A typical bone has these 2 distinct regions of bone
Compact & spongy bone
The inside of the bone; important function is hematopoiesis
Marrow cavity
Difference r/t hematopoiesis in children vs. adults
Children - all bones make blood cells
Adults - only some parts of certain bones make blood cells
Region of long bone:
Head of bone
Epiphysis
Region of long bone:
Shaft of bone
Diaphysis
Bones found in the limbs
Long bones
In the femur, as in the humerus, hematopoiesis occurs only in 1) this region of the bone, which is composed of 2) this type of bone
1. Head & neck (proximal portion)
2. Spongy bone
In adult bones that don't participate in hematopoiesis, 1) what change occurs, 2) what is it due to, and 3) where does it occur?
1. Red marrow is replaced with yellow marrow
2. Yellow = fat (red was due to RBC production)
3. Spongy part of the bone
Most of bone is encased within this layer, which has 2 sublayers
Periosteum
The periosteum, which encases most bone, consists of these 2 layers
1. Tough fibrous outer layer w/collagen
2. Inner cellular layer playing key role in bone formation
Layer of periosteum w/collagen fibers
Tough fibrous outer layer
Layer of periosteum that plays key role in bone formation
Inner cellular layer
The periosteum is replaced by _____ 1 _____ on the _____ 2 _____ of the bone
1. articular cartilage
2. articular surface
Articular cartilage, which replaces the periosteum on the articular surface of bones, is composed of this glassy, very smooth cartilage
Hyaline cartilage
Glassy, very smooth cartilage that replaces the periosteum on articular surfaces of bones
Hyaline cartilage
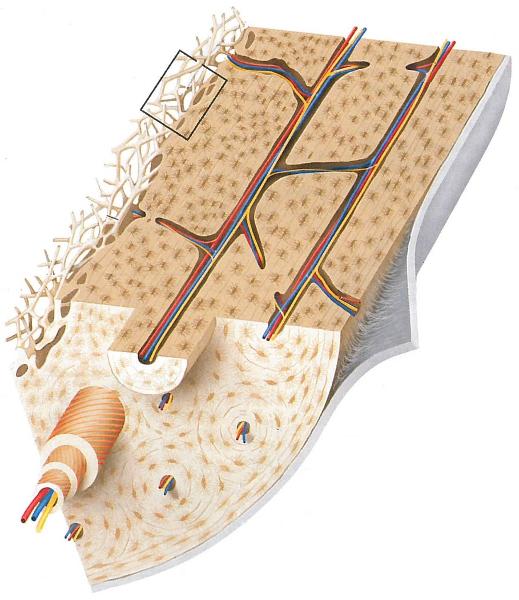
This type of bone has an orderly structure & contains a series of tunnels
Compact bone
Series of tunnels within compact bone; contain blood vessels
Central canals
The layer lining the central canals within compact bone
Endosteum
2 layers within bone that participate in new bone formation
1. Inner cellular layer of periosteum
2. Endosteum (lining central canals of compact bone)
Completely encloses spongy bone
Compact bone
-Thin layer
-Accounts for smaller volume of given bone
-Higher density, so 75% of bone by weight
Compact bone
What would happen if all of your bone was compact bone?
Too heavy to move or even sit up!!!
The circular structure surrounding one central canal; includes rings marked with osteocytes
Osteon
Cells in concentric rings within an osteon; trapped inside the matrix of compact bone
Osteocytes
1. Where are osteoblasts located?
2. What substance do they secrete?
3. What is this substance?
1. Endosteum & inner cellular layer of periosteum
2. Osteoid
3. Precursor of bone
Making the bone matrix (and thus bone formation) is a 2-step process. What are these 2 steps?
1. Secretion of the bone precursor, osteoid, from osteoblasts
2. Crystallization of hydroxyapatite (Ca++, Phosphorus) onto collagen fibers of osteoid
Where do the minerals that form hydroxyapatite and complete the 2nd step of bone matrix formation come from?
Osteoblasts - as does the osteoid that comprises the 1st step in bone matrix formation
What happens to some osteoblasts that get trapped in matrix?
-Stop secreting osteoid
-Turn into osteocytes
What function do the tiny canals that connect osteocytes serve?
Passage of nutrients & wastes
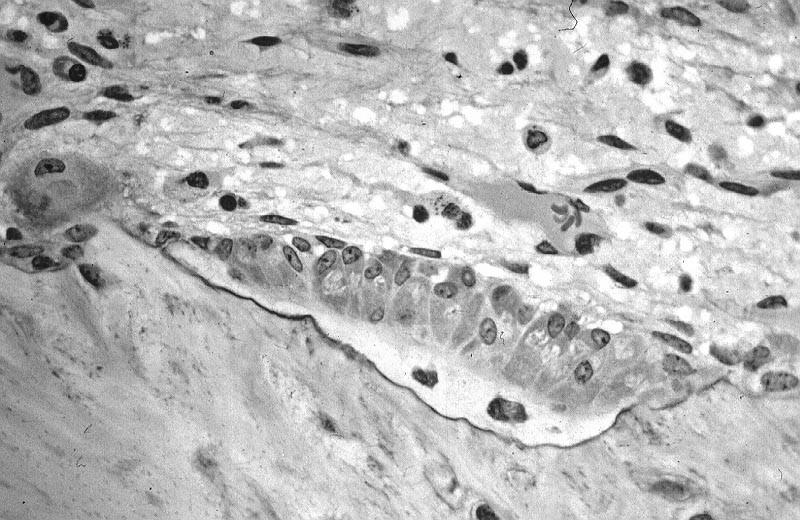
Identify which cells are osteoblasts (depositing osteoid) & which are osteocytes (trapped in osteoid)
1. White layer with 2 cells = osteocytes
2. Cells above white layer = osteoblasts
Precursor cells, forming osteocytes; responsible for bone formation
Osteoblasts
Multinucleate cells made from fusion of many macrophages; role is bone resorption
Osteoclasts
When an osteoblast becomes an osteocyte (normal life cycle), does the activity increase or decrease?
Decreases (structure simplifies as well, since no need for organelles to secrete osteoid)
Sequence of events for bone remodeling (3 steps)
1. Osteoclast attaches to bone & secretes acid (H+ ions) to dissolve bone underneath it
2. Osteoclast detaches from bone & moves on
3. Osteoblasts move into pit, secreting osteoid to build new bone
Cluster of cells functioning as "Cutting Cones", like Big Bertha; tunneling machine
Osteoclasts
Follow behind, zipping up & resealing tunnel left behind (bone formation)
Osteoblasts
Can cause significant lag in between bone breakdown & bone formation
Insufficient building blocks (Ca++, phosphorus)
Insufficient Ca++/phosphorus, which can create a lag between bone breakdown & formation, can lead to a situation not unlike what disease process?
Osteoporosis
Induces more bone growth as a response
Chronic stress (i.e. exercise) - whereas a person who leads a sedentary lifestyle would have less bone growth/remodeling
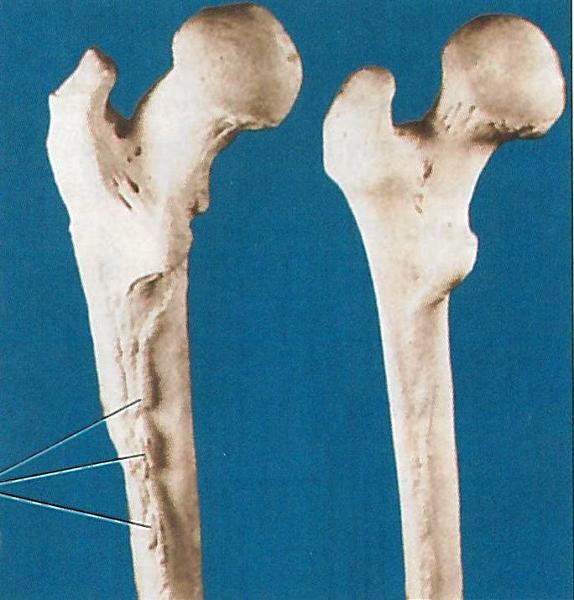
Which femur, left or right, is reflective of an individual who lived a sedentary lifestyle?
Right femur - less use of quads, which are attached to bone's ridge where growth is expansive on left femur
Made up of lots of tiny struts of bone; space between struts filled with marrow
Spongy bone
Tiny struts that form the composition of spongy bone
Trabeculi
Since trabeculi surfaces are covered by endosteum, bone is deposited in __1__ layers, with the __2__ bone being the outermost layer
1. circular
2. youngest
How do the trabeculi of spongy bone line up in relation to direction? How is this different in adults vs. infants/toddlers?
-Parallel to the direction of force (i.e. along stress lines)
-Infants/toddlers don't put ambulatory stress on bones until much later in development
Bone density condition increasing risk of fractures
Osteoporosis
Bone disorder characterized by vitamin D deficiency in children; uncommon in developed countries
Rickets
Caused by vitamin D or Ca++ deficiency in adults
Osteomalacia
2 bone disorders which can result in bone deformations which aren't reversible
Rickets & osteomalacia
Repair of broken bone is similar to bone development, but requires these 2 components
-Blood vessels
-Chondrocytes
4 steps of bone remodeling following fracture:
1. Blood forms hematoma - angiogenesis
2. Collagen deposited
3. Osteoblasts deposit temporary bone to stabilize break
4. Blasts & clasts work together to breakdown/rebuild
After a fracture, after spongy bone is converted to compact bone, these cells perform the final "editing"
Osteoclasts
Even though skeleton is bone, it still requires this as the foundation for its development
Cartilage
Type of fracture caused by overuse r/t repetition
Stress FX
Type of fracture where bone isn't broken all the way through
Incomplete FX
Type of fracture where bone is broken all the way across
Complete FX
Type of fracture where 2 pieces are still together
Nondisplaced FX
Type of fracture where 2 pieces, or ends, are apart
Displaced FX
Type of fracture that is broken or splintered into 3 or more fragments
Comminuted FX
List fracture types from least to most severe
-Stress
-Incomplete
-Complete
-Nondisplaced
-Displaced
-Comminuted
Most common fracture site in body - due to a medial forceful thrust
Clavicle FX
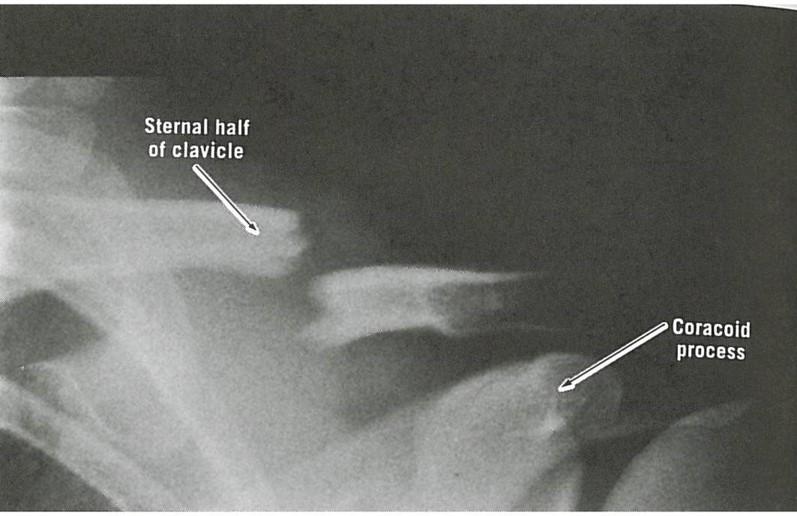
Note that distal end of clavicle sags, while proximal end is displaced upwards
No information...
4 most clinically relevant bones
-Femur
-Vertebrae
-Radius
-Ulna
"Porous bone" - disease of the aged; more common in women
Osteoporosis
Most common sites of FX's r/t osteoporosis
Neck of femur (hip) & spine
DX tool for bone health; can be used to assess bone density for both hip & spine, which can predict risk of future FX's
DEXA scan (Dual-energy X-ray absorptiometry)
Excellent DX tool to detect early signs of osteoporosis & estimate risk of future FX's
DEXA scan
The World Health Organization (WHO) has adopted standards for bone health, called T & Z scores. While Z scores are measured in a percentile based on age & gender (similar to physical development of children), where having a Z score of 80% is better than 40%, T scores have 4 different classifications. What are these 4 classifications?
1. Normal bone: Better than -1 (w/in 10% of average)
2. Osteopenia: Between -1 & -2.5 (about 10-25% less)
3. Osteoporosis: Less than -2.5 (about 25% less)
4. Established (severe) osteoporosis includes presence of non-traumatic FX
Under ideal circumstances, what's the best treatment for osteoporosis? Once diagnosed, what's the treatment regimen?
*Prevention (DEXA scan can show early density issues)
-Diet high in vitamin D & Ca++
-Bisphosphonates (drug)
-Exercise (stress = strength)
18-month training program designed to add bone density to hips & vertebrae & strengthen lower extremities, mostly through resistance exercise, education & diet. This will reduce the risk of falls.
Osteo-cise
Why does aging result in bone loss?
Balance shifts to bone resorption, & osteoclast activity isn't matched as well by osteoblast activity
Abnormal spine curvature r/t compression FX's of multiple vertebrae
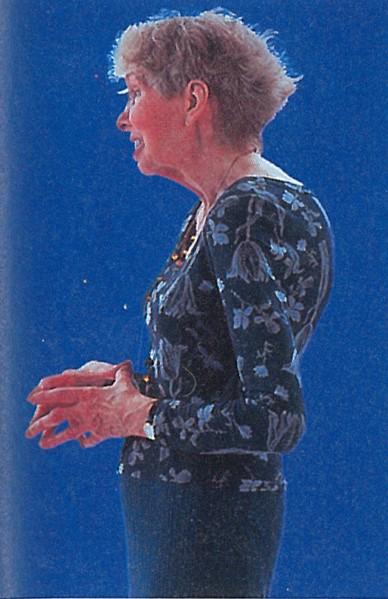
Kyphosis

Normal MRI of spine vs. =>

MRI of compression FX (see white arrow)
Why is osteoporosis more common in women?
-Lower starting bone density
-Loss of estrogen following menopause reduces bone deposition
What 2 features complicate vertebral compression FX's?
1. Tilts superior vertebrae anteriorly (most common)
2. Ligaments adjust to shortened vertebrae, cinching down & locking it into place
*Only SX can correct this
The majority of vertebral FX's are located where?
Lumbar region
As recent as 25 years ago, this FX was tantamount to a death sentence r/t how it was treated
Hip FX
In a bad ankle sprain, this ligament is almost always the first to rupture
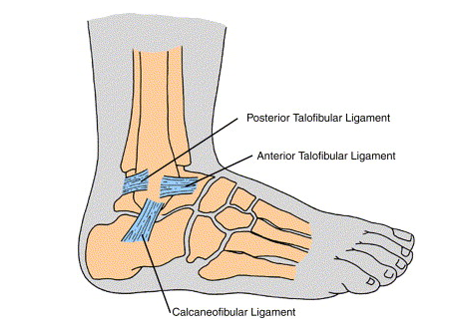
Anterior Talofibular Ligament (ATL)
Ligaments do what when rested (opposite of muscles)? This means initially we'll passively rest, & then actively rest by doing resistance training in the foot (muscles & tendons of foot are strengthened, taking "load" off ligaments)
Shorten
A ligament in this state, which usually occurs following injury, places the person at greater risk of another sprain
"Lax" ligament (loose, not allowed to shorten back to normal thru rest)
3 of these; attach to ischial tuberosity; can avulse from bone (usually not all 3 due to amount of force required) at high speeds & with rapid acceleration & deceleration
Hamstrings
Bone d/o of young adolescents; chronic injury characterized by painful lump just below knee; usually resolves w/rest
Osgood-Schlatter
If you're considering Osgood-Schlatter as a DX, but a patient's symptoms are acute, what else must you consider?
Avulsion injury (Osgood-Schlatter has slow onset)
Painful condition from irritation of the anterior tibia region; can involve posterior tibialis muscle; rapid increase in activity level increases risk, & rest is the treatment
Shin splints (medial tibial stress syndrome)
What's the stress FX continuum?
Progression from chronic tendinitis => stress reaction => stress FX => bone FX (if S/S are ignored)
Approximately 85% of body's metabolic activity & heat production come from these
Muscles
Muscle repair is __1__ controlled and __2__ directed
1. Hormone
2. Blood
Hormones involved in muscle remodeling
-GH (initiates repair)
-Insulin-like growth factor-1 (IGF-1): finalizes repair
Prime mover; muscle primarily responsible for given joint's action; if more than one muscle is involved, this is supplying the most force
Agonist (muscle)
Muscle that opposes prime mover (agonist) at a joint
Antagonist (muscle)
Muscle that works w/agonist to further muscle action
Synergist
This muscle type is found on the opposite side of a limb or the body
Antagonist (muscle)
Muscles must overcome these 3 forces
1. Gravity
2. Inertia
3. Force of opposing muscle group
How is a joint, say the knee, stabilized during exercise or activity?
Agonist & antagonist muscles cooperate to stabilize it
How do muscles show efficiency of patterned movement, such as when running?
Quads are first activated when running, then hamstrings
*Cooperating by not getting in each other's way
What are the 3 types of skeletal muscle?
Type I: Slow twitch
Type IIa: Fast twitch endurance (FO)
Type IIb: Fast twitch power (FG)
Between the 3 skeletal muscle types (ST/FO/FG), give the size of each
ST: small
FO: medium
FG: large
1. Which of the 3 skeletal muscle types would be called upon for minimal work?
2. What about for a heavy load or when other fibers are fatigued?
1. Slow twitch (ST)
2. Fast twitch power (FG)
Attach muscle to bone
Tendons
Attach bone to bone
Ligament
Why does healing take so long with ligament/tendon damage?
Blood vessels absent or sparse
A muscle tear; usually graded
Strain
Injury to a ligament r/t overstretching
Sprain
Classic tendon structure
Tendon => muscle => tendon
What's the name for a mild Achilles injury? What's the treatment?
-Peritendinosis
-Ice & grabbing cord from base & pulling up several times to break up adhesions
Longest tendon of the body

IT band (connects from hip to lateral knee)
Tendons with wide, sheet-like attachments in which the attachment of a broad, flat muscle occurs over a wide area; found primarily in the lower back, ABD wall, skull, palms of hands & soles of feet
Aponeuroses
Muscle that acts to flex the spine; important for posture; encased in a sheath formed from 3 aponeuroses
Rectus abdominus
Prime flexor of the elbow; contributes most force to flexion
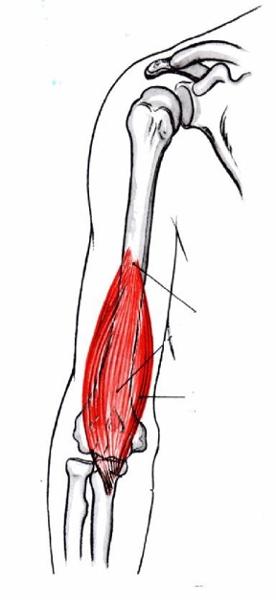
Brachialis
Synergistic flexor of elbow; supinates forearm
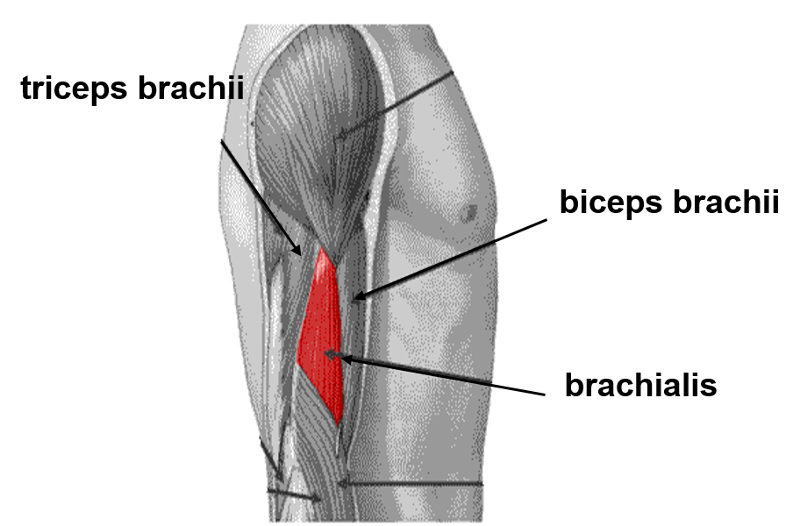
Biceps brachii
Extensor; extends elbow
Triceps brachii
Muscle group (4); extend knee & flex hip
Quadriceps
The quads are innervated solely by this nerve
Femoral nerve
Muscle group (3); flex knee & extend hip
Hamstrings
The __1__ is the prime move of plantar flexion, while the __2__ is the prime mover when the knee is extended
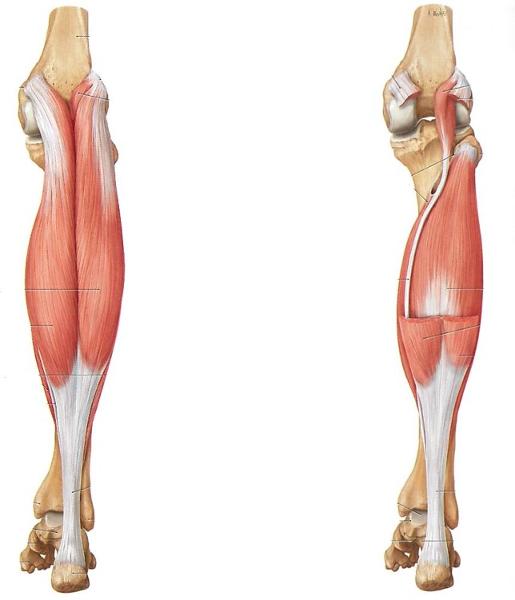
1. Soleus (right)
2. Gastrocnemius (left)
Prime mover of dorsiflexion; flexes big toe; sometimes source of shin splints
Tibialis anterior
What's the concept of "remote control" in relation to muscles, and what are some examples?
-Muscles having role in multiple joints
-TFL, plantaris, & peroneus longus
Leading cause of lateral knee pain
IT Band Syndrome
Two muscles which become one (level of the femur); strongest of muscles that flex hip
Iliacus & psoas (iliopsoas - hip flexors)
Muscle that sits over sciatic notch that causes sciatica when inflamed
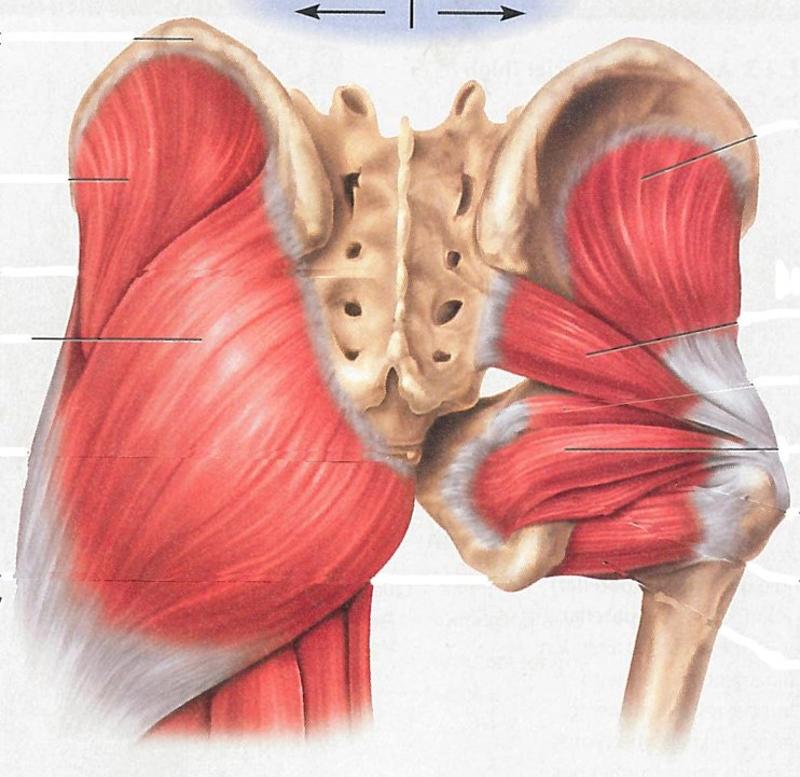
Piriformis (middle right attaching to mid-sacrum)
Longest nerve in body - extending from hip to foot
Sciatic nerve
What are some causes of back pain resulting from straining the paraspinal muscles?
-Lifting/twisting
-Poor fitness
-Overuse
1. Piriformis syndrome can lead to this
2. Treatments include...
1. Sciatica (lower back pain)
2. RICE, NSAID's, rolling out area, ultrasound TX
Thin membrane lining joint cavity; nourishes & lubricates articular cartilage
Synovial membrane
Deepens socket (labrum) or acts as wedges for a better fit between bones
Fibrocartilage
Fluid-filled sac that cushions space between tendons & bones
Bursa
Sleeve-like, loose fibrous layer attached to articulated surfaces
Capsule
Provides GLASSY surface to reduce friction between bones
Articular cartilage
"Shrink-wrapping" tissue which prevents tendons from bowstringing away from bone
Retinaculum
Arrangement of ligaments along most joints for directional support
Cross-stitch
Perforating fibers of periosteum, which penetrate bone & help attach tendon
Sharpey fibers (under flap)
When bursa are wrapped around a tendon, what are they called?
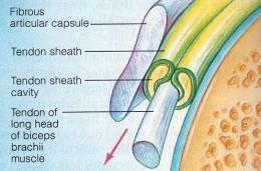
Tendon sheath
Bursitis is most common in this joint
Shoulder
Increased amount of joint fluid in response to infection, inflammation, crystals, or increased friction is called:
Effusion
Consists of fibrous connective tissue; lined inside with synovial membrane
Capsule
Large class of inflammatory disorders in synovial joints
Arthritis
Chronic degenerative disease caused by loss of articular cartilage; distinguished by its lack of inflammation, despite the "itis" suffix
Osteoarthritis
TX for bursitis
RICE, NSAID's (ABX if infection present)
Carpal tunnel TX
-Wrist brace to limit movement
-Cortisone injections
-SX (last resort)
Joint designed for ROM, not stability
Shoulder
Clinically significant joint; very mobile, yet unstable, gets dislocated often
Glenohumeral joint (shoulder)
Strongest joint of the body
Hip joint (more than 1/2 of femoral head in acetabulum)
A shoulder dislocation occurs when the __1__ comes out of its __2__ socket; 95% of the time, the shoulder is dislocated __3__; treatment is a __4__, followed by immobilization (sling) and rest
1. Humerus
2. Glenoid
3. Anteriorly
4. Reduction (replacing arm in shoulder joint)
Largest, most complex joint in body; strength depends mostly on ligaments, muscles, and tendons
Knee (femur & tibia - not fibula)
This bone is a sesamoid bone, meaning it's within a tendon
Patella
How can you test for an ACL injury?
Move tibia forward (drawers test)
"Unhappy triad" of ACL injuries
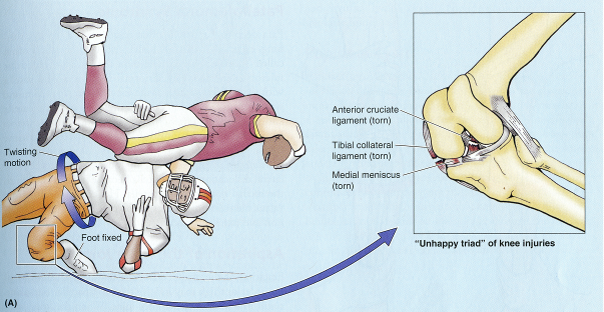
Tear of ACL, tibial collateral ligament, & medial meniscus
Articular cartilage & bone wear away; common in weight bearing joints, distal finger joints, & hips
Osteoarthritis (OA)
1. What activities reduce symptoms r/t osteoarthritis?
2. What medications are helpful?
1. Exercise - such as swimming & aquajogging
2. Embrel (cytokine inhibitor) and/or NSAID's
Autoimmune form of arthritis
Rheumatoid arthritis (RA)
The ligaments that stabilize the __1__ joint stretch during pregnancy due to secretion of __2__
1. Sacroiliac (SI) joint
2. Relaxin
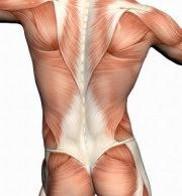
This huge, superficial group of 3 muscles are the common site of back strains r/t heavy lifting, twisting, or sudden movement
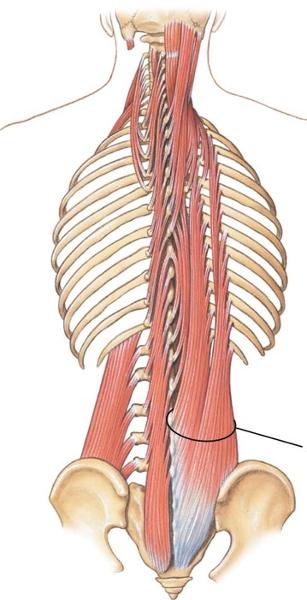
Erector spinae
Technical name for "runner's knee"
Patellofemoral Syndrome
The peripheral nervous system consists of these 2 components
-Nerves (bundles of axons)
-Ganglia (groups of neuronal cell bodies)
A neuron consists of these 3 parts
-Dendrite (receives input from other neurons)
-Axon body
-Axon terminal (releases neurotransmitter)
Part of neuron that receives information from other neurons
Dendrite
Part of neuron that releases neurotransmitter
Axon terminal
The message being transmitted by neurotransmitters is a mix of these two types of messages
Excitatory & inhibitory
What determines whether a neuron will fire?
Sum of excitatory & inhibitory neurons (more excitatory = fire)
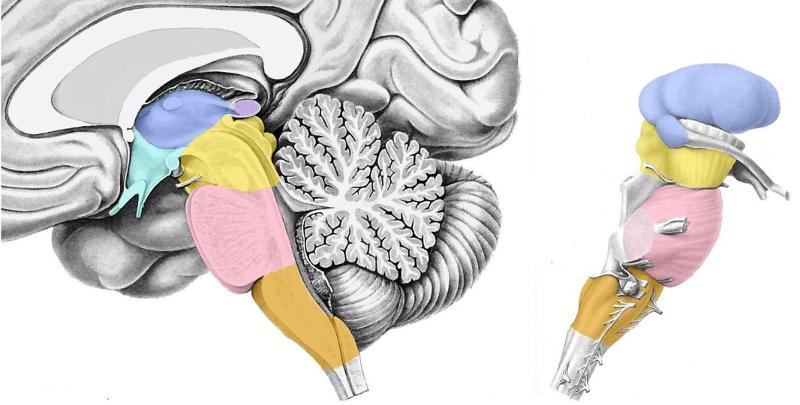
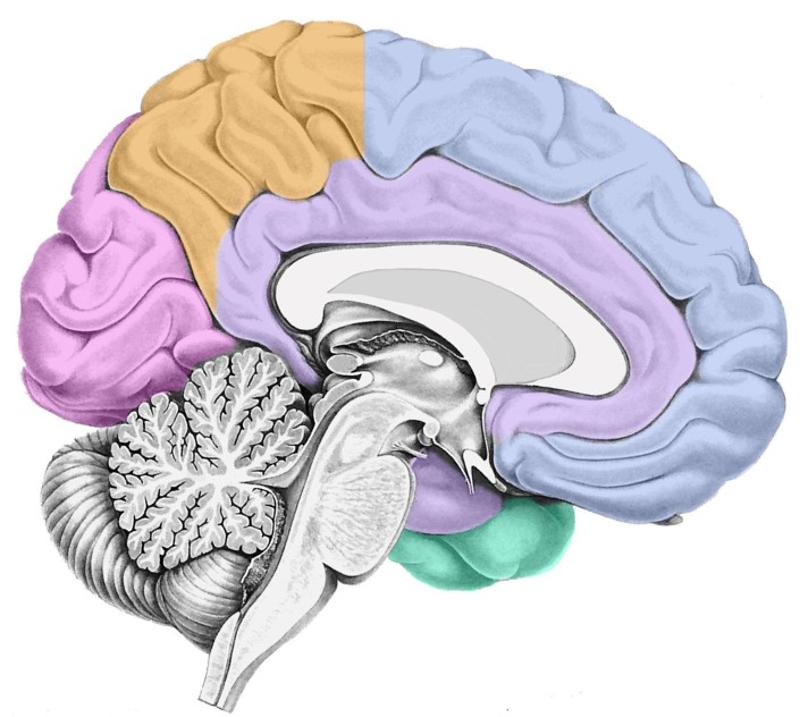
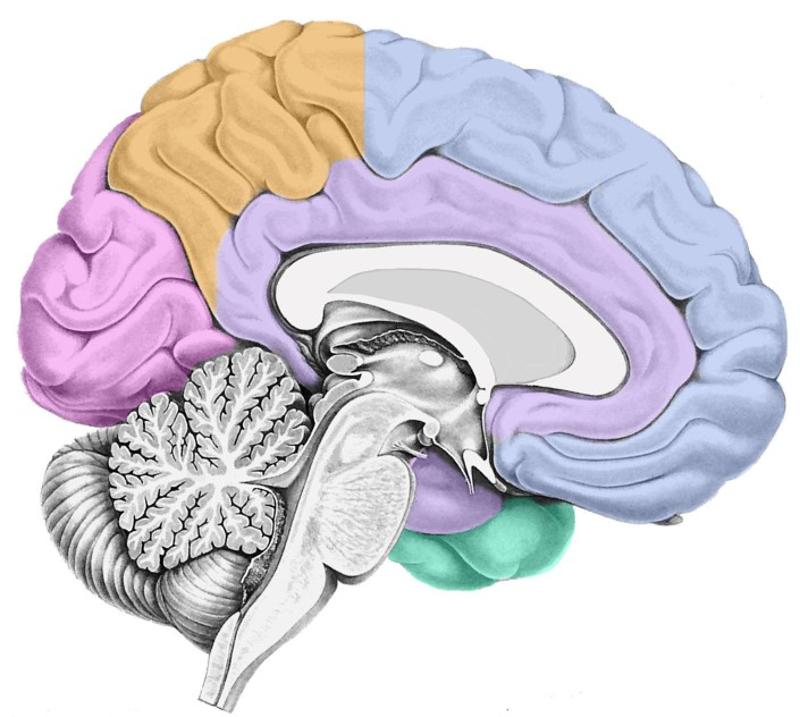
Locate the following:
-Thalamus
-Hypothalamus
-Midbrain
-Pons
-Medulla
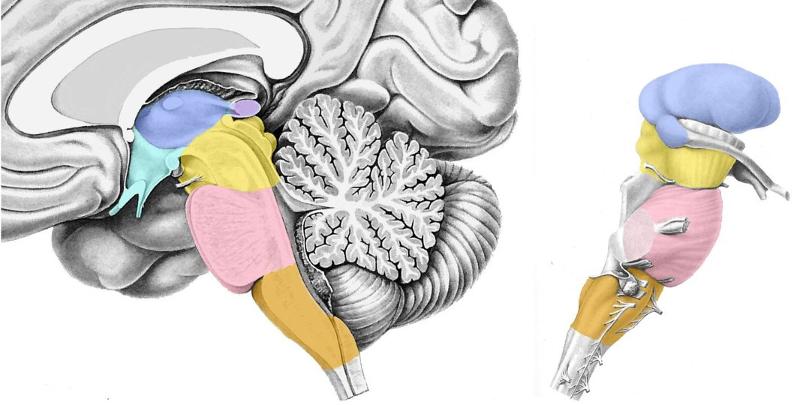
In order of descending colors (hypothalamus is under & to right of thalamus - colored green)
*Lateral view to right is also descending, but hypothalamus not pictured - so skip
Relays information to cerebral cortex; a left & right side, which are completely independent of each other
Thalamus
Deals with "housekeeping"; temp control, BP, thirst/appetite, sex drive, & lactation
Hypothalamus
The brainstem is divided into these 3 parts
-Midbrain
-Pons
-Medulla
Posterior & inferior to cerebral cortex; mostly involved in motor control
Cerebellum
Largest part of brain
Cerebral cortex
Depression or fissure in the surface of the brain
Sulcus
Ridge on the surface of the brain
Gyrus
This colored matter forms the exterior of the cerebral cortex
Gray matter surrounds white matter
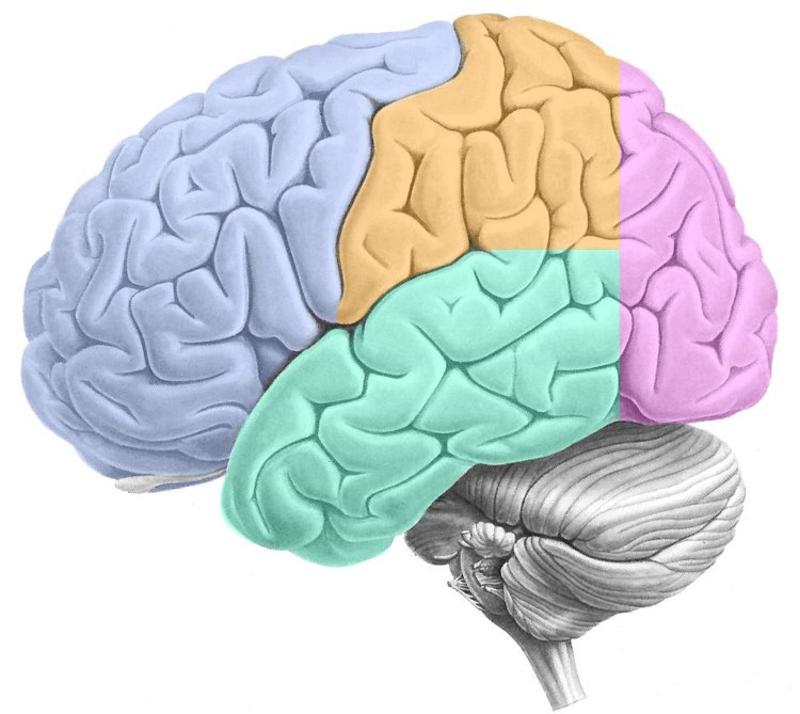
ID the following:
-Frontal lobe
-Parietal lobe
-Occipital lobe
-Temporal lobe
-Central sulcus
Frontal: Purple opposite side of cerebellum
Parietal: Orange behind frontal
Occipital: Purple above cerebellum
Temporal: Green under frontal/parietal
Central sulcus: Crease between frontal & parietal
Locate the limbic lobe

Surrounds corpus callosum
Locate the hippocampus
*What lobe is it part of?

Inferior portion of limbic lobe that swings back & under corpus callosum towards cerebellum
Generally considered the part of the cortex most susceptible to seizures
Hippocampus
Responsible for forming long-term memories (not storing!)
Hippocampus
Tube embedded in temporal bone; filled with fluid; receives sound waves which excite auditory receptor cells (hair cells)
Cochlea
Therapy for total deafness; excite auditory neurons in the auditory relay nucleus (cochlea) directly
Cochlear implant (hearing aid)
Where does auditory information go once it's received by the cochlea & transferred to CN VIII?
-Sent to nucleus at junction of pons & medulla
-Travels up to Thalamus
-Then to both left & right primary auditory cortices (AI)
Why would a person suffering damage to one hemisphere of the auditory cortex (left or right) not necessarily experience deafness in either ear?
Signals from each side are collected bilaterally, so damage to the right wouldn't stop information from left reaching right cortex
Essential for language comprehension (spoken or written); damage here causes _____'s aphasia, resulting in inability to comprehend language, although individual can still speak
Wernicke's area (Wernicke's aphasia)
Type of aphasia resulting in patient being unable to comprehend language, although they're still able to speak
Wernicke's aphasia (lesion to Wernicke's area)
Essential for language production (speech or writing); damage here will result in speech production being limited, from modest deficits in sentence generation to complete inability to speak
Broca's area (Broca's aphasia)
Probably more r/t language comprehension than production; located posterior & superior to Wernicke's area
Angular gyrus
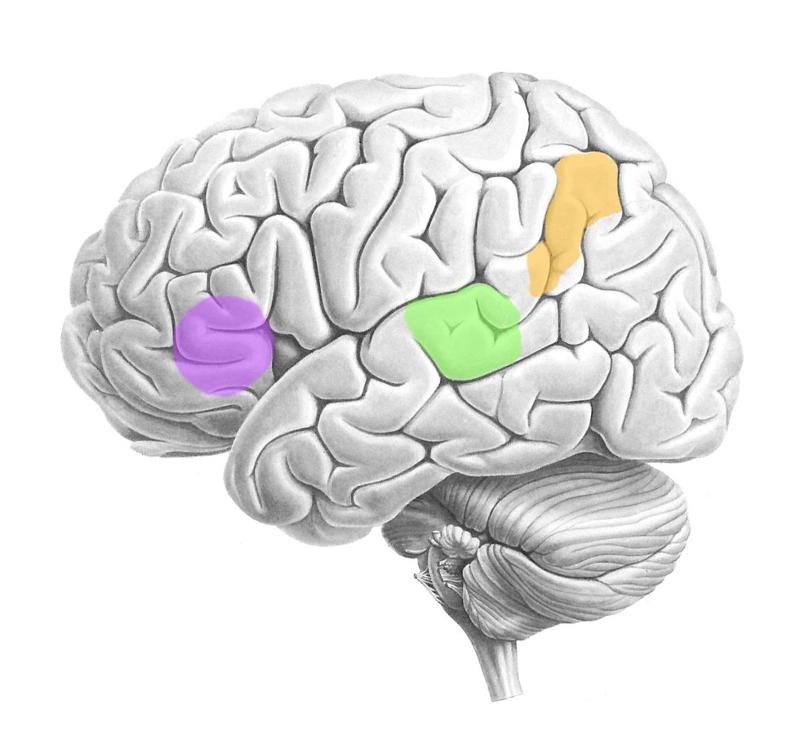
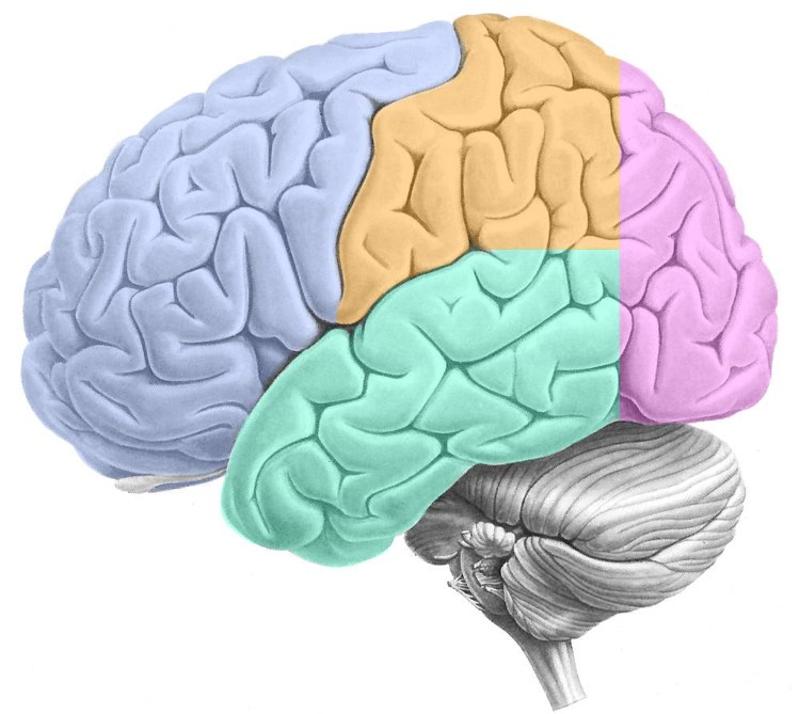
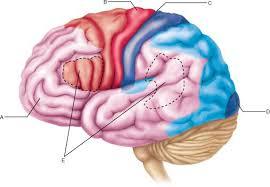
ID the following:
-Wernicke's area
-Broca's area
-Angular gyrus
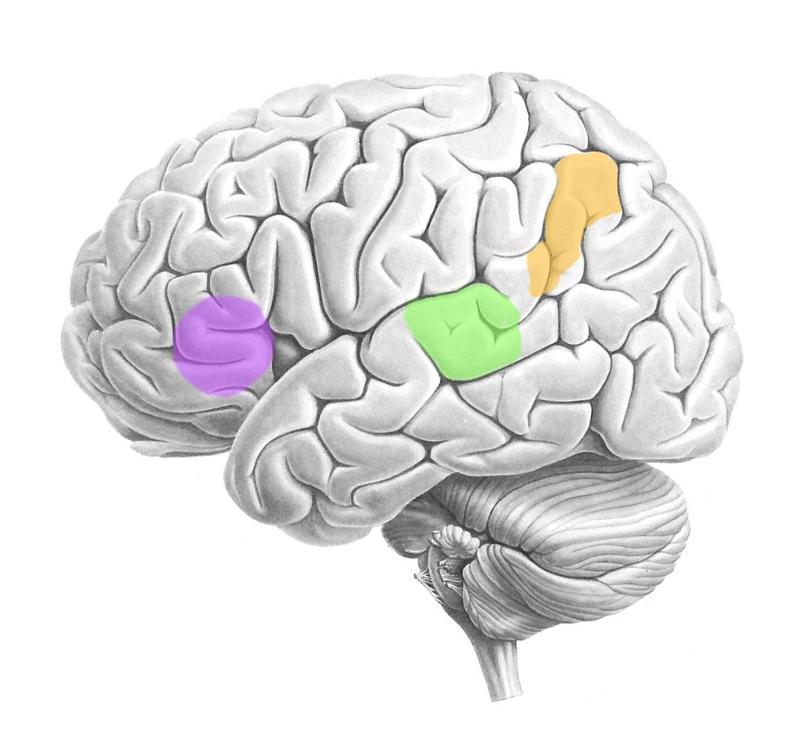
Wernicke's area: Green (temporal lobe)
Broca's area: Purple (frontal lobe)
Angular gyrus: Orange (parietal lobe)
These areas are found only in the left hemisphere in almost all right-handed people & about 70% of left-handed people
Wernicke's, Broca's, Angular gyrus

A person with a lesion in this region may suffer from what disorder?

Anomia - patient can't remember names of common objects or famous people
If a person suffering from anomia (caused by lesion of temporal lobe), and they were shown a comb, how would they describe it?
They'd be able to describe what it's used for, but not be able to remember its name
Where's the primary visual cortex (VI) located?
Occipital lobe
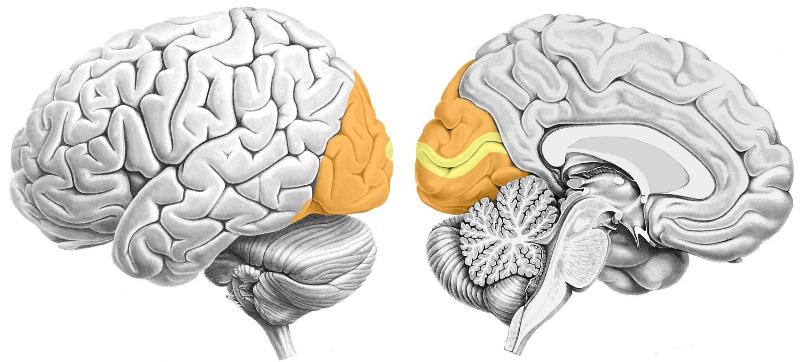
What sensory cortex is part of this lobe?
Primary visual cortex & higher-order visual cortex (occipital lobe)
Sheet of neurons lining 2/3 of the eye
Retina
Outermost layer of the retina
Rods & cones
Innermost layer of the retina
Relay neurons whose axons form the optic nerve
Where is the first visual relay in the brain?
Thalamus
Where do axons cross in the visual pathway?
Optic chiasm
Optic nerve axons (50%) that cross the optic chiasm send information to this cortex
Contralateral visual cortex
Optic nerve axons (50%) that don't cross the optic chiasm send information to this cortex
Ipsilateral visual cortex
Rule for visual system:
1. Information from the right half of the visual field goes to what half of the brain?
2. Info from the left half of visual field goes to what half?
Right visual => left half brain
Left visual => right half brain
Sees right visual field
Left visual cortex (occipital lobe)
Sees left visual field
Right visual cortex (occipital lobe)
1. What would happen if a lesion occurred along the optic nerve prior to the optic chiasm?
2. What if the lesion occurred after the optic chiasm (closer to visual cortex in occipital lobe)?
*Picture on reverse side
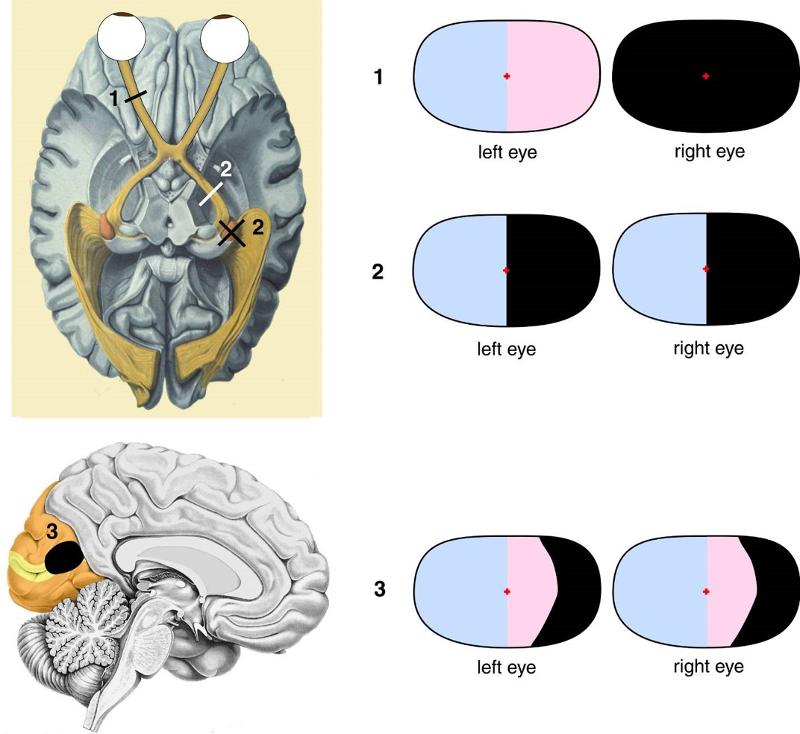
1. The side of the lesion would be blind
2. If the left tract had a lesion, the right half of each eye's field of vision would be gone
Caused by atherosclerotic-like deposits that build up behind the retina on the central region; responsible for high visual acuity (foveal vision) needed to read books, look at pictures, & other fine detail activities
Macular degeneration
While the spinal cord is part of the CNS, its projections, the _____ _____ _____, are part of the peripheral nervous system
Dorsal root ganglia
The spinal cord is shorter than the vertebral column:
1. What's the space inferior to the spinal cord called?
2. What's it useful for?
1. Lumbar cistern
2. Injecting drugs or drawing CSF for testing
Color of the outer layer of the spinal cord
White matter surrounding gray matter
Part of peripheral nervous system containing cell bodies of somatosensory neurons
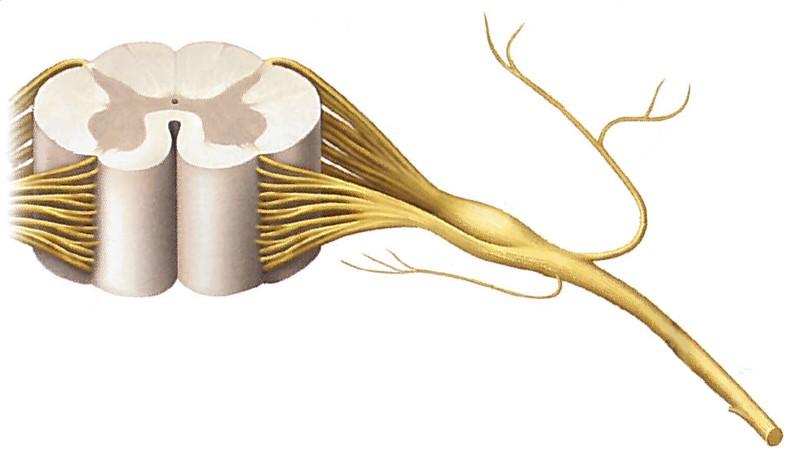
Dorsal root ganglion (just before dorsal roots connecting to spinal cord)
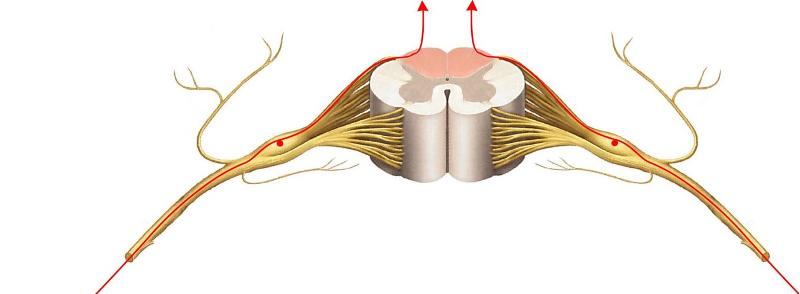
The central axonal branch of each __1__ neuron runs up the spinal cord in the __2__ matter; these axons make up a tract called the _____ 3 _____
1. Touch
2. White
3. Dorsal columns (pink highlights between dorsal horns)
How does touch pathway convey information?
1. One axonal branch to skin detects touch
2. One axonal branch through white matter to brain stem (medulla)
3. Goes to 2nd relay in thalamus
4. Cross on way primary somatosensory cortex (SI)
Touch information from the left side of the body will terminate where?
Right primary somatosensory cortex (SI) - pathway crosses after thalamus
1. What's the red area?
2. What's the blue area behind it?
3. What separates the two?
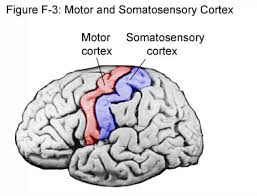
1. Primary motor cortex (red)
2. Primary somatosensory cortex (SI - blue)
3. Central sulcus
As the touch relay pathway travels up the axonal branch in the white matter of the spinal cord, what 2 relay points does it hit before reaching the primary somatosensory cortex (SI)?
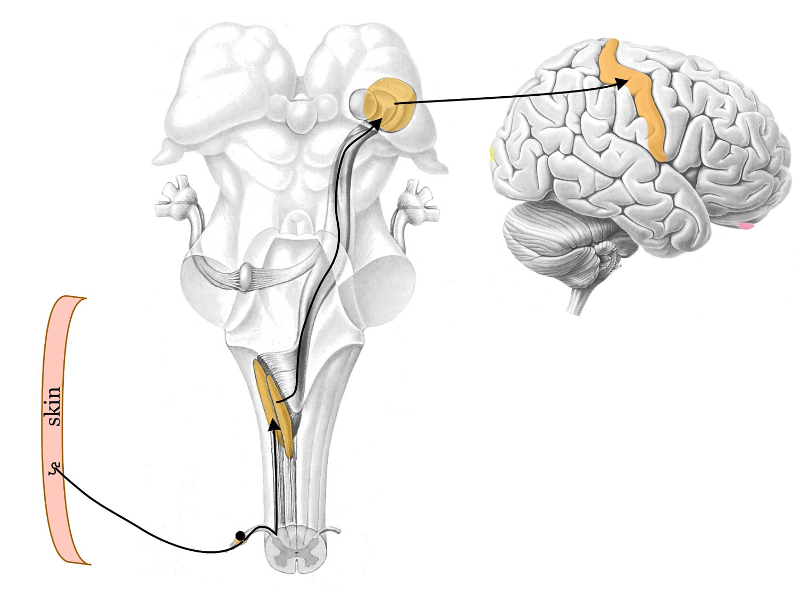
1. Relay nucleus in brainstem (medulla)
2. Relay nucleus in thalamus
Pathway for touch relay pathway is same for face with one exception - touch neurons have cell bodies in the __1__ ganglion, and the 1st relay occurs in the __2__ of the brainstem, not the __3__
1. Trigeminal
2. Pons
3. Medulla
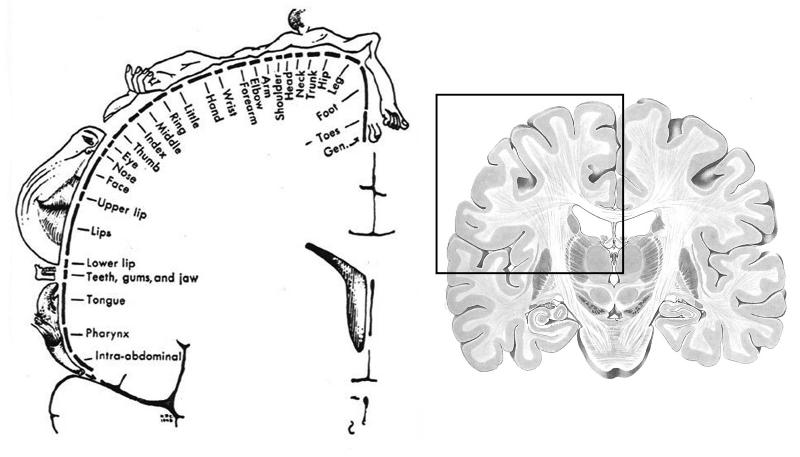
1. What's the image on the left depicting?
2. If this is an anterior view, what would happen if a lesion occurred where "leg" is mapped?
1. Somatotopic "touch" map for SI (primary somatosensory cortex)
2. This would depict right side of SI, so there would be touch deficit in left leg
Deficits resulting from a lesion in the primary somatosensory cortex (SI), which would be localized to opposite side using somatotopic "touch" map (i.e. leg, arm, GI, etc.), would produce what potential deficits?
-Lose ability to accurately locate touch/pinprick
-Lose ability to ID objects by feel
-Lose ability to ID a letter/number drawn by an examiner on hand
Most of the axons in the pain/temperature pathway are of this variety
Nociceptive
Believed to be the major pain-processing area in the cortex
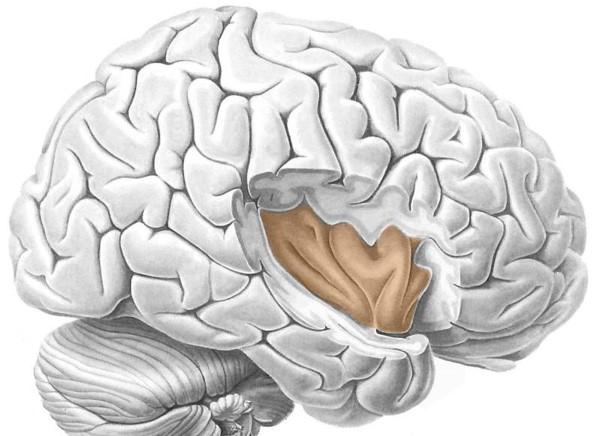
Insula
1. All pain/temp neurons in the face & head have cell bodies in what ganglion?
2. Where does information travel to from this ganglion?
3. What's different from touch relay pathway?
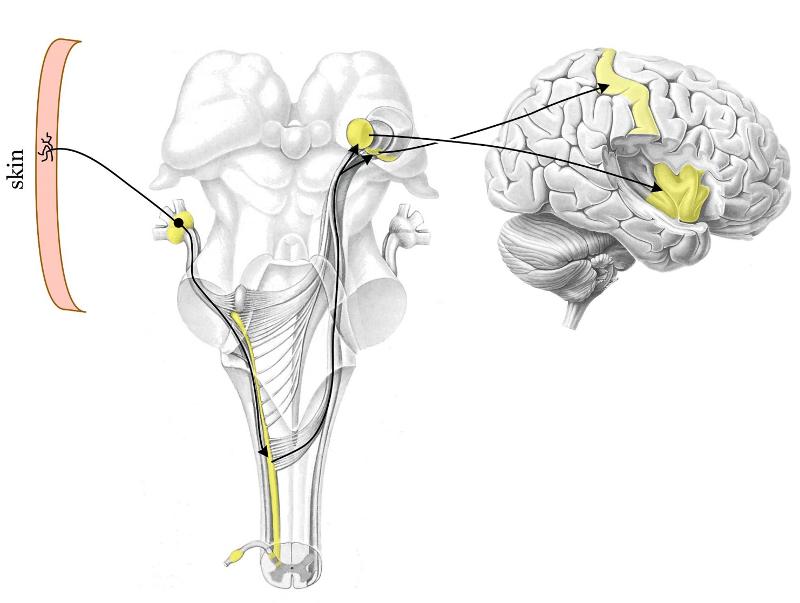
1. Trigeminal
2. Thalamus (not same part as touch pathway)
3. Some info goes to SI for general pain location, but most goes to insula to process pain
Whereas the face/head nociceptors have their cell bodies in the trigeminal ganglion, the body's nociceptors house their cell bodies in the _____ ganglia
Dorsal root
1. First "relay nucleus" for body's pain reception
2. Message then travels along this highway
3. The highway ends here
1. Dorsal horn (yellow)
2. Spinothalamic tract (through entire brainstem)
3. Thalamus
Dull pain nociceptors are activated by strong mechanical stimulation, intense heat/cold, & these substances
-Histamine
-Prostaglandin
-Serotonin
When a dull pain nociceptor is activated, it not only fires spikes, but also releases a peptide, __1__ from its own endings; this peptide stimulates __2__ cells, producing __3__. Substances (histamine, prostaglandin, serotonin) further stimulate nociceptor, which continues to fire even after stimulus is gone; this is why dull pain nociceptors generate prolonged pain & contribute to inflammation
1. Substance P
2. Mast cells
3. Histamine
A person with a herniated disc will have these 2 kinds of pain
1. Low back pain from trauma/inflammation of local connective tissue (ligaments, etc.)
2. Pain radiating down associated dermatome (squeezing causes axons to fire - brain interprets as pain from dermatome)
Why do narcotic drugs relieve pain?
Mimic pain suppression neurotransmitters coming from midbrain, which inhibit nociceptors in dorsal horn (neurotransmitters similar to opiates)
"Unhealthy" pain; not caused by tissue injury, but CNS changes, such as damage to part of pathway; chronic & not easily controlled
Neuropathic pain
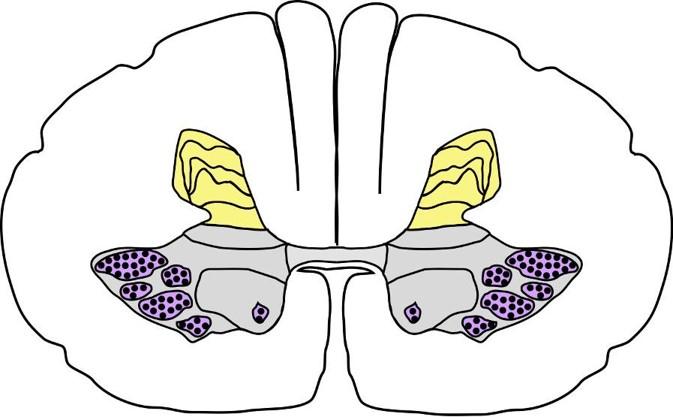
All motor neurons send their axons out to where?
Skeletal muscles (cause contraction)
Cell bodies of motor neurons are located where?
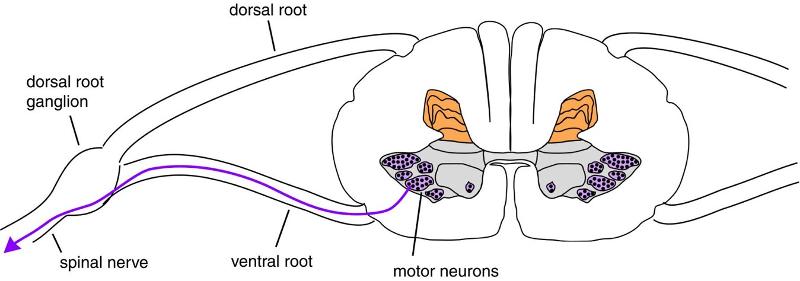
Ventral horn of the spinal cord (blue)
How are motor neurons arranged in the spinal cord?
In groups - each group corresponds to a particular muscle
Motor neurons that control muscles of the face/head have their cell bodies in the __1__; their axons go out to their muscle targets via _____ 2 _____.
1. Brainstem
2. Cranial nerves
The descending motor pathway crosses over to the contralateral side of the spinal cord just below this structure
Medulla (bottom of brainstem)
Corticospinal tract carrying signals from the right motor cortex will run through the spinal cord on which side?
Left side
A patient with damage to their left motor cortex will have motor symptoms appear on what side of their body?
Right side of body (opposite)
There is an elaborate mechanism in the brainstem & cortex for controlling eye movements. The master controller in the brainstem is a large bulge on the dorsal surface of the midbrain, called the:
Superior colliculus
Information from vestibular hair cells, located in the otolith organs, send information to brainstem via 1) what ganglion, and 2) where do they travel?
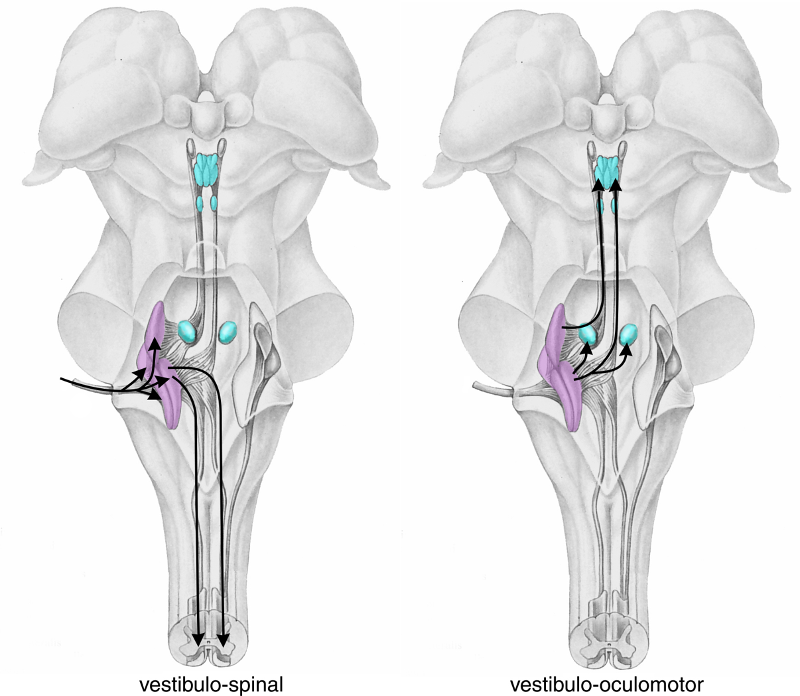
1. Scarpa's ganglion
2. Vestibular nuclei (purple - middle)
This reflex cancels out the unintended head rotation that results from activities such as walking (foot strikes ground), causing eyes to rotate in opposite directions to stabilize image on retinas; suppressed during intentional head rotation
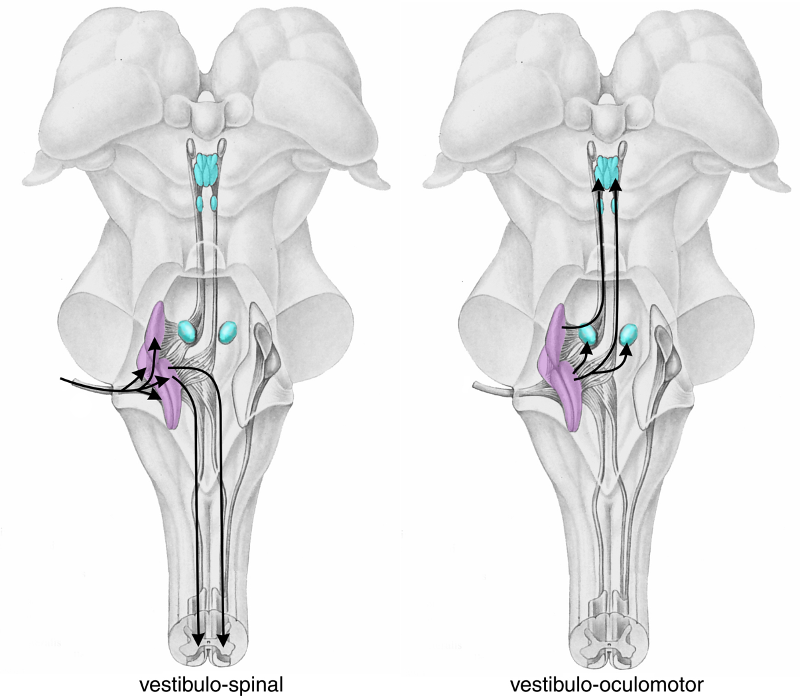
Vestibulo-ocular reflex
Damage to cerebellum causes what type of problems?
Motor (largest input by far to cerebellum is from gray matter forming base of pons - which deals heavily with motor response)
An information loop exists between the motor cortex & cerebellum; since the motor cortex is a crossed system, but the cerebellum isn't, how many times do the connections in the loop cross the midline?
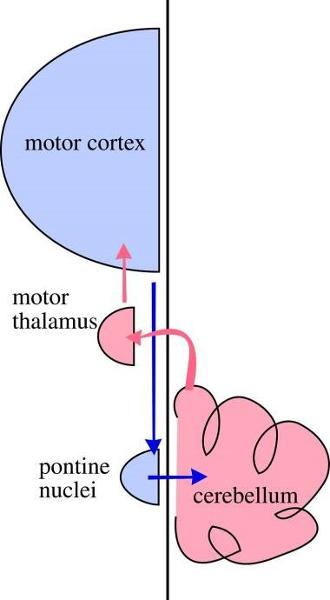
Twice
Damage to the medial portion of the cerebellum, or vernis, may cause this motor problem
Instability when standing (i.e. swaying when stationary, or when eyes are closed, patient unable to stay upright)
1. What test, when performed, will yield these results if positive?
-Movements too large
-Patient has intentional tremor - hand oscillates with extension, but no tremor at rest
-Movement broken down into smaller movements (sequential)
2. What is the probable diagnosis?

1. Asking patient to alternately touch provider's finger & then own nose
2. Cerebellar ataxia (bottom of pic)
Patient's with cerebellar disease will exhibit what characteristic r/t their gait?
Wide-base with staggering & reeling
The function of this brain region is to encourage or strengthen movements - gives a "boost" to commands from motor cortex, lest they miss this area & be weak/feeble
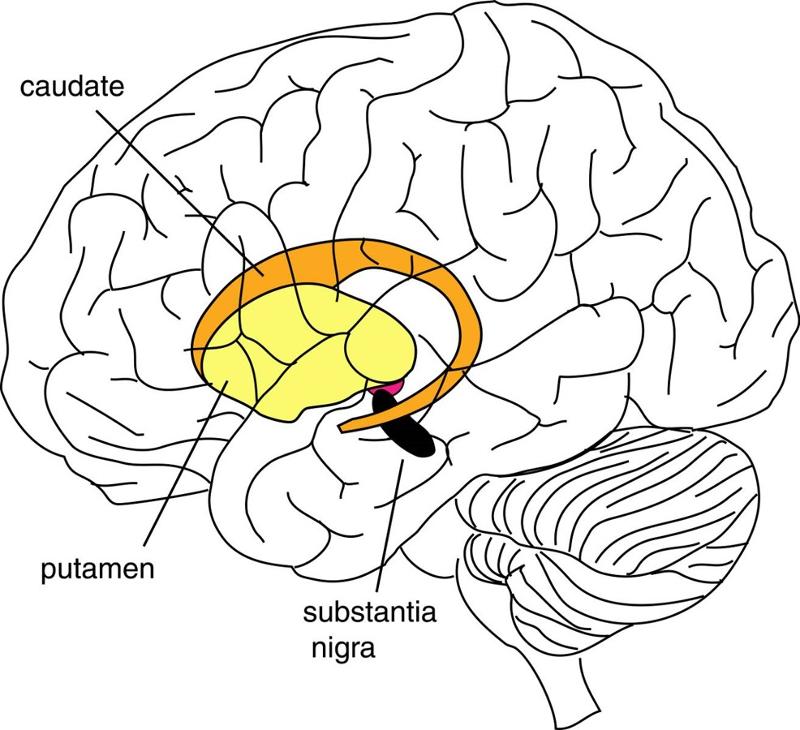
Basal ganglia
The substantia nigra, part of the basal ganglia, enhances movement through exciting the striatum (and other parts of basal ganglia). Its neurons use __1__ as its neurotransmitter, and in __2__ disease, these neurons mostly die, resulting in difficulty moving and weakness; slow & progressive
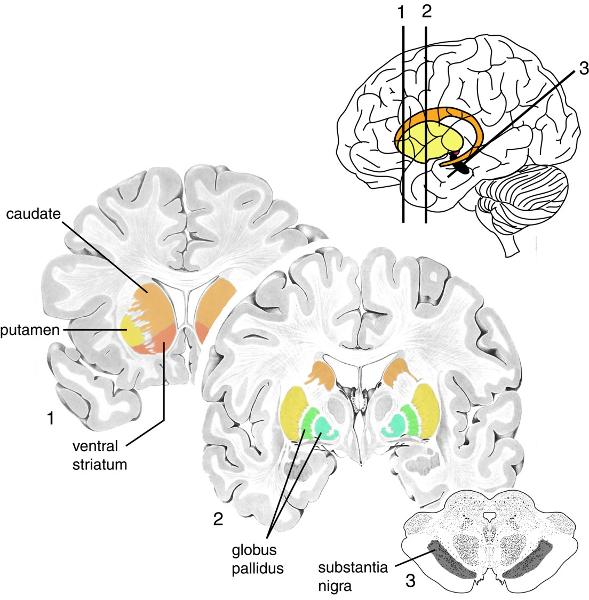
1. Dopamine
2. Parkinson's disease

ID the following:
-Left lateral ventricle (right hidden)
-4th ventricle
-3rd ventricle
No information
CSF flow starts in the __1__ ventricles, then thru the __2__ ventricle & into a tube that leads to the __3__ ventricle, also called the _____ 4 _____; it then exits to bathe the brain & spinal cord
1. Lateral
2. 3rd
3. 4th
4. Cerebral aqueduct
Which 2 routes of blood into the brain are essential for it to function?
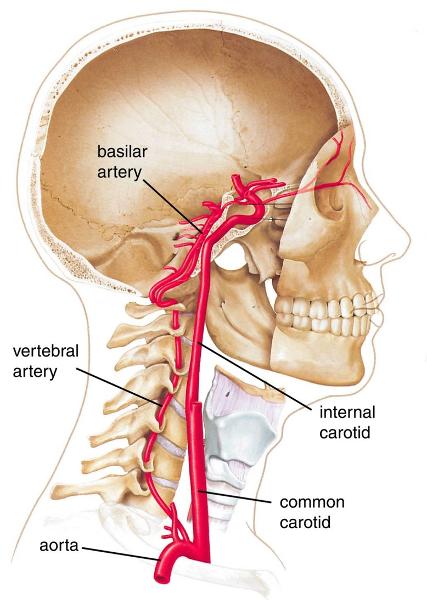
1. Vertebral arteries (threaded through cervical vertebrae)
2. Internal carotid
This vessel is clinically important because a rupture of one of its branches may result in a hematoma, which can compress the cortex
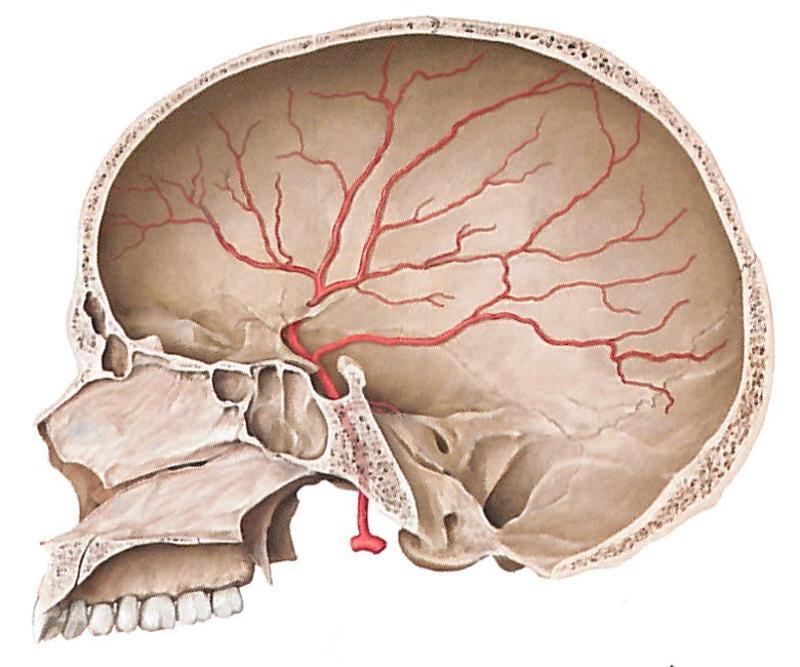
Middle meningeal (main artery of dura covering lateral & superior part of cerebral cortex)
This pathology is characterized by slow, oozing accumulation of blood with vague, nonspecific symptoms such as headache, cognitive impairment, unsteady gait
Subdural hematoma
Most common, and catastrophic, cause of this pathology is an aneurysm; can cause an extremely severe headache ("thunderclap")
Subarachnoid hemorrhage
Characterized by a "thunderclap" headache
Subarachnoid hemorrhage
Common location of an aneurysm
Where middle cerebral artery arises from internal carotid
These substances can get past the blood-brain barrier
-Glucose
-Amino acids
-Some ions
-Lipid soluble substances (i.e. ETOH)
Form blood-brain barrier; provide structure & sustenance in CNS
Astrocytes
Make glia wrapping (myelin sheath) in CNS
Oligodendrocytes
Autoimmune disease where myelin wrappings in some regions of white matter are attacked; these regions are subsequently termed "plaques"; plaques heal, but there remains unhealed damage that adds up over time; eventually patient may not be able to walk
Multiple Sclerosis (MS)
1. What difference would you see if you cut both an axon in the CNS & an axon in the PNS?
2. Why?
1. CNS - no regeneration
PNS - regenerates (very slowly)
2. Glia in CNS hostile to axonal regrowth, but Schwann cells (glia of PNS) actively promote axonal regrowth
Glia in this region are special; have been used to culture & grow more for injection into the spinal cord for regenerative purposes
Olfactory bulb
The peripheral nervous system can be divided into these 2 parts
Somatic & autonomic nervous systems
Nervous system that innervates skeletal muscles; r/t motor controls, such as voluntary movements & involuntary reflexes (i.e. patellar reflex, or knee jerk)
Somatic nervous system
In addition to innervating skeletal muscle for motor purpose, the somatic nervous system also has __1__ nerve fibers that are responsible for communicating __2__ information to the CNS, such as touch, temperature, & pressure
1. Afferent
2. Sensory
The autonomic nervous system is further divided into these 3 systems
-Sympathetic NS
-Parasympathetic NS
-Enteric NS
This nervous system is self-governed; innervates viscera (i.e. smooth muscle, cardiac) to adjust their functions
Autonomic nervous system
The __1__ coordinates ANS function with both the __2__ & __3__ systems, and circadian rhythmic activity (i.e. sleep-wake cycles)
1. Hypothalamus
2. Endocrine
3. Limbic (emotional)
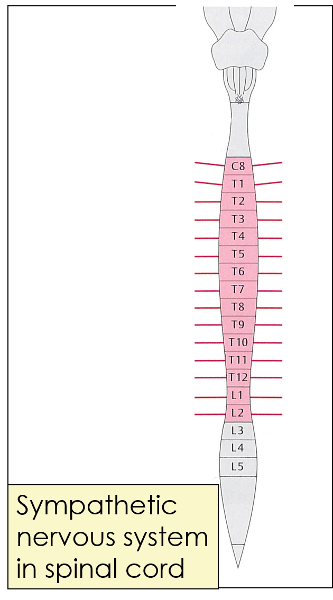
What does this picture represent?
Sympathetic nervous system in spinal cord (projecting lines represent nerves going out to sympathetic ganglia)
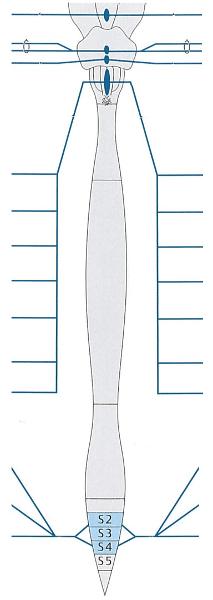
What does this picture represent?
Parasympathetic nervous system in brainstem & spinal cord
Where do the cell bodies of neurons belonging to the ANS reside?
Outside brain & spinal cord (mostly)
Organ involved in "sympathetic activation"
Adrenal gland (epinephrine)
BP is monitored by __1__ located in an enlarged part of the _____ 2 _____; information is sent to the __3__ center in the __4__
1. Baroreceptors
2. Carotid artery
3. Vasomotor
4. Medulla
If BP is too high, the __1__ nerve transmits __2__ activity to the heart to slow rate & reduce force; if BP is too low, signals from __3__ center go to __4__ cells in the spinal cord, which are then relayed to neurons in the _____ 5 _____, which accelerate HR & increase force of contraction
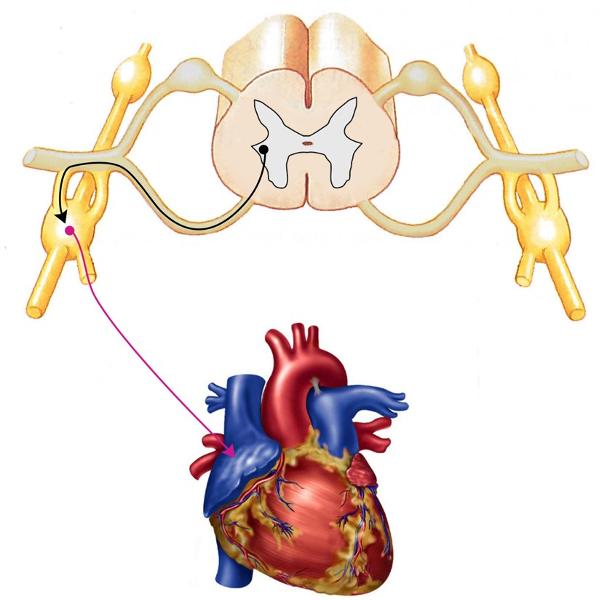
1. Vagus
2. Parasympathetic
3. Vasomotor
4. Sympathetic
5. Sympathetic chain (picture above)
Orthostatic hypotension is caused by these 2 factors
-Venous pooling
-Decreased venous return
Viral disease of spinal ganglia; dermatomally distributed skin lesions
Herpes Zoster (herpes virus)
Patients most at risk of developing a subdural hematoma
Young & elderly