A critical early step in designing an EHR is to develop a(n) _____ in which the characteristics of each data element are defined.
- Accreditation Manual
- Core Content
- Continuity of Care Record
- Data Dictionary
D. Data Dictionary
Once hospital discharge abstract systems were developed and their ability to provide comparative data to hospitals was established, it became necessary to develop _____.
- Data Sets
- Data Elements
- Electronic Data Interchange
- Bills of Mortality
- Data Sets
In healthcare, data sets serve two purposes. The first purpose is to identify data elements to be collected about each patient. The second is to _____.
- Provide Uniform Data Definitions
- Guide Efforts Toward Computerization
- Determine Statistical Formulas
- Provide a Research Database
- Provide Uniform Data Definitions
A health information technician has been charged with the responsibility of designing a data collection form to be used on admission of a patient to the acute care hospital in which she works. The first resource that she should use is _____.
- UHDDS
- UACDS
- MDS
- ORYX
- UHDDS
Which of the following is NOT a characteristic of the common healthcare data sets such as UHDDS and UACDS?
- They define minimum data elements to be collected.
- They provide a complete and exhaustive list of data elements that must be collected.
- They provide a framework for data collection to which an individual facility can add data items.
- The federal government recommends, but does not mandate, implementation of most of the data sets.
B. They provide a complete and exhaustive list of data elements that must be collected.
A corporation is evaluating several health plans for its benefits package. The data set that provides comparison information about health plan performance is _____.
- ORYX
- HEDIS
- UHDDS
- MDS
B. HEDIS
The name of the government agency that has led the development of basic data sets for health records and computer data bases is _____.
- Centers for Medicare and Medicaid Services
- Johns Hopkins University
- American National Standards Institute
- National Committee on Vital and Health Statistics
D. National Committee on Vital and Health Statistics
The primary purpose of a minimum data set in healthcare is to _____.
- Recommend Common Data Elements to be Collected in Health Records.
- Mandate All Data That Must be Contained in a Health Record.
- Define Reportable Data for Federally Funded Programs.
- Standardize Medical Vocabulary.
- Recommend Common Data Elements to be Collected in Health Records.
The inpatient data set that has been incorporated into federal law and is required for Medicare reporting is the _____.
- Ambulatory Care Data Set
- Uniform Hospital Discharge Data Set
- Minimum Data Set for Long-Term Care
- Health Plan Employer Data and Information Set
B. Uniform Hospital Discharge Data Set
Both HEDIS and the Joint Commission's ORYX programs are designed to collect data to be used for _____.
- Performance Improvement Programs
- Billing and Claims Data Processing
- Developing Hospital Discharge Abstracting Systems
- Developing Individual Care Plans for Residents
A. Performance Improvement Programs
While the focus of inpatient data collection in the UHDDS is on principal diagnosis, the focus of outpatient data collection in the UACDS is on _____.
- Reason for Admission
- Reason for Encounter
- Discharge Diagnosis
- Activities of Daily Living
B. Reason for Encounter
In long term care, the resident's care plan is based on data collected in the _____.
- UHDDS
- OASIS
- MDS Version 2.0
- HEDIS
C. MDS Version 2.0
Reimbursement for home health services is dependent on data collected from _____.
- HEDIS
- UHDDS
- OASIS
- MDS Version 2.0
C. OASIS
Each of the three dimensions (personal, provider, and community) of information defined by the National Health Information Infrastructure (NHII) contains specific recommendations for _____.
- Government Regulations
- Core Data Elements
- Privacy Controls
- Technology Requirements
B. Core Data Elements
A core data set developed by ASTM to communicate a patient's past and current health information as the patient transitions from one care setting to another is _____.
- Continuity of Care Record
- Minimum Data Set
- Ambulatory Care Data Set
- Uniform Hospital Discharge Data Set
A. Continuity of Care Record
The home health prospective payment system uses the _____ data set for patient assessments.
- HEDIS
- OASIS
- MDS
- UHDDS
B. OASIS
The government agency most closely involved in the development of healthcare data sets and information standards is _____.
- Centers of Medicare and Medicaid Services
- Department of Health and Human Services
- Johns Hopkins University
- National Centers for Health Statistics
D. National Centers for Health Statistics
The data set designed to organize data for public release about the outcomes of care is _____.
- UHDDS
- DEEDS
- MDS
- HEDIS
D. HEDIS
OASIS data are used to assess the _____ of home health services.
- Outcome
- Financial Performance
- Utilization
- Core Measure
A. Outcome
Which of the following indexes and databases includes patient-identifiable information?
- MEDLINE
- Clinical Trials Database
- Master Patient/Population Index
- UMLS
C. Master Patient/Population Index
Occasionally gets hungry. No insulin reactions. Says she is following her diabetic diet."
In which part of a POMR progress note would this notation be written?
- Subjective
- Objective
- Assessment
- Plan
A. Subjective
A notation for a diabetic patient in a physician progress note reads:
"FBS 110 mg%, urine sugar, no acetone."
In which part of a POMR progress note would this notation be written?
- Subjective
- Objective
- Assessment
- Plan
B. Objective
A notation for a hypertensive patient in a physician ambulatory care progress note reads:
"Continue with Duril, 500 mgs once daily. Return visit in 2 weeks."
In which part of a POMR progress note would this notation be written?
- Subjective
- Objective
- Assessment
- Plan
D. Plan
A notation for a hypertensive patient in a physician ambulatory care progress note reads:
"Blood pressure adequately controlled."
In which part of a POMR progress note would this notation be written?
- Subjective
- Objective
- Assessment
- Plan
C. Assessment
The set of all terms that may be used in a language is referred to as a _____.
- Classification
- Nomenclature
- Nominal Data
- Vocabulary
D. Vocabulary
Which of the following promotes uniform reporting and statistical data collection for medical procedures, supplies, products, and services?
- Current Procedural Terminology
- Healthcare Common Procedure Coding System
- International Classification of Diseases, Ninth Revision, Clinical Modification
- International Classification of Diseases for Oncology, Third Edition
B. Healthcare Common Procedure Coding System
Which of the following provides a detailed classification system for coding the histology, topography, and behavior of neoplasms?
- Current Procedural Terminology
- Healthcare Common Procedure Coding System
- International Classification of Diseases for Oncology, Third Edition
- Systematized Nomenclature of Medicine Clinical Terminology
C. International Classification of Diseases for Oncology, Third Edition
Which of the following provides a standardized vocabulary for facilitating the development of computer-based patient records?
- Current Procedural Terminology
- Healthcare Common Procedure Coding System
- International Classification of Diseases, Ninth Revision, Clinical Modification
- Systematized Nomenclature of Medicine Clinical Terminology
D. Systematized Nomenclature of Medicine Clinical Terminology
Which of the following provides a system for classifying morbidity and mortality information for statistical purposes?
- Current Procedural Terminology
- Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition
- Healthcare Common Procedure Coding System
- International Classification of Diseases, Ninth Revision, Clinical Modification
D. International Classification of Diseases, Ninth Revision, Clinical Modification
Which of the following is not a knowledgeable source for users of the Unified Medical Language System?
- Concept Table
- Semantic Network
- Metathesaurus
- Specialist Lexicon
A. Concept Table
Nosology can be defined the branch of medical science that deals with _____.
- Cosmetic Surgery
- Hospital-Acquired Infections
- Nursing Diagnoses
- Classification Systems
D. Classification Systems
Which of the following classifications is used exclusively for classifying cases of malignant disease?
- CPT
- HCPCS
- ICD-9-CM
- ICD-O-3
D. ICD-O-3
Which of the following provides the most comprehensive controlled vocabulary for coding the content of a patient record?
- CPT
- HCPCS
- ICD-9-CM
- SNOMED
D. SNOMED
Which of the following provides a set of codes used for collecting data about substance abuse and mental health disorders?
- CPT
- DSM-IV-TR
- HCPCS
- SNOMED-CT
B. DSM-IV-TR
Dr. Jones entered a progress note in a patient's health record 24 hours after he visited the patient. Which quality element is missing from the progress note?
- Data Completeness
- Data Relevancy
- Data Currency
- Data Precision
C. Data Currency
The admitting data of Mrs. Smith's health record indicated that her birth date was March 21, 1948. On the discharge summary, Mrs. Smith's birth date was recorded as July 21, 1948. Which quality element is missing from Mrs. Smith's health record?
- Data Completeness
- Data Consistency
- Data Accessibility
- Data Comprehensiveness
B. Data Consistency
The term used to describe expected data values is _____.
- Data Definition
- Data Currency
- Data Precision
- Data Relevancy
C. Data Precision
The diagnosis of a patient was recorded as an abscess in the procedure report, but was listed as carcinoma on the discharge summary. This is an example of a problem with:
- Data Granularity
- Data Consistency
- Data Precision
- Data Relevance
C. Data Precision
Which of the following is a primary weakness of the paper-based health record?
- Difficulty to Provide Availability to a Number of Providers at the Same Time
- Poor Communication Tool
- Difficulty in Documenting Healthcare Process
- Lack of Available Resources
A. Difficulty to Provide Availability to a Number of Providers at the Same Time
Which of the following elements is not a component of most patient records?
- Patient Identification
- Clinical History
- Financial Information
- Test Results
C. Financial Information
Which of the following is not a characteristic of high-quality healthcare data?
- Data Relevancy
- Data Currency
- Data Consistency
- Data Accountability
D. Data Accountability
Which of the following represents an example of data granularity?
- A Progress Note Recorded at or Near the Time of the Observation
- An Acceptable Range of Values Defined for a Clinical Characteristic
- A Numerical Measurement Carried Out to the Appropriate Decimal Place
- A Health Record That Includes All of the Required Components
C. A Numerical Measurement Carried Out to the Appropriate Decimal Place
Which of the following is a primary purpose of the health record?
- Document Patient Care Delivery
- Assist Caregivers in Patient Care Management
- Aid in Billing and Reimbursement Functions
- Assist in Process Redesign
A. Document Patient Care Delivery
Which of the following best describes data accuracy?
- Data Are Correct
- Data Are Easy to Obtain
- Data Include All Required Elements
- Data Are Reliable
A. Data Are Correct
Which of the following best describes data completeness?
- Data Are Correct
- Data Are Easy to Obtain
- Data Include All Required Elements
- Data Are Reliable
C. Data Include All Required Elements
Which of the following best describes data accessibility?
- Data Are Correct
- Data Are Easy to Obtain
- Data Include All Required Elements
- Data Are Reliable
B. Data Are Easy to Obtain
In which department/unit does the health record typically begin?
- HIM Department
- Patient Registration
- Nursing Unit
- Billing Department
B. Patient Registration
Identify where the following information would be found in the acute care record:
"Following induction of an adequate general anesthesia, and with the patient supine on the padded table, the upper left extremity was prepped and draped in the standard fashion."
- Anesthesia Report
- Physician Progress Notes
- Operative Report
- Recovery Room Record
C. Operative Report
Identify where the following information would be found in the acute care record:
"CBC: WBC 12.0, RBC 4.65, HGB 14.8, HCT 43.3, MCV 93."
- Medical Laboratory Report
- Pathology Report
- Physical Examination
- Physician Orders
A. Medical Laboratory Report
Identify where the following information would be found in the acute care record:
"PA and Lateral Chest: The lungs are clear. The heart and mediastinum are normal in size and configuration. There are minor degenerative changes of the lower thoracic spine."
- Medical Laboratory Report
- Physical Examination
- Physician Progress Note
- Radiography Report
D. Radiography Report
The attending physician is responsible for which of the following types of acute care documentation?
- Consultation Report
- Discharge Summary
- Laboratory Report
- Pathology Report
B. Discharge Summary
A nurse is responsible for which of the following types of acute care documentation?
- Operative Report
- Medication Record
- Radiology Report
- Therapy Assessment
B. Medication Record
Which of the following is an example of clinical data?
- Admitting Diagnosis
- Date and Time of Admission
- Insurance Information
- Health Record Number
A. Admitting Diagnosis
Documentation of aides who assist a patient with activities of daily living, bathing, laundry, and cleaning would be found in which type of specialty record?
- Home Health
- Behavioral Health
- End Stage Renal Disease
- Rehabilitative Care
A. Home Health
The following is documented in an acute care record:
"HEENT: Reveals the tympanic membranes, nares, and pharynx to be clear. No obvious head trauma.
CHEST: Good bilateral chest sounds."
In which of the following would this documentation appear?
- History
- Pathology Report
- Physical Examination
- Operation Report
C. Physical Examination
The following is documented in an acute care record:
"Microscopic: Sections are of squamous mucosa with no atypia."
In which of the following would this documentation appear?
- History
- Pathology Report
- Physical Examination
- Operation Report
B. Pathology Report
The following is documented in an acute care record:
"Admit to 3C. Diet: NPO, Meds: Compazine 10mg, IV Q 6 PRN."
In which of the following would this documentation appear?
- Admission Order
- History
- Physical Examination
- Progress Notes
A. Admission Order
The following is documented in an acute care record:
"Following induction of an adequate general anesthesia, and with the patient supine on the padded table, the upper left extremity was prepped and draped in the standard fashion."
- Anesthesia Report
- Discharge Summary
- Operation Report
- Progress Notes
C. Operation Report
The following is documented in an acute care record:
"CBC: WBC 12.0H, RBC 4.65, HGB 14.8, HCT 43.3, MCV 93."
In which of the following would this documentation appear?
- Anesthesia Report
- Clinical Laboratory Report
- Respiratory Therapy Report
- Radiology Report
B. Clinical Laboratory Report
The following is documented in an acute care record:
"38 weeks gestation, Apgars 8/9, 6# 9.8 oz, good cry."
In which of the following would this documentation appear?
- Admission Note
- Clinical Laboratory
- Newborn Record
- Physician Order
C. Newborn Record
The following is documented in an acute care record:
"Atrial fibrillation with rapid ventricular response, left axis deviation, left bundle branch block."
In which of the following would this documentation appear?
- Admission Order
- Clinical Laboratory Report
- ECG Report
- Radiology Report
C. ECG Report
The following is documented in an acute care record:
"I was asked to evaluate this Level I trauma patient with an open left humeral epicondylar fracture. Recommendations: Proceed with urgent surgery for debridement, irrigation, and treatment of open fracture."
In which of the following would this documentation appear?
- Admission Note
- Consultation Report
- Discharge Summary
- Nursing Progress Notes
B. Consultation Report
The following is documented in an acute care record:
"Spoke to the attending re: my assessment. Provided adoption and counseling information. Spoke to CPS re: Referral. Case manager to meet with patient and family."
In which of the following would this documentation appear?
- Admission Note
- Nursing Note
- Physician Progress Note
- Social Work Note
D. Social Work Note
Which of the following is not usually a part of quantitative analysis review?
- Checking that all forms contain the patient's name and health record number.
- Checking that all forms and reports are present.
- Checking that every word in the record is spelled correctly.
- Checking that reports requiring authentication have signatures.
C. Checking that every word in the record is spelled correctly.
Which of the following materials is not documented in an emergency care record?
- Patients' instructions at discharge.
- Time and means of the patient's arrival.
- Patient's complete medical history.
- Emergency care administered before arrival at the facility.
C. Patient's complete medical history.
Which of the following provides macroscopic and microscopic information about tissue removed during an operative report?
- Anesthesia Report
- Laboratory Report
- Operative Report
- Pathology Report
D. Pathology Report
Sleeping patterns, head and chest measurements, feeding and elimination status, weight and Apgar scores are recorded in which of the following records?
- Emergency
- Newborn
- Obstetric
- Surgical
B. Newborn
In a problem-oriented medical record, problems are organized _____.
- In Alphabetical Order
- In Numeric Order
- In Alphabetical Order by Body System
- By Date of Onset
B. In Numeric Order
What is the defining characteristic of an integrated health record format?
- Each section of the record is maintained by the patient care department that provided the care.
- Integrated health records are intended to be used in ambulatory settings.
- Integrated health records include both paper forms and computer printouts.
- Integrated health records components are arranged in strict chronological order.
D. Integrated health records components are arranged in strict chronological order.
Which of the following represents documentation of the patient's current and past health status?
- Physical Exam
- Medical History
- Physician Orders
- Patient Consent
B. Medical History
Which of the following contains the physician's findings based on an examination of the patient?
- Physical Exam
- Discharge Summary
- Medical Summary
- Patient Instructions
A. Physical Exam
What is the function of a consultation report?
- Provides a chronological summary of the patient's medical history and illness.
- Documents opinions about the patient's condition from the perspective of a physician not previously involved in the patient's care.
- Concisely summarizes the patient's treatment and stay in the hospital.
- Documents the physician's instructions to other parties involved in providing care to a patient.
B. Documents opinions about the patient's condition from the perspective of a physician not previously involved in the patient's care.
What is the function of physician's orders?
- Provides a chronological summary of the patient's medical history and illness.
- Document the patient's current and past health status.
- Documents the physician's instructions to other parties involved in providing care to a patient.
- Document the provider's instructions for follow-up care given to the patient or patient's caregiver.
C. Documents the physician's instructions to other parties involved in providing care to a patient.
What type of patient care record includes documentation of a family bereavement period?
- Hospice Record
- Home Health Record
- Long-Term Care Record
- Ambulatory Record
A. Hospice Record
Reviewing the health record for missing signatures, missing medical reports, and ensuring that all documents belong in the health record is an example of _____ review.
- Quantitative
- Qualitative
- Statistical
- Outcomes
A. Quantitative
Which of the following is a secondary purpose of the health record?
- Support for provider reimbursement.
- Support for patient self-management activities.
- Support for research.
- Support for patient care delivery.
C. Support for research.
Use of the health record by a clinician to facilitate quality patient care is considered _____.
- A primary purpose of the health record.
- Patient care support.
- A secondary purpose of the health record.
- Policy making and support.
A. A primary purpose of the health record.
Use of the health record to monitor bioterrorism activity is considered a _____.
- A primary purpose of the health record.
- A secondary purpose of the health record.
- Patient use of the health record.
- Healthcare licensing agency function.
B. A secondary purpose of the health record.
In designing an electronic health record, one of the best resources to use in helping to define the content of the record as well as to standardize data definitions is the E1384 standard promulgated by the _____.
- Centers for Medicare and Medicaid Services (CMS)
- American Society for Testing and Measurement (ASTM)
- Joint Commission (JC)
- National Centers for Health Statistics (NCHS)
B. American Society for Testing and Measurement (ASTM)
The _____ mandated the development of standards for electronic medical records.
- Medicare and Medicaid Legislation of 1965
- Prospective Payment Act of 1983
- Health Insurance Portability and Accountability Act (HIPAA) of 1996
- Balanced Budget Act of 1997
C. Health Insurance Portability and Accountability Act (HIPAA) of 1996
Messaging standards for electronic data interchange in healthcare have been developed by _____.
- HL7
- IEE
- The Joint Commission
- CMS
A. HL7
A statement or guideline that directs decision making or behavior is called a _____.
- Directive
- Procedure
- Policy
- Process
C. Policy
Which of the following is the planned replacement for ICD-9-CM Volumes 1 and 2?
- Current Procedural Terminology (CPT)
- International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)
- International Classification of Diseases, Tenth Revision (ICD-10)
- International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)
D. International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)
Which organization originally published ICD-9?
- American Medical Association (AMA)
- Centers for Disease Control (CDC)
- United States Federal Government
- World Health Organization (WHO)
D. World Health Organization (WHO)
Which of the following organizations is responsible for updating the procedure classification of ICD-9-CM?
- Centers for Disease Control (CDC)
- Centers for Medicare and Medicaid Services (CMS)
- National Center for Health Statistics (NCHS)
- World Health Organization (WHO)
B. Centers for Medicare and Medicaid Services (CMS)
At which level of the classification system are the most specific ICD-9-CM codes found?
- Category Level
- Section Level
- Subcategory Level
- Subclassification Level
D. Subclassification Level
What are five-digit ICD-9-CM diagnosis codes referred to as?
- Category Codes
- Section Codes
- Subcategory Codes
- Subclassification Codes
D. Subclassification Codes
What are four-digit ICD-9-CM diagnosis codes referred to as?
- Category Codes
- Section Codes
- Subcategory Codes
- Subclassification Codes
C. Subcategory Codes
Which of the following ICD-9-CM codes are always alphanumeric?
- Category Codes
- Procedure Codes
- Subcategory Codes
- V Codes
D. V Codes
Which of the following ICD-9-CM codes classify environmental events and circumstances as the cause of an injury, poisoning, or other adverse effect?
- Category Codes
- E Codes
- Subcategory Codes
- V Codes
B. E Codes
Which volume of ICD-9-CM contains the tabular and alphabetic lists of procedures?
- Volume 1
- Volume 2
- Volume 3
- Volume 4
C. Volume 3
Which of the following provides a system for coding the clinical procedures and services provided by physicians and other clinical professionals?
- Current Procedural Terminology (CPT)
- Diagnostic and Statistical Manual of Mental Disorders, Fourth Revision
- Healthcare Common Procedure Coding System
- International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)
A. Current Procedural Terminology (CPT)
Which of the following is used to report the healthcare supplies, products, and services provided to patients by healthcare professionals?
- CPT
- HCPCS
- ICD-9-CM
- SNOMED CT
B. HCPCS
Which of the following is a standard terminology used to code medical procedures and services?
- CPT
- HCPCS
- ICD-9-CM
- SNOMED CT
A. CPT
Which of the following elements of coding quality represent the degree to which codes accurately reflect the patient's diagnoses and procedures?
- Reliability
- Validity
- Completeness
- Timeliness
B. Validity
A patient is admitted to the hospital with acute lower abdominal pain. The principal diagnosis is acute appendicitis. The patient also has a diagnosis of diabetes. The patient undergoes an appendectomy and subsequently develops to wound infections. In the DRG system, which of the following would be considered a comorbidity in this case?
- Acute Appendicitis
- Appendectomy
- Diabetes
- Wound Infection
C. Diabetes
A health information technician is processing payments for hospital outpatient services to be reimbursed by Medicare for a patient who had two physician visits, underwent radiology examinations, clinical laboratory tests, and who received take-home surgical dressings. Which of the following could be reimbursed under the outpatient prospective payment system?
- Clinical Laboratory Tests
- Physician Office Visits
- Radiology Examinations
- Take-Home surgical Dressings
C. Radiology Examinations
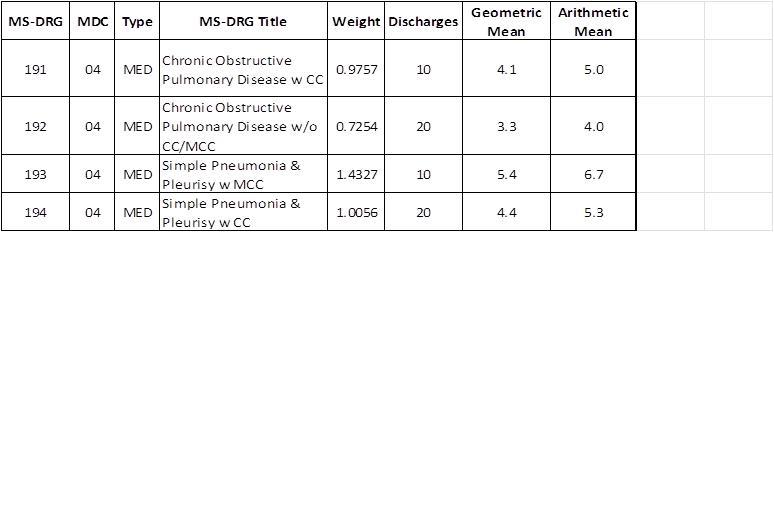
Given the information here, which of the following statements is correct?
- In each MS-DRG the geometric mean is lower than the arithmetic mean.
- In each MS-DRG the arithmetic mean is lower than the geometric mean.
- The higher the number of patients in wach MS-DRG, the greater the geometric mean for that MS-DRG period.
- The geometric means are lower in MS-DRGs that are associated with a CC or MCC.
<p>A. In each MS-DRG the geometric mean is lower than the arithmetic mean.</p> <br>
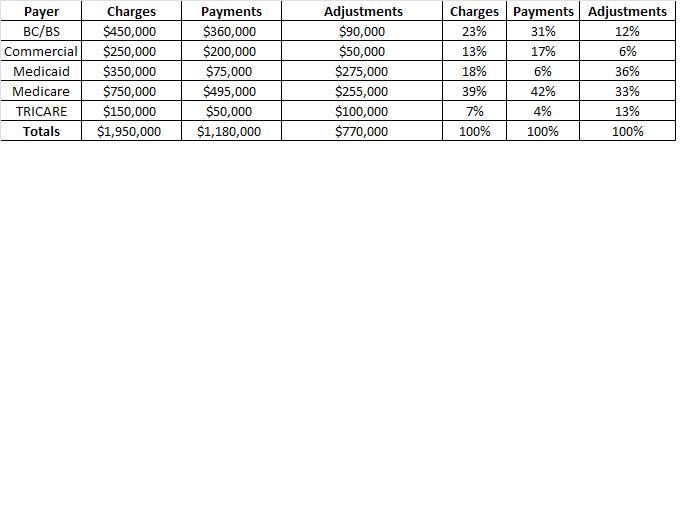
Given the following information, from which payer does the hospital proportionately receive the least amount of payment?
- BC/BS
- Medicaid
- Medicare
- TRICARE
B. Medicaid
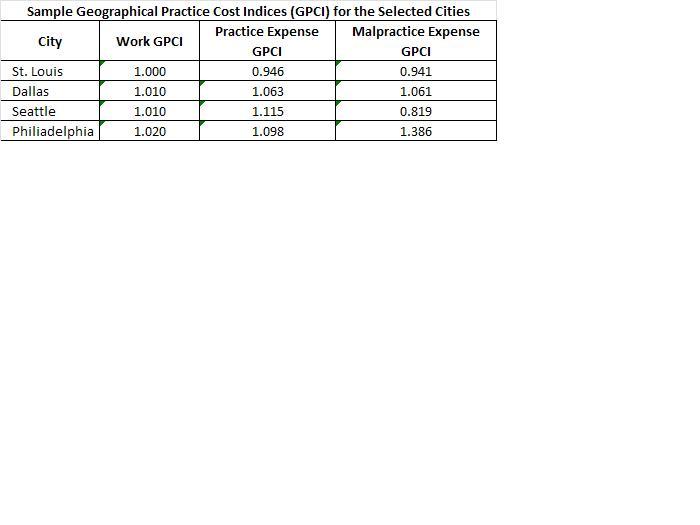
Given the following information, in which city is the GPCI the highest for practice expense?
- St. Louis
- Dallas
- Seattle
- Philiadelphia
C. Seattle
What term is used for retrospective cash payments paid by the patient for services rendered by a provider?
- Fee-for-Service
- Deductible
- Retrospective
- Prospective
A. Fee-for-Service
Which of the following is the condition established after study to be the reason for hospitalization?
- Case Mix
- Complication
- Comorbidity
- Principal Diagnosis
D. Principal Diagnosis
In which of the following payment systems is the amount of payment determined before the service is delivered?
- Fee-for-Service
- Per Diem
- Prospective
- Retrospective
C. Prospective
Which of the following is a prospective payment system implemented for payment of inpatient services?
- APC
- DRG
- OPPS
- RBRVS
B. DRG
In the Inpatient Prospective Payment System assignment to a DRG begins with the _____.
- Principal Diagnosis
- Primary Diagnosis
- Secondary Diagnosis
- Surgical Procedure
A. Principal Diagnosis
Which of the following types of hospitals are excluded from the Medicare inpatient prospective payment system?
- Children's
- Rural
- State Supported
- Tertiary
A. Children's
Diagnosis-related groups are organized into _____.
- Case-Mix Classifications
- Geographic Practice Cost Indices
- Major Diagnostic Categories
- Resource-Based Relative Values
C. Case-Mix Classifications
MS-DRGs may be split into a maximum of _____ payment tiers based on severity as determined by the presence of a major complication/comorbidity, a CC; or no CC.
- Two
- Three
- Four
- Five
B. Three
The purpose of the present on admission (POA) indicator is to _____.
- Differentiate between conditions present on admission and conditions that develop during an inpatient admission.
- Track principal diagnoses.
- Distinguish between principal and primary diagnoses.
- Determine principal diagnosis.
A. Differentiate between conditions present on admission and conditions that develop during an inpatient admission.
The present on admission (POA) indicator for
- Inpatient Medicare claims submitted by all hospitals.
- Inpatient Medicare and Medicaid claims submitted by all hospitals.
- Medicare claims submitted by all entities.
- Inpatient skilled nursing facility Medicare claims.
A. Inpatient Medicare claims submitted by all hospitals.
Which of the following is associated with the Medicare fee schedule?
- APCs
- MS-DRGs
- RBRVS
- RUG-III
C. RBRVS
To assign SNF residents to the appropriate resource utilization group data are collected using the _____.
- MDS
- HEDIS
- RUG-III
- UHDDS
A. MDS
SNFs complete MDS assessments _____.
- On admission and once every 14 days.
- Once every 30 days up to 180 days.
- According to a schedule designed for Medicare payment.
- Depending on the diagnosis of the patient.
C. According to a schedule designed for Medicare payment.
In processing a Medicare payment for outpatient radiology exams a hospital outpatient services department would receive payment under which of the following?
- DRGs
- HHRGS
- OASIS
- OPPS
D. OPPS
Which of the following is not reimbursed according to the Medicare outpatient prospective payment system?
- CMHC Partial Hospitalization Services
- Critical Access Hospitals
- Hospital Outpatient Departments
- Vaccines Provided by CORF's
B. Critical Access Hospitals
Fee schedules are updated by third-party payers _____.
- Annually
- Monthly
- Semiannually
- Weekly
A. Annually
Which of the following would a health record technician use to perform the billing function for a physician's office?
- CMS-1500
- UB-04
- UB-92
- CMS 1450
A. CMS-1500
When a provider accepts assignment this means that the _____.
- Patient authorizes payment to be made directly to the provider.
- Provider accepts as payment in full whatever the payer reimburses.
- Balance filling is allowed on patient accounts, but at a limited rate.
- Participating provider receives a fee-for-service reimbursement.
B. Provider accepts as payment in full whatever the payer reimburses.
A coding audit shows that an inpatient coder is using multiple codes that describe the individual components of a procedure rather than using a single code that describes all the steps of the procedure performed. Which of the following should be done in this case?
- Require all coders to implement this practice.
- Report the practice to the OIG.
- Counsel the coder and stop the practice immediately.
- Put the coder on unpaid leave of absence.
C. Counsel the coder and stop the practice immediately.
A health information technician is hired as the chief compliance officer for a large group practice. In evaluating the current program, the HIT learns that there are written standards of conduct and policies and procedures that address specific areas of potential fraud as well as audits in place to monitor compliance. Which of the following should the compliance officer also ensure are in place?
- Compliance program education and training programs for all employees in the organization.
- Establishment of a hotline to receive complaints and adoption of procedures to protect whistle blowers from retaliation.
- Adopt procedures to adequately identify individuals who make complaints so that appropriate follow-up can be conducted.
- Establish a corporate compliance committee who report directly to the CFO.
B. Establishment of a hotline to receive complaints and adoption of procedures to protect whistle blowers from retaliation.
In developing a coding compliance program, which of the following would not be ordinarily included as participants in coding compliance education?
- Current Coding Personnel
- Medical Staff
- Newly Hired Coding Personnel
- Nursing Staff
D. Nursing Staff
The national Correct Coding Initiative (NCCI) was developed to control improper coding leading to inappropriate payment for:
- Part A Medicare Claims
- Part B Medicare Claims
- Medicaid Claims
- Medicare and Medicaid Claims
B. Part B Medicare Claims
When the CCI editor flags that a comprehensive code and a component code are billed together for the same beneficiary on the same date of service, Medicare will pay for:
- The component code but not the comprehensive code.
- The comprehensive code but not the component code.
- The comprehensive code and the component codes.
- Neither the comprehensive code nor the component code.
B. The comprehensive code but not the component code.
CCI edit files contain code pairs called mutually exclusive edits which prevent payment for _____.
- Services that cannot reasonably be billed together.
- Services that are components of a more comprehensive procedure.
- Unnecessary procedures.
- Comprehensive procedures.
A. Services that cannot reasonably be billed together.
Which of the following issues compliance program guidance?
- AHIMA
- CMS
- Federal Registrar
- HHS Office of the Inspector General
D. HHS Office of the Inspector General
The coordination of benefits transaction (COB) is important so that _____.
- There is no duplication of benefits paid.
- The hospital receives the full amount of billed services.
- The provider receives the full amount of billed services.
- The patient receives the correct bill.
A. There is no duplication of benefits paid.
Which of the following is a written description of an organizations; formal position?
- Hierarchy Chart
- Organizational Chart
- Policy
- Procedure
C. Policy
Community Hospital is launching a clinical documentation improvement (CDI) initiative because currently clinical documentation does not always adequately reflect the severity of illness of the patient and does not support optimal HIM coding quality and accuracy. Given this situation, which of the following would be the best action to provide improved documentation for patient care and coding.
- Hire clinical documentation specialists to review records prior to coding.
- Ask coders to query physicians more often.
- Provide physicians the opportunity to add addenda to their reports to clarify documentation issues.
- Conduct qualitative analyses of inpatient records while the patient is hospitalized to identify opportunities to improve the documentation in the record.
D. Conduct qualitative analyses of inpatient records while the patient is hospitalized to identify opportunities to improve the documentation in the record.
A coder notes that the patient is taking prescribed Haldol. The final diagnoses on the progress notes include diabetes mellitus, acute pharyngitis, and malnutrition. What condition might the coder suspect the patient has and should query the physician?
- Insomnia
- Hypertension
- Mental or Behavior Problems
- Rheumatoid Arthritis
C. Mental or Behavior Problems
In conducting a qualitative analysis to ensure that documentation in the health record supports the diagnosis of the patient, what documentation would a doctor look for to substantiate the diagnosis of aspiration pneumonia?
- Diffuse parenchymal lung disease on x-ray.
- Patient has history of inhaled food, liquid, or oil.
- Positive culture for Pneumocystis carinii.
- Positive culture for Streptococcus pneumoniae.
B. Patient has history of inhaled food, liquid, or oil.
The HIM department is planning to scan non-electronic medical record documentation. The project includes the scanning of health record documentation such as history and physicals, physicians orders, operative reports, and nursing notes. Which of the following methods of scanning would be best to help HIM professionals monitor the completeness of health records during a patient's hospitalization?
- Ad Hoc
- Concurrent
- Retrospective
- Post-Discharge
B. Concurrent
The HIM department is planning to scan non-electronic medical record documentation. The project includes the scanning of health record documentation such as history and physicals, physicians orders, operative reports, and nursing notes will be scanned. Which of the following methods of scanning would be best so that critical patient health information is available electronically at the patient's bedside or in the physician portal?
- Ad Hoc
- Concurrent
- Retrospective
- Post-Discharge
B. Concurrent
The HIM department is planning to scan non-electronic medical record documentation. The project will include scanning of documents at the point of admission such as consents, drivers' licenses, and insurance cards, The project also includes that scanning of health record documentation such as history and physicals, physicians orders, operative reports, and nursing notes will be scanned. Which of the following methods of scanning would be most efficient to make intake documents such as consents, drivers' licenses, and insurance cards immediately available to the hospital's billing department?
- Centralized
- Concurrent
- Hybrid
- Post-Discharge
B. Concurrent
The HIM department is planning to scan non-electronic medical record documentation. The project will include scanning of documents at the point of admission such as consents, drivers' licenses, and insurance cards, The project also includes that scanning of health record documentation such as history and physicals, physicians orders, operative reports, and nursing notes will be scanned. Which of the following methods of scanning would be the simplest to implement?
- Ad Hoc
- Concurrent
- Decentralized
- Post-Discharge
D. Post-Discharge
In conducting a qualitative review, the clinical documentation specialist sees that the nursing staff has documented the patient's skin integrity on admission to support the presence of a stage I pressure ulcer. However, the physician's documentation is unclear as to whether this condition was present on admission. How should the clinical documentation specialist proceed?
- Note the condition as present on admission.
- Query the physician to determine if the condition was present on admission.
- Note the condition as unknown on admission.
- Note the condition as not present on admission.
B. Query the physician to determine if the condition was present on admission.
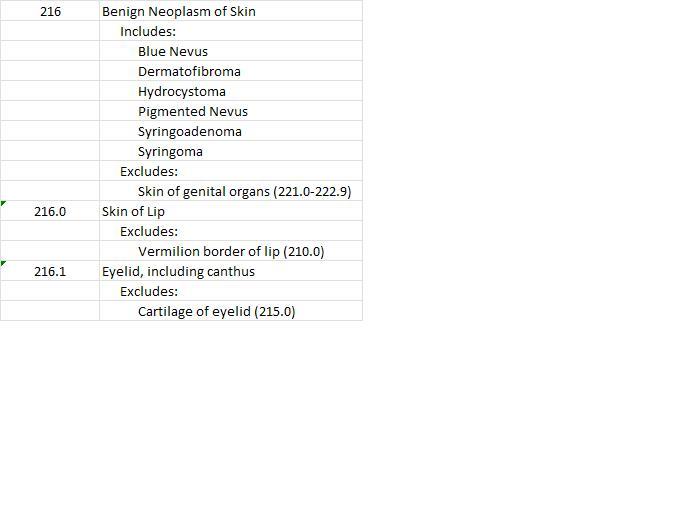
When coding a hydrocystoma of the eyelid, which of the following codes should be used?
- 216
- 210.0
- 215.0
- 216.1
D. 216.1
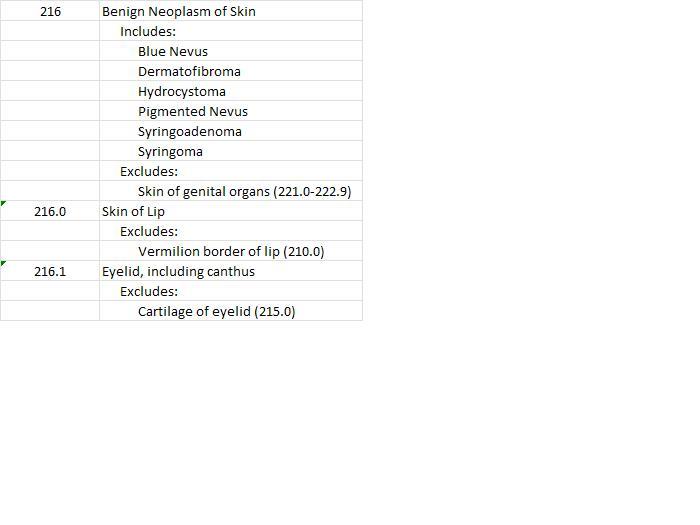
When coding a benign neoplasm of skin of the vermilion border of the lip, which of the following codes should be used?
- 216
- 210.0
- 216.0
- 216.1
B. 210.0
If a patient has an excision of a malignant lesion of the skin, the CPT code is determined by the body area from which the excision occurs and which of the following?
- Length of the lesion as described in the pathology report.
- Dimension of the specimen submitted as described in the pathology report.
- Width times the length of the lesion as described in the pathology report.
- Diameter of the lesion as well as the margins excised as described in the operative report.
D. Diameter of the lesion as well as the margins excised as described in the operative report.
According to CPT, a repair of a laceration that includes retention sutures would be considered what type of closure?
- Complex
- Intermediate
- Not Specified
- Simple
A. Complex
The patient was admitted with nausea, vomiting, and abdominal pain. The physician documents the following on the discharge summary: acute cholecystitis, nausea, vomiting, and abdominal pain. Which of the following would be the correct coding and sequencing for this case?
- Acute cholecystitis, nausea, vomiting, and abdominal pain.
- Abdominal pain, vomiting, nausea, acute cholecystitis.
- Nausea, vomiting, and abdominal pain.
- Acute cholecystitis.
D. Acute cholecystitis.
A patient is admitted with spotting. She had been treated two weeks previously for a miscarriage with sepsis. The sepsis had resolved and she is afebrile at this time. She is treated with an aspiration dilation and curettage. Products of conception are found. Which of the following should be the principal diagnosis?
- Miscarriage
- Complications of spontaneous abortion with sepsis
- Sepsis
- Spontaneous abortion with sepsis
A. Miscarriage
An 80-year-old female is admitted with fever, lethargy, hypotension, tachycardia, oliguria, and elevated WBC. The patient has more than 100,000 organisms of Escherichia coli per cc of urine. The attending physician documents "urosepsis." How should the coder proceed to code this case?
- Code sepsis as the principal diagnosis with urinary tract infection due to E coli as secondary diagnosis.
- Code urinary tract infection with sepsis as the principal diagnosis.
- Query the physician to ask if the patient has septicemia because of the symptomology.
- Query the physician to ask if the patient had septic shock so that this may be used as the principal diagnosis.
C. Query the physician to ask if the patient has septicemia because of the symptomology.
A 65-year-old patient, with a history of lung cancer, is admitted to a healthcare facility with ataxia and syncope and a fractured arm as a result of falling. The patient undergoes a closed reduction of the fracture in the emergency department and undergoes a complete workup for metastatic carcinoma of the brain. The patient is found to have metastatic carcinoma of the lung to the brain and undergoes radiation therapy to the brain. Which of the following would be the principal diagnosis in this case?
- Ataxia
- Fractured Arm
- Metastatic Carcinoma of the Brain
- Carcinoma of the Lung
C. Metastatic Carcinoma of the Brain
A patient was admitted for abdominal pain with diarrhea and was diagnosed with infectious gastroenteritis. The patient also had angina and chronic obstructive pulmonary disease. Which of the following would be the correct coding and sequencing for this case?
- Abdominal pain; infectious gastroenteritis; chronic obstructive pulmonary disease; angina.
- Infectious gastroenteritis; chronic obstructive pulmonary disease; angina.
- Gastroenteritis; abdominal pain; angina.
- Gastroenteritis; abdominal pain; diarrhea; chronic obstructive pulmonary disease; angina.
B. Infectious gastroenteritis; chronic obstructive pulmonary disease; angina.
A patient is admitted with a history of prostate cancer and with mental confusion. The patient completed radiation therapy for prostatic carcinoma three years ago and is status post a radical resection of the prostate. A CT scan of the brain during the current admission reveals metastatic. Which of the following is the correct coding and sequencing for the current hospital stay?
- Metastatic carcinoma of the brain; carcinoma of the prostrate; mental confusion.
- Mental confusion; history of carcinoma of the prostate; admission for chemotherapy.
- Metastatic carcinoma of the brain; history of carcinoma of the prostate.
- Carcinoma of the prostate; metastatic carcinoma to the brain.
C. Metastatic carcinoma of the brain; history of carcinoma of the prostate.
A patient is admitted with abdominal pain. The physician states that the discharge diagnosis is pancreatitis versus noncalculus cholecystitis. Both diagnoses are equally treated. The correct coding and sequencing for this case would be:
- Sequence either the pancreatitis or the noncalculus cholecystitis as principal diagnosis.
- Pancreatitis; noncalculus cholecystitis; abdominal pain.
- Noncalculus cholecystitis; pancreatitis; abdominal pain.
- Abdominal pain; pancreatitis; noncalculus cholecystitis.
A. Sequence either the pancreatitis or the noncalculus cholecystitis as principal diagnosis.
According to the UHDDS, which of the following is the definition of "other diagnoses"?
- Is recorded in the patient record.
- Is documented by the attending physician.
- Receives clinical evaluation or therapeutic treatment or diagnostic procedures or extends the length of stay or increases nursing care and/or monitoring.
- Is documented by at least two physicians and/or the nursing staff.
C. Receives clinical evaluation or therapeutic treatment or diagnostic procedures or extends the length of stay or increases nursing care and/or monitoring.
A 7-year-old patient was admitted to the emergency department for treatment of shortness of breath. The patient is given epinephrine and nebulizer treatments. The shortness of breath and wheezing are unabated following treatment. What diagnosis should be suspected?
- Acute bronchitis
- Acute bronchitis with chronic obstructive pulmonary disease
- Asthma with status asthmaticus
- Chronic obstructive asthma
C. Asthma with status asthmaticus
A coder might find which of the following on a patient's problem list if the medication list contains the drug Protonix?
- High blood pressure
- Esophagitis
- Congestive heart failure
- AIDS
B. Esophagitis
A physician orders a chest x-ray for a patient who presents with fever, productive cough, and shortness of breath. The physician indicates in the progress notes:
"Rule out pneumonia."
What should the coder report for the visit when the results have not yet been received?
- Pneumonia
- Fever, cough, shortness of breath
- Cough, shortness of breath
- Pneumonia, cough, shortness of breath, fever
B. Fever, cough, shortness of breath
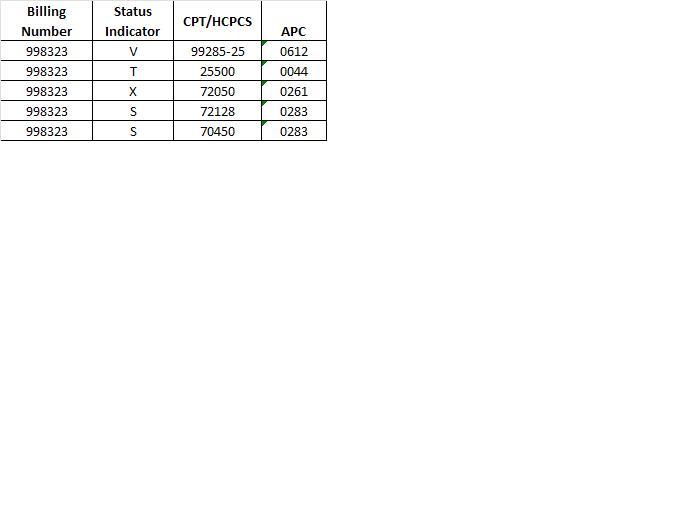
If another Status T procedure were performed, how much would the facility receive for the second Status T procedure?
- 0%
- 50%
- 75%
- 100%
B. 50%
Using a hospital discharge database, a physician does a study of diabetes mellitus comparing age of onset with response to a specific drug regimen. The physician has gathered _____ from the database.
- Data Elements
- Information
- Information Standards
- Data Sets
B. Information
Two clerks are abstracting data for the same case for a registry. When their work is checked, discrepancies are found. Which data quality component is lacking.
- Completeness
- Validity
- Reliability
- Timeliness
C. Reliability
Which of the following terms refers to the incidence of death?
- Classification
- Morbidity
- Mortality
- Vital Statistics
C. Mortality
Review of the disease indexes, pathology reports, and radiation therapy reports is part of which function in the cancer registry?
- Case Definition
- Case-Finding
- Follow-Up
- Reporting
B. Case-Finding
Cancer registries receive approval as a part of the facility cancer program from which of the following agencies?
- American Cancer Society
- National Cancer Registrar's Association
- National Cancer Institute
- American College of Surgeons
D. American College of Surgeons
Which of the following is a database from the National Health Care Survey that uses the patient health record as a data source?
- National Health Provider Inventory
- National Ambulatory Medical Care Survey
- National Employer Health Insurance Survey
- National Infectious Disease Inventory
B. National Ambulatory Medical Care Survey
Which of the following contains a list maintained in diagnosis code number order of patients discharged from a facility during a particular time period?
- Physician Index
- Master Patient Index
- Disease Index
- Operation Index
C. Disease Index
Which of the following contains a list maintained in a procedure code number order of patients discharged from a facility during a particular time period?
- Physician Index
- Master Patient Index
- Disease Index
- Operation Index
D. Operation Index
Case finding is a method used to _____.
- Identify patients who have been seen or treated in a facility for a particular disease or condition for inclusion in a registry.
- Define which cases are to be included in a registry.
- Identify trends and changes in the incidence of disease.
- Identify facility-based trends.
A. Identify patients who have been seen or treated in a facility for a particular disease or condition for inclusion in a registry.
In a cancer registry, the accession number _____.
- Identifies all the cases of cancer treated in a given year.
- Is the number assigned to each case as it is entered into a cancer registry.
- Identifies the pathologic diagnosis of an individual cancer.
- Is the number assigned for the diagnosis of a cancer patient entered into the cancer registry.
B. Is the number assigned to each case as it is entered into a cancer registry.
A population-based registry _____.
- Includes information from more than one facility in a particular geopolitical area, such as a state or region.
- Includes only cases for a particular facility such as a hospital or clinic.
- Represents a computerized system that was developed for a particular facility.
- Provides data for comparisons in several rates and quality of life for patients with different treatments and at different stages of cancer.
A. Includes information from more than one facility in a particular geopolitical area, such as a state or region.
Vital statistics include data on _____.
- Research projects on which new treatments and tests are investigated to determine whether the are safe and effective.
- Births, deaths, fetal deaths, marriages, and divorces.
- Medicare claims.
- ICD diagnoses codes.
B. Births, deaths, fetal deaths, marriages, and divorces.
The most prevalent trend in the collection of secondary databases is _____.
- Increased use of encryption technology.
- Increased use of encoders.
- Increased use of automated data entry.
- Widespread implementation of electronic medical records.
C. Increased use of automated data entry.
A record is considered a primary data source when it _____.
- Contains information about the patient that has been documented by the professionals who provided care to the patient.
- Contains data abstracted from a patient record.
- Includes data stored in a computer system.
- Contains data that are entered into a disease-oriented database.
A. Contains information about the patient that has been documented by the professionals who provided care to the patient.
The following data were derived from a comparative discharge database for hip and femur procedures. These data can best be described as:
- Aggregate Data
- Identifiable Data
- Patient Specific Data
- Primary Data
A. Aggregate Data
Suppose there are six males in a class of 20 students. What term could be used to describe the comparison?
- Ratio
- Percentage
- Proportion
- Rate
C. Proportion
In a frequency distribution, the lowest value is 5 and the highest value is 20. What is the range?
- 5 to 20
- 15
- 7.5
- 20 to 5
B. 15
What is the mean for the following frequency distribution:10, 15, 20, 25, 25?
- 47.5
- 20
- 19
- 95
C. 19
What is the mode for the frequency distribution 10, 15, 20, 25, 25?
- 47.5
- 20
- 19
- 95
D. 25
Suppose that five patients stayed in the hospital for a total of 27 days. Which term would be used to describe the result of the calculation 27 divided by 5?
- Average Length of Stay
- Total Length of Stay
- Patient Length of Stay
- Average Patient Census
A. Average Length of Stay
Which of the following statements best describes the difference between a hospital inpatient and a hospital outpatient?
- Outpatients are treated in the emergency department; inpatients receive services in the regular clinical departments of the hospital.
- Inpatients always stay in the hospital overnight; outpatients never do.
- Inpatients receive room, board, and continuous nursing services in areas of the hospital where patients generally stay overnight; outpatients receive ambulatory diagnostic and therapeutic services.
- Outpatients primarily receive diagnostic services; inpatients receive mostly therapeutic services.
C. Inpatients receive room, board, and continuous nursing services in areas of the hospital where patients generally stay overnight; outpatients receive ambulatory diagnostic and therapeutic services.
Given the numbers 47, 20, 11, 33, 30, 30, 35, and 50, what is the mean?
- 30
- 32
- 32.5
- 35
B. 32
Given the numbers 47, 20, 11, 33, 30, 30, 35, and 50, what is the mode?
- 30
- 32
- 32.5
- 35
A. 30
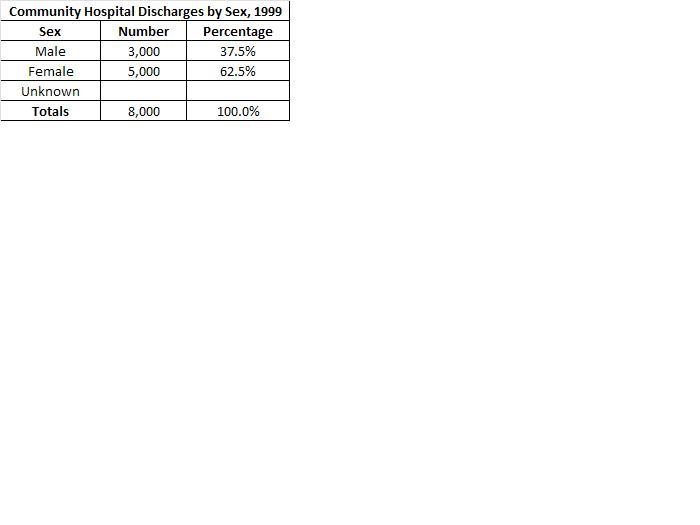
What is (are) the format problems with the following table?
- Title is missing
- Variable names are missing
- There are blank cells
- Row totals are inaccurate
C. There are blank cells
Mr. Jones was admitted to the hospital on March 21 and discharged on April 1. What was the length of stay of Mr. Jones?
- 5 days
- 10 days
- 11 days
- 15 days
C. 11 days
Community Hospital discharged nine patients on April 1. The length of stay for each of the patients was as follows: for patient A; 1 day; for patient B; 5 days; for patient C; 3 days; for patient D; 3 days; for patient E; 8 days; for patient F; 8 days; for patient G; 8 days; for patient H; 9 days; for patient I; 9 days. What was the median length of stay?
- 5 days
- 6 days
- 8 days
- 9 days
C. 8 days
Community Hospital had 25 inpatient deaths, including newborns, for the month of June. The hospital performed five autopsies for the same period. What was the gross autopsy rate for the hospital for June?
- 0.02%
- 5%
- 20%
- 200%
C. 20%
Which national database includes data on all discharged patients regardless of payer?
- Healthcare Cost and Utilization Project
- Medicare Provider Analysis and Review File
- Unified Medical Language System
- Uniform Hospital Discharge Data Set
A. Healthcare Cost and Utilization Project
Look into this more
Which of the following is made up of claims data from Medicare claims submitted by acute care hospitals and skilled nursing facilities?
- NPDB
- MEDPAR
- HIPDB
- UHDDS
B. MEDPAR
The Medicare Provider Analysis and Review file is made up of _____.
- Medical malpractice payments and sanctions taken against providers.
- Data collected from a sample of office-based physicians.
- Medicare claims from acute care hospitals and skilled nursing facilities.
- Data collected on births and deaths.
C. Medicare claims from acute care hospitals and skilled nursing facilities.
The collection of information on healthcare fraud and abuse was mandated by HIPAA and resulted in the development of _____.
- National Practitioner Data Bank
- Healthcare Integrity and Protection Data Bank
- National Health Provider Inventory
- Nationwide False Claims Data Bank
B. Healthcare Integrity and Protection Data Bank
The Healthcare Cost and Utilization Project is a major initiative of which organization within the federal government?
- Agency for Healthcare Research and Quality (AHRQ)
- Food and Drug Administration (FDA)
- National Center for Healthcare Statistics (NCHS)
- Centers for Medicare and Medicaid Services (CMS)
A. Agency for Healthcare Research and Quality (AHRQ)
If you are interested in displaying the parts of a whole in graphic form, what graphic technique would you use?
- Table
- Histogram
- Line Chart
- Pie Chart
D. Pie Chart
Which rate describes the number of new cases of an illness for a specific time period?
- Mortality Rate
- Incidence Rate
- Morbidity Rate
- Prevalence Rate
B. Incidence Rate
Which term is used to describe the number of inpatients present at the census-taking time each day pus the number of inpatients who were both admitted and discharged after the census-taking time the previous day?
- Inpatient Bed Occupancy Rate
- Bed Count
- Average Daily Census
- Daily Inpatient Census
D. Daily Inpatient Census
Which unit of measure is used to indicate the services received by one inpatient in a 24-hour period?
- Inpatient Service Day
- Volume of Services
- Average Occupancy Charges
- Length of Stay
A. Inpatient Service Day
Which rate is used to compare the number of inpatient deaths to the total number of inpatient deaths and discharges?
- Net Hospital Death Rate
- Fetal/Newborn/Maternal Hospital Death Rate
- Gross Hospital Death Rate
- Adjusted Hospital Death Rate
C. Gross Hospital Death Rate
Which rate is used to compare the number of calendar days that a patient is hospitalized?
- Average Length of Stay
- Length of Stay
- Occupancy Rate
- Level of Service
B. Length of Stay
Which rate compares the number of autopsies performed on hospital inpatients to the total number of inpatient deaths for the same period of time?
- Net Autopsy Rate
- Gross Autopsy Rate
- Hospital Autopsy Rate
- Average Autopsy Rate
B. Gross Autopsy Rate
Which rate compares the number of autopsies performed on hospital inpatients to the total number of inpatient deaths minus unautopsied coroners' or medical examiners' cases for the same period of time?
- Net Autopsy Rate
- Gross Autopsy Rate
- Hospital Autopsy Rate
- Average Autopsy Rate
A. Net Autopsy Rate
What term is used for the number of calendar days of an inpatient hospitalization from admission to discharge?
- Average Daily Census
- Census
- Inpatient Service Day
- Length of Stay
D. Length of Stay
What term is used for the number of inpatients present at any one time in a healthcare facility?
- Average Daily Census
- Census
- Inpatient Service Day
- Length of Stay
B. Census
Several members of the hospital's quality performance improvement team arrive late for most team meetings. This practice hinders the efficiency of the team. Which of the following would be the best action to take to remedy the situation?
- Reprimand the offenders.
- Ignore the individuals who come late to meetings.
- Develop team ground rules for meeting attendance.
- Make sure that the individuals who come late are given extra teamwork.
C. Develop team ground rules for meeting attendance.
Look into further
What is the official count of inpatients taken at midnight called?
- Average Daily Census
- Census
- Daily Inpatient Census
- Inpatient Service Days
C. Daily Inpatient Census
What is the role of the case manager?
- Perform retrospective utilization reviews.
- Implement the prospective payment system for acute care.
- Coordinate medical care and ensure the necessity of the services provided to beneficiaries.
- Ensure that the hospital's resources are being used efficiently.
C. Coordinate medical care and ensure the necessity of the services provided to beneficiaries.
Which of the following is not a responsibility of a healthcare organization's quality management department?
- Helping departments to identify potential clinical quality problems.
- Participating in regular departmental meetings across the organization.
- Using medical peer review to identify patterns of care.
- Determining the method for studying potential problems.
C. Using medical peer review to identify patterns of care.
Which of the following statements best describes the purpose of universal precautions?
- Prevent exposure to disease-causing agents.
- Regulate direct patient care provided by nursing personnel.
- Ensure that hospital staff are properly qualified.
- Coordinate the hospital's quality management program.
A. Prevent exposure to disease-causing agents.
Which of the following statements best defines utilization management?
- It is the process of determining whether the medical care provided to a patient is necessary.
- It is a set of processes used to determine the appropriateness of medical services provided during specific episodes of care.
- It is a process that determines whether a planned service of a patient's condition warrants care in an inpatient setting.
- It is an ongoing infection surveillance program.
B. It is a set of processes used to determine the appropriateness of medical services provided during specific episodes of care.
Which of the following is NOT a type of utilization review?
- Preadmission Utilization Review
- Continued-Stay Utilization Review
- Discharge Utilization Review
- Documentation Utilization Review
D. Documentation Utilization Review
What role is not representative of the ombudsmen in patient advocacy?
- Judge
- Mediator
- Listener
- Partner
A. Judge
The process that involves ongoing surveillance and prevention of infection so as to ensure the quality and safety of healthcare for patients and employees is known as:
- Utilization Management
- Infection Control
- Risk Management
- Case Management
B. Infection Control
Every healthcare organization's risk management plan should include the following components:
- Reporting of claims, initial investigation of claims, protection of primary and secondary health records, negotiation of settlements, management of litigations, and use of information for claim's resolution in performance management activities.
- Safety management, security management, claims management, technology management, and facilities management.
- Objectives, key elements, responsibilities, methods, and areas of focus for the current year.
- Risk acceptance, risk avoidance, risk reduction or minimization, and risk transfer.
C. Objectives, key elements, responsibilities, methods, and areas of focus for the current year.
Which of the following is NOT one of the basic functions of the utilization review process?
- Case Management
- Discharge Planning
- Claims Management
- Utilization Review
C. Claims Management
A HIT professional who is following a process for abstracting information for a cancer registry would be engaging in what type of decision making?
- Long-Range
- Tactical
- Structured
- Unstructured
C. Structured
Total quality management and continuous quality improvement are well-known _____.
- Performance Improvement Models
- Quality Indicators
- Change Management Techniques
- Management Philosophies
A. Performance Improvement Models
Donabedian proposed three types of quality indicators: structure indicators, process indicators, and _____.
- Performance Indicators
- Management Indicators
- Outcome Indicators
- Ouput Indicators
C. Outcome Indicators
Many organizations and quality experts define quality as meeting or exceeding _____.
- Patient Quotas
- System Outputs
- Customer Expectations
- Data Collection
C. Customer Expectations
Teams generally go through the following stages as the develop: forming, _____, norming, and performing.
- Conforming
- Storming
- Informing
- Uniforming
B. Storming
The man credited with revitalizing the Japanese economy are World War II was _____.
- Brian Joiner
- Armand Feigenbaum
- Walter Shewart
- W. Edwards Deming
D. W. Edwards Deming
The individual whose principal responsibility is to facilitate the process of change is the _____.
- Change Manager
- Change Agent
- Change Supervisor
- Change Leader
B. Change Agent
Peter Senge believed that each individual within an organization must be committed to personal mastery and must always seek to _____.
- Change
- Improve
- Learn
- Solve Problems
C. Learn
The steps in Langley, Nolan, and Nolan's PDSA cycle are _____.
- Plan, Do, Simplify, Act
- Prepare, Do, Study, Act
- Plan, Do, Share, Act
- Plan, Do, Study, Act
D. Plan, Do, Study, Act
Brainstorming, affinity grouping, and nominal group techniques are tools and techniques used during performance improvement initiatives to facilitate _____.
- Communication
- Knowledge
- Quality Improvement
- Cooperation
A. Communication
Which of the following terms refers to the process of planning for change?
- Brainstorming
- Change Agent
- Change Management
- Performance Improvement
C. Change Management
Which of the following is a data collection tool that records and compiles observations or occurrences?
- Check Sheet
- Force-Field Analysis
- Pareto Chart
- Scatter Diagram
A. Check Sheet
According to the Pareto principle, _____.
- 20 percent of the sources of a problem are responsible for 80 percent of its actual effects.
- 80 percent of the sources of a problem are responsible for 20 percent of its effects.
- 20 percent of the sources of a problem are responsible for 20 percent of its effects.
- 80 percent of the sources of a problem are responsible for 100 percent of its effects.
A. 20 percent of the sources of a problem are responsible for 80 percent of its actual effects.
Change management is the process of planning for change. It concentrates on _____.
Addressing employee resistance to changes in processes, procedures, and policies.
Scheduling planned changes in processes, procedures, and policies.
Implementing the technology required to execute planned changes.
Managing the cost of implementing planned changes.
A. Addressing employee resistance to changes in processes, procedures, and policies.
Which of the following statements does not represent a fundamental principle of performance improvement?
- The structure of a system determines its performance.
- Systems are static and do not demonstrate variation.
- Improvements rely on the collection and analysis of data.
- Performance improvement requires the commitment and support of top administration.
B. Systems are static and do not demonstrate variation.
Which of the following should be the first step in any decision-making process?
- Analyzing the Problem
- Defining the Problem
- Developing Alternate Solutions
- Deciding on the Best Solution
B. Defining the Problem
Which of the following is used to plot the points for two variables that may be related to each other in some way?
- Force-Field Analysis
- Pareto Chart
- Root Cause Analysis
- Defining the Problem
D. Defining the Problem
The HIM analytics professional is reviewing a chart on nosocomial infections presented by the hospital's infection control committee. The committee is reporting that the decrease in infection rate has accelerated over the past ten years. What comments should the data analytics professional make?
- Concur with the conclusion of the committee.
- State that the greatest decrease in infection rate in a year took place in 2005.
- State that the greatest decrease in infection rate occurred in 1960 and 1970.
- Request a new data chart be presented that accurately reflects the trend of infection rate.
D. Request a new data chart be presented that accurately reflects the trend of infection rate.
Hospital A discharges 10,000 patients a year. Hospital B is located in the same town and discharges 5,000 patients per year. At a medical staff committee meeting a physician reports that he is concerned about the quality of care at Hospital A because Hospital A has double the number of deaths per year than Hospital B. The HIM director is attending the meeting in a staff position. Which of the following actions should the director take?
- Make no comment since this is a medical staff meeting.
- Agree with the physician that the data suggest a quality issue.
- Suggest that the data be adjusted for possible differences in type and volume of patients treated.
- Suggest that an audit be done immediately to determine the cause of deaths within the hospital.
C. Suggest that the data be adjusted for possible differences in type and volume of patients treated.
A flu epidemic has occurred in a small-sized town. This resulted in 200 visits to the emergency department of the local hospital. Of the 200 emergency patients, 80 were subsequently admitted, and of those, 20 died. Based on the data, the local paper is reporting that the mortality rate area wide from the flu epidemic is 10 percent. How should the HIM data analytics professional respond to this conclusion?
- Confirm that the percentage of deaths from the flu is correct.
- Argue that the true mortality rate from the flu should be based on the sicker patients and is really 25 percent.
- Maintain that the true mortality rate for the area is unknown.
- Write a letter to the editor advising the paper not to scare the public.
C. Maintain that the true mortality rate for the area is unknown.
The Medical Record Committee wants to determine if the hospital is in compliance with Joint Commission standards for medical record delinquency rates. The HIM director has compiled a report that shows that the records are delinquent for an average of 29 days after discharge. Given this information what can the Committee conclude?
- Delinquency rate is within Joint Commission standards.
- All physicians are performing at optimal levels.
- The chart deficiency process is working well.
- Data are insufficient to determine if the hospital is in compliance.
D. Data are insufficient to determine if the hospital is in compliance.
The coding supervisor has compiled a report on the number of coding errors made each day by the coding staff. The report data show that Tim makes as average of six errors per day; Jane makes and average of five errors per day, and Bob and Susan each make an average of two errors per day. What action should the coding supervisor take given this information?
- Counsel Tim and Jane because they have the highest error rates.
- Encourage Tim and Jane to get additional training.
- Provide Bob and Susan with incentive pay for low coding error rate.
- Take no action since not enough information is given to make a judgement.
D. Take no action since not enough information is given to make a judgement.

Community Hospital has compared its 2003 and 2008 admission type patient profile data. From a performance improvement standpoint, which admission types should the hospital examine for possible changes in capacity handling?
- Elective
- Emergency
- Newborn
- Urgent
B. Emergency
As part of the clinic's performance improvement program, a HIM director wants to implement benchmarking for the transcription division at a large physician clinic. The clinic has 21 transcriptionists who average about 140 lines an hour. The transcription unit supports 80 physicians at a cost of 15 cents per line. What should be the first step that the supervisor takes to establish benchmarks for the transcription division?
- Clearly define what is to be studied and accomplished by instituting benchmarks.
- Hold a meeting with the transcriptionists to announce the benchmark program.
- Obtain other benchmarks from other institutions.
- Hire a consultant to assist with the process.
A. Clearly define what is to be studied and accomplished by instituting benchmarks.
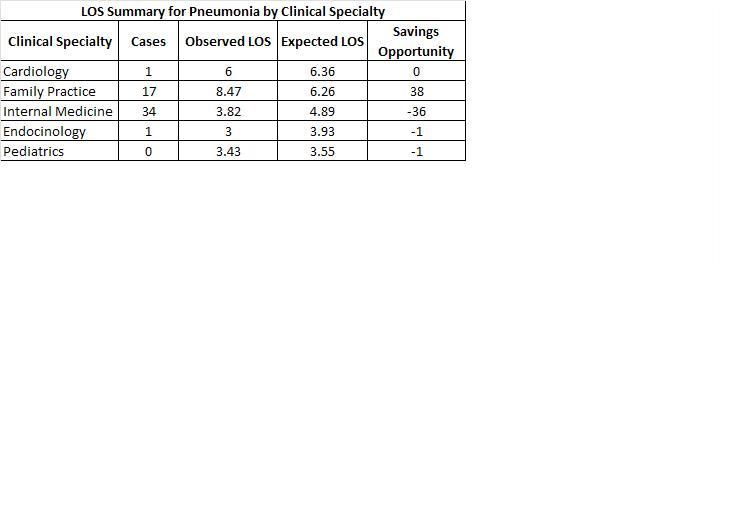
The following table compares Community Hospital's pneumonia length of stay (observed LOS) to the pneumonia length of similar hospitals (expected LOS). Given this data where might Community Hospital want to focus attention on its pneumonia LOS?
- Cardiology
- Endocrinology
- Family Practice
- Internal Medicine
C. Family Practice
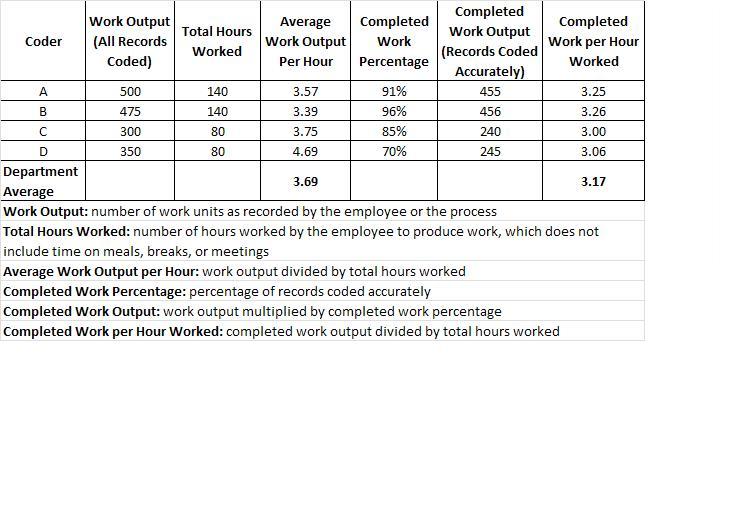
The following data has been collected about the HIM department's coding productivity as part of the organization's total quality improvement program. Which of the following is the best assessment of this data?
- Part-time coders are more productive than full-time coders.
- Full-time coders are more productive than part-time coders.
- All coders produce more than the departmental average.
- Part-time coders exceed the departmental average.
B. Full-time coders are more productive than part-time coders.
Which one of the following is the largest healthcare standards-setting body in the world?
- Agency for healthcare Research and Quality
- National Guideline Clearinghouse
- National Committee for Quality Assurance
- Joint Commission
D. Joint Commission
Patient care managers use the data documented in the health record to:
- Evaluate the performance of individual patient care providers.
- Communicate vital information among departments and across disciplines and settings.
- Generate patient bills and/or third-party payer claims for reimbursement.
- Determine the extent and effects of occupational hazards.
A. Evaluate the performance of individual patient care providers.
Which of the following use data from the MDS for Long-term Care?
- Centers for Medicare and Medicaid Services (CMS)
- Home Health Hospice Agencies
- Home Health Agencies
- Rehabilitation Facilities
A. Centers for Medicare and Medicaid Services (CMS)
What is the name of the federally funded program that pays the medical bills of the spouses and dependents of the persons on active duty in the uniformed services?
- HHS-CMS
- TRICARE
- CHAMPVA
- Medigap
B. TRICARE
The primary goal of the Hospital Standardization Program established in 1918 by the American College of Surgeons was to _____.
- Raise the standards of surgical practice.
- Train physicians and nurses for American hospitals.
- Standardize the educational curricula of American medical schools.
- Force substandard hospitals to close.
A. Raise the standards of surgical practice.
Which accrediting organization has instituted continuous improvement and sentinel event monitoring and use tracer methodology during survey visits?
- Accreditation Association for Ambulatory Healthcare
- Commission on Accreditation of Rehabilitation Facilities
- American Osteopathic Association
- Joint Commission
D. Joint Commission
Which of the following groups is the primary accreditation organization for facilities that treat individuals who have functional disabilities?
- American Osteopathic Organization
- Commission on Accreditation of Rehabilitation Facilities
- Accreditation Association for Ambulatory Health Care
- Joint Commission
B. Commission on Accreditation of Rehabilitation Facilities
What is the general name for Medicare standards impacting healthcare organizations?
- Conditions of Participation
- Regulations for Licensure
- Requirements for Service
- Terms of Accreditation
A. Conditions of Participation
Specific performance expectations and/or structures and processes that provide detailed information for each of the Joint Commission standards are called _____.
- Elements of Performance
- Fact Sheets
- Ad Hoc Reports
- Registers
A. Elements of Performance
The creation of the National Practitioner Data Bank was mandated by the _____.
- Social Security Act
- Privacy Act
- Health Insurance Portability and Accountability Act (HIPAA)
- Health Care Quality Improvement Act
D. Health Care Quality Improvement Act
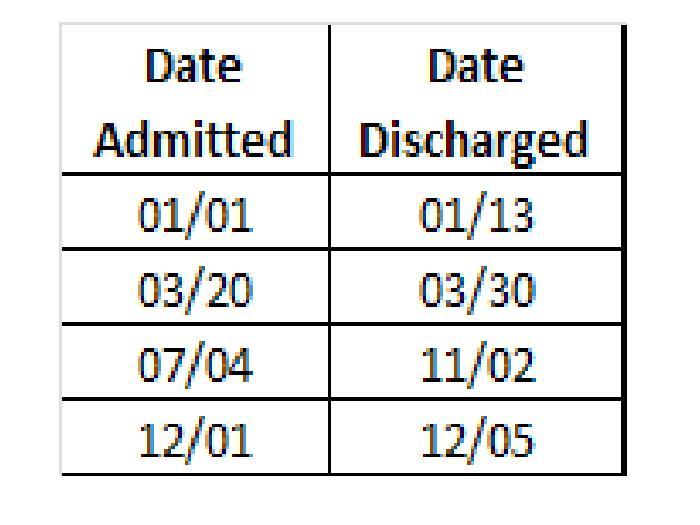
Mr. Jones is a 67-year-old patient who only has Medicare's Part A insurance. Given the information here, if Mr. Jones used 36 lifetime reserve days, how many does the patient have left to be used at a later date?
- 24 days
- 50 days
- 60 days
- 90 days
A. 24 days
Under outpatient prospective payment system, Medicare decides how much a hospital or a community mental health center will be reimbursed for each service rendered. Depending on the service, the patient pays either a coinsurance amount (20 percent) or a fixed copayment amount, whichever is less. Mr. Smith, who has paid his deductible for the year, was charged $85 for a minor procedure performed in the hospital outpatient department. The fixed copayment amount for this type of procedure, adjusted for wages in the geographic area, is $15. What would Mr. Smith need to pay in this case?
- $15
- $17
- $68
- $85
A. $15
The number of days Medicare will cover SNF inpatient care is limited to which of the following?
- 21
- 60
- 30
- 100
D. 100
Which of the following types of care is not covered by Medicare?
- Long-Term Nursing Care
- Skilled Nursing Care
- Hospice Care
- Home Healthcare
A. Long-Term Nursing Care
How many benefit periods are covered by hospital insurance during a Medicare beneficiary's lifetime?
- One per year
- Based on a 90-day stay
- None
- Unlimited
D. Unlimited
What is the name of the program funded by the federal government to provide medical care to people on public assistance?
- CHAMPUS
- Medicare
- Medicaid
- Medigap
C. Medicaid
Some services are covered and paid by Medicare before Medicaid makes payments because Medicaid is considered which of the following?
- Qualified Beneficiary
- Premium Payer
- Payer of Last Resort
- Alternative Payer
C. Payer of Last Resort
Which of the following groups of healthcare providers contracts with an employer to provide healthcare services?
- Preferred Provider Organization (PPO)
- Health Maintenance Organization (HMO)
- Point-of-Service (POS) Provider
- Independent Practice Association
A. Preferred Provider Organization (PPO)
Which of the following reimbursement methods pays providers according to charges that are calculated before healthcare services are rendered?
- Fee-for-service reimbursement method
- Prospective payment method
- Retrospective payment method
- Resource-based payment method
B. Prospective payment method
Which of the following payment methods reimburses healthcare providers in the form of lump sums for all healthcare services delivered to a patient for a specific illness?
- Managed Fee-For-Service
- Captation
- Episode of Care
- Point of Service
C. Episode of Care
Which of the following apply to radiological and other procedures that include professional and technical components and are paid as a lump sum to be divided between physician and healthcare facility?
- Global Payments
- Professional Payment
- Bundled Payment
- Fee-For-Service
A. Global Payments
Prospective payment systems were developed by the federal government to:
- Increase healthcare access
- Manage Medicare and Medicaid Costs
- Implement Managed Care Programs
- Eliminate Fee-For-Service Programs
B. Manage Medicare and Medicaid Costs
Private health insurance is a type of _____ insurance.
- Commercial
- Federal
- Military
- State
A. Commercial
Health insurance plans where providers give healthcare services to members of the plan at a discounted rate are called _____ plans.
- ASO
- Medigap
- POS
- PPO
D. PPO
Which of the following encourages subscribers to select providers from a prescribed network but also allow them to seek healthcare services from providers outside the network at a higher level of copay?
- ASO
- POS
- PPO
- TRICARE
B. POS
Title XVIII of the Social Security Act Amendment of 1965 is also known as:
- Medicare
- Medicaid
- Medigap
- SCHIP
A. Medicare
Which of the following establish eligibility standards for enrollment in Medicaid?
- Centers for Medicare and Medicaid Services (CMS)
- Department of Health and Human Services (HHS)
- Federal Government
- Individual States
D. Individual States
This program provides additional federal funds to states so that Medicaid eligibility can be expanded to include a greater number of children.
- Medigap
- PACE
- SCHIP
- TRICARE
C. SCHIP
Active armed services members and their qualified family members are covered by which of the following healthcare providers?
- Medicaid
- Medicare
- PACE
- TRICARE
D. TRICARE
Dependents and survivors of permanently and totally disabled veterans are covered by which of the following healthcare programs?
- CHAMPUS
- CHAMPVA
- IHS
- TRICARE
B. CHAMPVA
Which of the following agencies is responsible for providing healthcare services to American Indians and Alaskan natives?
- CMS
- IHS
- NIH
- VA
B. IHS
Which of the following insurance covers healthcare costs and lost income associated with work-related injuries?
- CHAMPVA
- Medicare
- Medicaid
- Workers' Compensation
D. Workers' Compensation
A Medicare benefit period is defined as _____.
- Beginning the day the Medicare patient is admitted to the hospital and ending when the patient has not been hospitalized for a period of sixty consecutive days.
- The period in which a Medicare patient is hospitalized.
- The period that begins on January 1 of each year with an allowable inpatient hospitalization benefit of up to 90 days.
- Between 1 and 90 days of a Medicare patient's hospitalization.
A. Beginning the day the Medicare patient is admitted to the hospital and ending when the patient has not been hospitalized for a period of sixty consecutive days.
Which of the following is an external user of data?
- Public Health Department
- Medical Staff
- Hospital Administrator
- Director of the Clinical Laboratory
A. Public Health Department
Which of the following is the best definition of ambulatory surgery?
- Any surgical procedure that is done in an emergency department.
- Any surgical procedure that does not require an overnight stay in the hospital.
- Any surgical procedure that is done on a patient who is brought to the hospital in as ambulance.
- Any surgical procedure that is performed in a surgicenter.
B. Any surgical procedure that does not require an overnight stay in the hospital.
Which of the following dictates how the medical staff operates?
- Medical Staff Classification
- Medical Staff Bylaws
- Medical Staff Credentialing
- Medical Staff Committees
B. Medical Staff Bylaws
Who is responsible for implementing the policies and strategic direction of the hospital or healthcare organization and for building and effective executive management team?
- Board of Directors
- Chief Executive Officer
- Chief Information Officer
- Chief of Staff
B. Chief Executive Officer
What was the main result of the publication of the Flexner report?
- Medical school standards were established.
- Nursing school standards were established.
- Hospital standards were established.
- Health information management standards were established.
A. Medical school standards were established.
_____ govern(s) the operation of a hospital medical staff.
- Medical Staff Classification
- Medical Staff Bylaws
- Medical Staff Credentialing
- Medical Staff Committees
B. Medical Staff Bylaws
Which of the following bears the ultimate responsibility for the quality of care in a hospital?
- CEO
- Board of Directors
- Medical Staff
- Medical Director
B. Board of Directors
Ultimate responsibility for the operation of healthcare organizations lies with _____.
- Senior Management
- The Board of Directors
- All Employees
- Supervisory Managers
B. The Board of Directors
HIM professionals have been working with a multidisciplinary committee to identify the best solution that will allow hospital physicians coordinated access to all forms of incoming and outgoing messages including voice, fax, e-mail, and video mail. Currently physicians have to log in to various systems, using different IDs and passwords to retrieve all their messages, reducing effectiveness and efficiency. Which of the following would provide the best solution to the current problem?
- Computer-Telephone Integration (CTI)
- Kiosk
- IP Telephony
- Unified Messaging
D. Unified Messaging
Which of the following statements is true of decision making in an organization?
- Decision makers at all levels of the organization routinely make structured decisions.
- All decision makers make the same types of decisions.
- All decisions require periodic reports.
- Decisions makers at different levels of the organization have different information needs,
D. Decisions makers at different levels of the organization have different information needs,
Why was the American Medical Association established?
- To represent the interests of physicians across the country.
- To standardize the curriculum for U.S. medical schools.
- to develop state licensure systems.
- To close most of the existing medical schools to address the problem of oversupply.
A. To represent the interests of physicians across the country.
The VA hospital system was established to provide hospital, nursing home, residential, and outpatient medical and dental care to the veterans of which war?
- World War II
- Korean War
- Vietnam War
- World War I
D. World War I
Which of the following refers to the organization of physicians according to clinical assignment?
- Medical Staff Classifications
- Medical Staff Bylaws
- Medical Staff Credentialing
- Case Management
A. Medical Staff Classifications
Which of the following statements regarding the nursing profession is true?
- RNs and LPNs/LVNs have equivalent levels of education.
- All RNs must have a bachelor's degree.
- Both associate's and bachelor's degree nursing graduates qualify to become RNs.
- An LVN certification is equivalent to an RN certification.
C. Both associate's and bachelor's degree nursing graduates qualify to become RNs.
Medical school students must pass a test before they can obtain a _____ to practice medicne.
- Degree
- Residency
- Specialty
- License
D. License
The chief information officer is a senior-level executive who is responsible for _____.
- Managing the security of all patient-identifiable information.
- Ensuring the organization's compliance with federal and state governments and accrediting body rules and regulations on confidentiality.
- Ensuring the IS implementation plans are in line with the organization's strategic vision.
- Leading the organization's strategic IS planning process.
D. Leading the organization's strategic IS planning process.
Law enacted by a legislative body is a(n) _____.
- Administrative Law
- Statute
- Regulation
- Rule
B. Statute
Which stage of the litigation process focuses on how strong a case the opposing party has?
- Deposition
- Discovery
- Trial
- Verdict
B. Discovery
Which of the following is NOT true of notices of privacy practices?
- They must be made available at the site where the individual is treated.
- They must be posted in a prominent site.
- They must contain content that may not be changed.
- They must be prominently posted on the covered entity's Web site when the entity has one.
C. They must contain content that may not be changed.
Which of the following spells out the powers of the three branches of the federal government?
- United States Constitution
- Statutes
- Administrative Law
- Judicial Decisions
A. United States Constitution
Which document directs an individual to bring originals or copies of records to court?
- Summons
- Subpoena
- Subpoena Duces Tecum
- Deposition
<p>C. Subpoena Duces Tecum</p> <br>
To comply with HIPAA, under usual circumstances, a covered entity must act on a patient's request to review or copy his or her health information within _____ days.
- 10
- 20
- 30
- 60
C. 30
The HIPAA Privacy Rule requires that covered entities must limit use, access, and disclosure of PHI to only the amount needed to accomplish the intended purpose. What concept is this an example of?
- Minimum Necessary
- Notice of Privacy Practices
- Authorization
- Consent
A. Minimum Necessary
Which of the following statements if false?
- A notice of privacy practices must be written in plain language.
- A consent for use and disclosure of information must be obtained from every patient.
- An authorization does not have to be obtained for uses and disclosures for treatment, payment, and operations.
- A notice of privacy practices must give an example of a use or disclosure for healthcare operations.
C. An authorization does not have to be obtained for uses and disclosures for treatment, payment, and operations.
Which of the following statements is NOT true about a business associate agreement?
- It prohibits the business associate from using or disclosing PHI for any purpose other than that described in the contract with the covered entity.
- It allows the business associate to maintain PHI indefinitely.
- It prohibits the business associate from using or disclosing PHI in any way that would violate the HIPAA Privacy Rule.
- It requires the business associate to make available all of its books and records relating to PHI use and disclosure to the Department of Health and Human Services or its agents.
B. It allows the business associate to maintain PHI indefinitely.
Under HIPAA regulations, how many days does a covered entity have to respond to an individual's request for access to his or her PHI when the PHI is stored off-site?
- 10 days beyond the original agreement
- 30 days
- 60 days
- 90 days
C. 60 days
Which of the following provides a complete description to patients about how PHI is used in a healthcare facility?
- Notice of Privacy Practices
- Authorization
- Consent for Treatment
- Consent for Operations
A. Notice of Privacy Practices
Which of the following statements is true of the notice of privacy practices?
- It gives the covered entity permission to use information for treatment purposes.
- It gives the covered entity permission to use information for TPO purposes.
- It must be provided to every individual at the first time of contact or service with the covered entity.
- It must be provided to the individual by the covered entity within 10 days after receipt of treatment or service.
C. It must be provided to every individual at the first time of contact or service with the covered entity.
Which of the following statements about the directory of patients maintained by a covered entity is true?
- Individuals must be given an opportunity to restrict or deny permission to place information about them in the directory.
- Individuals must provide a written authorization before information about them can be placed in the directory.
- The directory may contain only identifying information such as the patient's name and birth date.
- The directory may contain private information as long as it is kept confidential.
A. Individuals must be given an opportunity to restrict or deny permission to place information about them in the directory.
What does the abbreviation PHI stand for?
- Personal Health Information
- Protected Health Information
- Primary Health Information
- Past Health Information
B. Protected Health Information
Under HIPAA rules, when an individual asks to see hos or her own health information, a covered entity _____.
- Must always provide access.
- Can deny access to psychotherapy notes.
- Can demand that the individual pay to see his or her record.
- Can always deny access.
B. Can deny access to psychotherapy notes.
In which of the following situations must a covered entity provide an appeals process for denials to requests from individuals to see their own health information?
- When access to psychotherapy notes is requested.
- When the covered entity is a correctional institution.
- When a licensed healthcare professional has determined that access to PHI would likely endanger the life or safety of the individual.
- When the covered entity has acted under the discretion of a correctional institution.
C. When a licensed healthcare professional has determined that access to PHI would likely endanger the life or safety of the individual.
Which of the following statements is true in regard to responding to requests from individuals for access to their PHI?
- A cost-based fee may be charged for retrieval of the PHI.
- A cost-based fee may be charged for making a copy of the PHI.
- No fees of any type may be charged.
- A minimal fee may be charged for retrieval and copying of PHI.
B. A cost-based fee may be charged for making a copy of the PHI.
Which of the following provides a complete description to patients about how PHI is used in a healthcare facility?
- Notice of Privacy Practices
- Authorization
- Consent for Treatment
- Consent for Operations
A. Notice of Privacy Practices
The legal health record (LHR) is a(n) _____.
- Defined subset of all patient-specific data created or accumulated by a healthcare provider that may be released to third parties in response to a legally permissible request for patient information.
- Entire set of information created or accumulated by a healthcare provider that may be released to third parties in response to a legally permissible request for patient information.
- Set of patient-specific data created or accumulated by a healthcare provider that is defined to be legal by the local, state, or federal authorities.
- Set of patient-specific data that is defined to be legal by state or federal statute and that is legally permissible to provide in response to requests for patient information.
A. Defined subset of all patient-specific data created or accumulated by a healthcare provider that may be released to third parties in response to a legally permissible request for patient information.
Privacy can be defined as the _____.
- Limitation of the use and disclosure of private information.
- Right of an individual to be left alone.
- Physical and electronic protection of information.
- Protection of information from accidental or intentional disclosure.
B. Right of an individual to be left alone.
Confidentiality can be defined as the _____.
- Limitation of the use and disclosure of private information.
- Right of an individual to be left alone.
- Physical and electronic protection of information.
- Protection of information from accidental or intentional disclosure.
A. Limitation of the use and disclosure of private information.
Which of the following statements represents an example of nonmaleficence?
- HITs must ensure that patient-identifiable information is not released unauthorized parties.
- HITs must apply rules fairly and consistently to every case.
- HITs must ensure that patient-identifiable information is released to the parties who need it to provide services to their patients.
- HITs must ensure that patients themselves, and not other parties, are authorizing access to the patients' individual health information.
A. HITs must ensure that patient-identifiable information is not released unauthorized parties.
Which of the following terms means "treating others fairly"?
- Autonomy
- Beneficence
- Justice
- Nonmaleficence
C. Justice
Which organization issues and maintains ethical standards for the health information management profession?
- American Medical Association
- American Health Information Management Association
- American College of Surgeons
- American Hospital Association
B. American Health Information Management Association
The hospital is revising its policy on completion of inpatient history and physical examination. The chairperson of the committee suggests that the history and physical examination be performed not more than 30 days before admission or later than 24 hours after admission. One of the committee members points out that if the history and physical is performed within 24 hours after admission, then the transcribed report should be documented in the patient's record within 48 hours of admission. How should the HIM director respond to this discussion?
- Indicate that it is impossible to have a 24-hour turn around for dictation.
- Suggest that the transcribed report be documented in the patient's record within 48 hours of completion of the dictation.
- Inform the committee that Joint Commission standards require the history and physical be placed in the medical record within 25 hours of admission.
- Contact the Joint Commission to clarify their standards.
C. Inform the committee that Joint Commission standards require the history and physical be placed in the medical record within 25 hours of admission.
During user acceptance testing of a new EHR system, physicians are complaining that they have to use multiple log-on screens in order to access all the system modules. For example, they have to use one log on for CPOE and another log on to view laboratory results. One physicians suggests having a single sign on that would provide access to all the EHR systems components. However, the hospital administrator feels that one log on would be a security issue. What information should the HIM director provide?
- Single sign on is not supported by HIPAA security measures.
- Single sign on is discouraged by the Joint Commission.
- Single sign on is less frustration for the end user and can provide better security.
- Single sign on is not possible given today's technology.
C. Single sign on is less frustration for the end user and can provide better security.
To date the HIM department has not charged for copies of records requested by the patient. However, the policy is currently under review for revision. One HIM committee suggests using the copying fee established by the state. Another committee member feels that HIPAA will not allow for copying fees. What input should the HIM director provide?
- HIPAA does not allow charges for copying of medical records.
- Use the state formula because HIPAA allows hospitals to use the state formula.
- Base charges on the cost of labor and supplies for copying and postage is copies are mailed.
- Since HIPAA restricts charges to the cost of paper, charge only for the paper used for copying the records.
C. Base charges on the cost of labor and supplies for copying and postage is copies are mailed.
The sister of a patient requests the HIM department to release copies of her brother's medical record to her. She states that because the doctor documented her name as her brother's caregiver that HIPAA regulations apply and that she may receive copies of her brother's medical record. In this case how should the HIM department proceed?
- Provide the copies as requested since the sister was a caregiver.
- Provide only copies of the reports where the sister's name is mentioned.
- Refuse the request.
- Refer the individual to legal counsel.
C. Refuse the request.
Community Hospital is discussing restricting the access that physicians have to electronic clinical records. The medical record committee is divided on how to approach this issue. Some committee members maintain that all information should be available, while others maintain that HIPAA restricts access. The HIM director is part of the committee. Which of the following should the director advise the committee?
- HIPAA restricts the access of physicians to all information.
- The "minimum necessary" concept does not apply to disclosures made for treatment purposes, therefore physician access should not be restricted.
- The "minimum necessary" concept does not apply to disclosures made for treatment purposes, but the organization must define what physicians need as part of their treatment role.
- The "minimum necessary" concept applies only to attending physicians and therefore restriction of access must be implemented.
C. The "minimum necessary" concept does not apply to disclosures made for treatment purposes, but the organization must define what physicians need as part of their treatment role.
Which of the following is NOT a description of a hybrid record?
- Includes both paper and electronic documents.
- Uses both manual and electronic processes.
- Includes components generated electronically.
- Includes an equal part of paper and electronically produced documents.
D. Includes an equal part of paper and electronically produced documents.
Which of the following is NOT a challenge in implementing a hybrid health record?
- Development of processes for both manual and computer processes
- Creation of a definition of what constitutes a health records in manual and electronic format.
- Creation of a pathway toward an EHR.
- Implementation of security measures for both paper and electronic processes.
C. Creation of a pathway toward an EHR.
Incorporating a workflow function in an electronic information system would help support _____.
- Tasks that need to be performed in a specific sequence.
- Moving patients from point to point.
- Registration of patients.
- Making computer output available to laser disk.
A. Tasks that need to be performed in a specific sequence.
To run an analysis on a large set of data from many patients, the best tool is a(n):
- CDR
- CDW
- DBMS
- EHR
B. CDW
Which of the following would be the best course of action to take in order to ensure continuous availability of electronic data?
- Acquire storage management software.
- Send data to a remote site via the Internet.
- Store data on RAID.
- Use mirrored processing on redundant servers.
D. Use mirrored processing on redundant servers.
Which of the following would be considered discrete data?
- Operative Report
- Medication Dosage
- Physical Examination
- Nursing Notes
B. Medication Dosage
Which of the following technologies would allow a hospital to get as much medical record information online as quickly as possible?
- Clinical Data Repository
- Picture Archiving System
- Electronic Document Management System
- Speech Recognition System
C. Electronic Document Management System
Which of the following technologies would be best for a hospital to use in order to manage data from its laboratory, pharmacy, and radiology information systems?
- Electronic Document Management System
- Clinical Data Repository
- Picture Archiving System
- COLD System
<p>B. Clinical Data Repository</p> <br>
Which of the following encourages patients to take an active role in collecting and storing their health information?
- EHR
- Intranet Web Service
- PHR
- CDS
C. PHR
Which of the following is necessary to ensure that each term used in an EHR has a common meaning to all users?
- Encoded Vocabulary
- Controlled Vocabulary
- Data Exchange Standards
- Proprietary Standards
B. Controlled Vocabulary
Why is an ideal EHR system one that requires point-of-care charting?
- Eases duplicate data entry burden.
- Eliminates intermediary paper forms.
- Reduces memory loss.
- Supports clinical decision making.
D. Supports clinical decision making.
Which of the following is a transition strategy to achieve an EHR?
- Ancillary System Report
- Clinical Data Repository
- Electronic Document Management System
- Results Retrieval
C. Electronic Document Management System
To ensure that a computerized provider order entry (CPOE) system supports patient safety, what other system must also be in place?
- Digital Dictation
- Electronic Medication Administration Forms
- Pharmacy Information System
- Point of Care Charting
C. Pharmacy Information System
Electronic prescribing is a special case of:
- CPOE
- EHR
- PDA
- RHIO
A. CPOE
As part of an EHR system selection, due diligence should be done:
- After installing an EHR to test for acceptance.
- Before contracting for an EHR product.
- During system build to check for interface quality.
- Prior to any user authorization for access to data.
B. Before contracting for an EHR product.
Which of the following tasks may not be performed in an electronic health record system?
- Document Imaging
- Analysis
- Assembly
- Indexing
C. Assembly
Which form of wireless technology is used to beam data between devices in close proximity to one another?
- Bar Coding
- Blu-Ray
- Ethernet
- IEEE 802.11
D. IEEE 802.11
A step-by-step approach to installing, testing, training, and gaining adoption for an EHR is referred to as:
- Implementation Plan
- Migration Path
- Readiness Assessment
- Strategic Plan
A. Implementation Plan
How are health plans incentivizing providers to use EHRs:
- Denying paper claims
- External reporting
- Paying for performance programs
- Requiring use of clinical guidelines
C. Paying for performance programs
Electronic systems used by nurses and physicians to document assessments and findings are called _____.
- Computerized Provider Order Entry (CPOE)
- Electronic Document Management Systems (EDMS)
- Electronic Medication Administration Record
- Electronic Patient Care Charting
D. Electronic Patient Care Charting
A medical record that is part electronic and part paper is called a(n) _____.
- Hybrid Record
- Electronic Health Record
- Electronic Medical Record
- Electronic Data Repository
A. Hybrid Record
A SNF wanting to collect MDS assessments in a database and transmit them in a standard CMS format would use which of the following data entry software?
- Grouper
- HIS
- MS Access
- RAVEN
D. RAVEN
What is the difference between data and information?
- Data represent basic facts, while information represents meaning.
- Data are expressed in numbers, while information is expressed in words.
- Information must be kept confidential, while data are meant to be shared.
- Information is about people, while data are about things.
A. Data represent basic facts, while information represents meaning.
Data definition refers to _____.
- Meaning of data.
- Completeness of data.
- Consistency of data.
- Detail of data.
A. Meaning of data.