid, and blood cells, which replace alveolar air.
- This decreases surface area of the respiratory membrane, causing hypoxemia.
- Inspection
- Increased respiratory rate.
- Guarding and lag on expansion on affected side.
- In children: sternal retraction and nasal flaring.
- Palpation
- Chest expansion decreased on affected side.
- Tactile fremitus increased if bronchus patent, decreased if bronchus obstructed.
- Percussion
- Dull over lobar pneumonia.
- Auscultation
- Breath sounds louder with patent bronchus, as if coming directly from larynx.
- Voice sounds have increased clarity.
- Bronchophony, egophony, whispered pectoriloquy present.
- In children: diminished breath sounds may occur early in pneumonia.
- Adventitious Sounds
- Crackles, fine to medium.
What is some subjective data for Lobar Pneumonia?
Pt. c/o:
- Dyspnea
- Fatigue
- Cough (may be productive)
- Chest pain
- Back pain
- Possible fever
What is some objective data for Lobar Pneumonia?
- Increase respiratory rate.
- Chest expansion decreased.
- Rales over affected area.
- Dull to percussion over affected area.
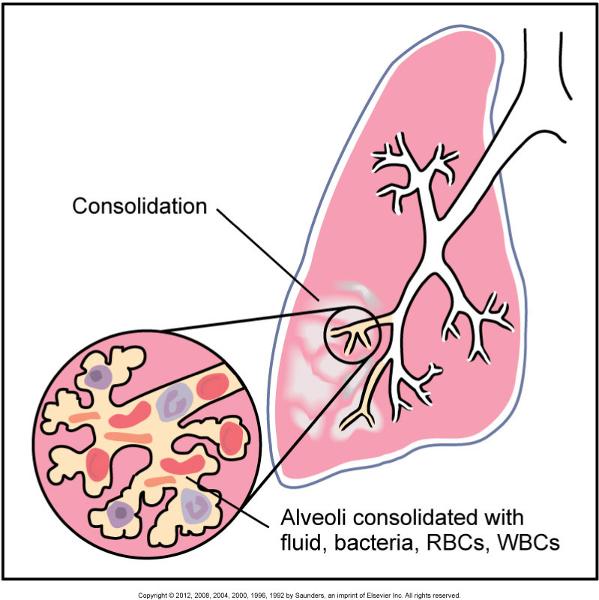
Lobar Pneumonia
Describe the Assessment of the Common Respiratory Conditions of Bronchitis.
- Condition
- Proliferation of mucus glands in the passageways, resulting in excessive mucus secretion.
- Inflammation of bronchi with partial obstruction of bronchi by secretions or constrictions.
- Sections of lung distal to obstruction may be deflated.
- Bronchitis may be acute or chronic with recurrent productive cough.
- Chronic bronchitis is usually caused by cigarette smoking.
- Inspection
- Hacking, rasping cough productive of thick mucoid sputum.
- Chronic: dyspnea, fatigue, cyanosis, possible clubbing of fingers.
- Palpation
- Tactile fremitus normal.
- Percussion
- Resonant.
- Auscultation
- Normal vesicular.
- Voice sounds normal.
- Chronic: prolonged expiration.
- Adventitious Sounds
- Crackles over deflated areas.
- May have wheeze.
What is some subjective data for Acute Bronchitis?
Pt. c/o:
- Acute or chronic, dry cough
- Dyspnea
- Increase respiratory rate
- Sputum production
- Fatigue
What is some objective data for Acute Bronchitis?
- Palpation and Percussion findings normal.
- Crackles over area of obstruction.
- May have wheezes.
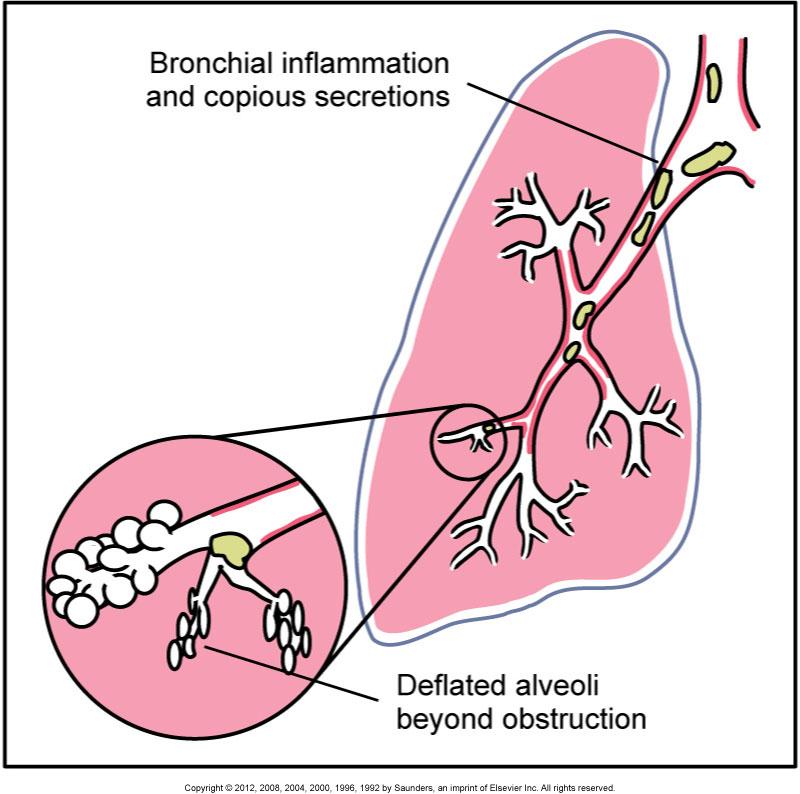
Bronchitis
Describe the Assessment of the Common Respiratory Conditions of Emphysema.
- Condition
- Caused by destruction of pulmonary connective tissue (elastin, collagen).
- Characterized by permanent enlargement of air sacs distal to terminal bronchioles and rupture of inter alveolar walls.
- This increases airway resistance, especially on expiration - producing a hyper-inflated lung and an increase in lung volume.
- Cigarette smoking accounts for 80%-90% of cases of emphysema.
- Inspection
- Increased anteroposterior diameter.
- Barrel chest.
- Use of accessory muscles to aid respiration.
- Tripod position.
- Shortness of breath, especially on exertion.
- Respiratory distress.
- Tachypnea.
- Palpation
- Decreased tactile fremitus and chest expansion.
- Percussion
- Hyper-resonant.
- Decreased diaphragmatic excursion.
- Auscultation
- Decreased breath sounds.
- May have prolonged expiration.
- Muffled heart sounds resulting from over-distention of lungs.
- Adventitious Sounds
- Usually none.
- Occasionally, wheeze.
What is some subjective data for Emphysema?
Pt. c/o:
- Dyspnea (also DOE)
- Increase respirations
What is some objective data for Emphysema?
- Increase respiratory rate.
- Use of accessory muscles.
- Barrel chest (chronic).
- Cyanosis.
- Tactile fremitus decreased.
- Breath sounds decreased.
- May have bilateral wheezing.
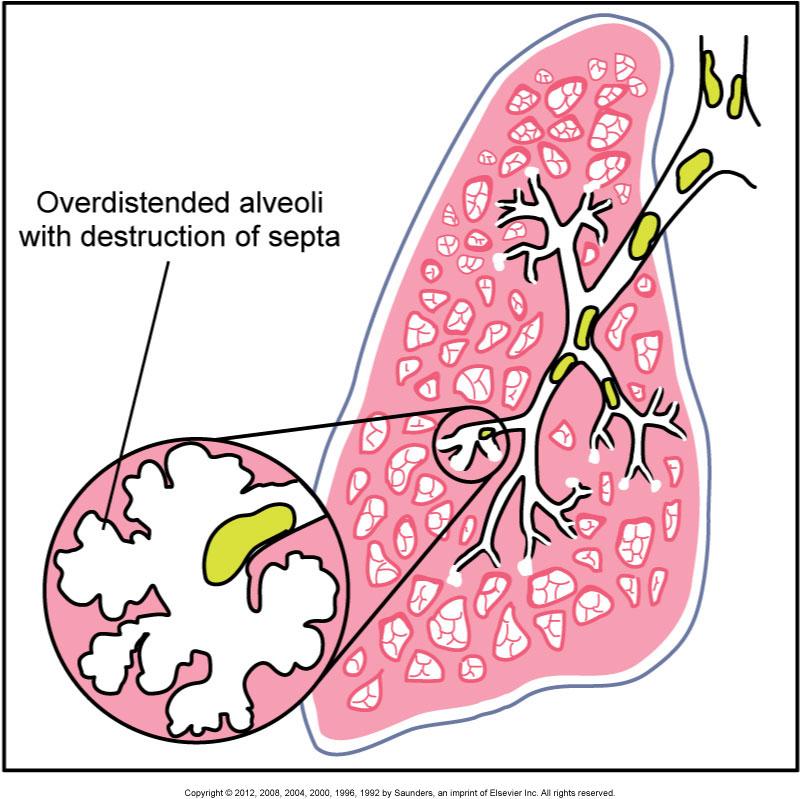
Emphysema
Describe the Assessment of the Common Respiratory Conditions of Asthma (aka Reactive Airway Disease) .
- Condition
- An allergic hypersensitivity to certain inhaled allergens (pollen), irritants (tobacco, ozone), microbes, stress, or exercise that produces a complex response characterized by bronchospasm and inflammation, edema in walls of bronchioles, and secretion of highly viscous mucus not airways.
- These factors greatly increase airway resistance, especially during expiration, and produce the symptoms of wheezing, dyspnea, and chest tightness.
- Inspection
- During severe attack:
- Increased respiratory rate
- SOB with audible wheeze
- Use of accessory muscles
- Cyanosis
- Apprehension
- Retraction of ICSs
- Expiration labored, prolonged.
- When chronic, may have barrel chest.
- During severe attack:
- Palpation
- Decreased tactile fremitus.
- Tachycardia.
- Percussion
- Resonant.
- May be hyper-resonant if chronic.
- Auscultation
- Diminished air movement.
- Breath sounds decreased, with prolonged expiration.
- Voice sounds decreased.
- Adventitious Sounds
- Bilateral wheezing on expiration
- Sometimes inspiratory and expiratory wheezing.
What is some subjective data for Asthma?
- Dyspnea
- Increase respiratory rate
- Wheezing
- Use of accessory muscles
What is some objective data for Asthma?
- Tactile fremitus decreased.
- Inspiratory & Expiratory wheezing.
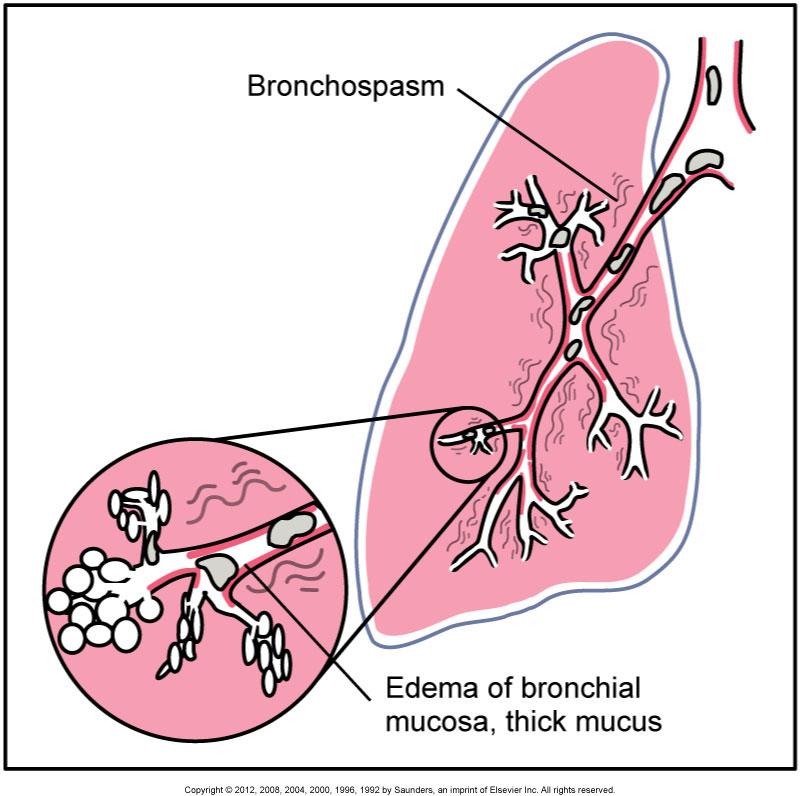
Asthma