Kidney Functions
Regulate ECF volume & blood pressure
Regulate osmolarity
Maintain ion balance
Regulate pH
Excrete wastes
Regulate hormone production
filter, reabsorb, secrete
nephron anatomy (picture)
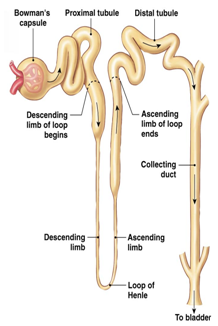
Normally highly twisted
Blood flows out of the nephrons into the efferent arterioles
Kidney portal system (picture)
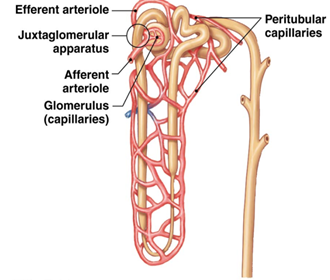
blood flows from the renal artery then into the cortex, then from the afferent arteriole into the glomerulus (ball-like network of capillaries). Then blood flows into the efferent arteriole then into the peritubular capillaries, then into the renal vein and out of the kidneys
In juxtamedullary nephrons, long peritubular capillaries that dip into the medulla are vasa recta.
Function: filter fluid out of the blood and into the lumen of the nephron at the glomerular capillaries, then to reabsorb fluid from the tubule back into the blood at the peritubular capillaries
kidney filtration (picture)
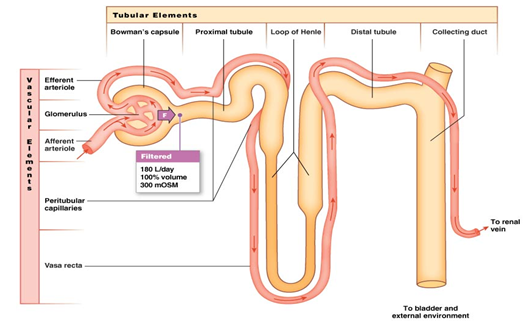
o Happens in glomerulus
o 300 mOsmol
o Filter fluid from plasma
o Leave behind plasma proteins & RBCs
o only 20% of the plasma that passes through the glomerulus is filtered and less than 1% of the filtered fluid is excreted (the other 99% return to systemic circulation
o takes place in the renal corpsule
net driving pressure causes filtration
renal corpuscle filtration
o first barrier is the capillary endothelium which contains glomerular fenestrated capillaries (large pores- RBC and most proteins still cannot pass)
o second filtration barrier is the basal lamina (Extensive extracellular matrix to exclude plasma proteins from the fluid)
o third filtration barrier is the epithelium of the bowmans capsule (podocyte foot processes leave narrow slits through which filtration takes place
3 pressure components acting within the renal corpuscle
Blood pressure – blood moving into glomerulus (provides hydrostatic pressure) forces fluid through leaky fenestrated capillaries
Osmotic pressure – Fluid moving back due to protein concentration differences
Capsule fluid pressure – hydrostatic fluid pressure of the enclosed space opposes fluid movement in and is in competition with blood and osmotic pressure
Glomerular filtration rate (GFR)
volume of liquid that filters into bowman's capsule that depends on 2 things: filtration pressure and the filtration coefficient (which depends on surface area of capillaries, permeability of membranes)
stays relatively constant even across ranges in blood pressure
regulated by blood flow in the renal arterioles or by autonomic regulation (sympathetic control changes the resistance in arterioles bu using NE to vasoconstrict as necessary)
regulation of the GFR by blood flow in the renal arterioles (picture)
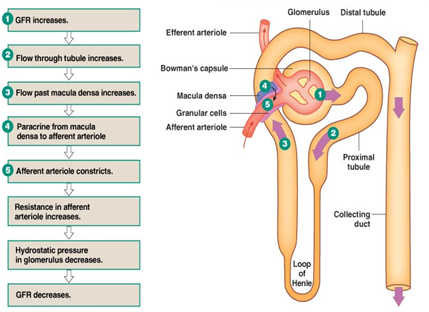
Increase in blood pressure= vasoconstriction to keep GFR constant
• Myogenic response: Vascular smooth muscle responds to pressure changes (Increase in blood pressure causes vasoconstriction, decreases causes vasodilation)
• Tubuloglomerular feedback: Paracrine signaling to change fluid flow through the loop of Henle
Passes by afferent and efferent arterioles which get direct feedback and twisting causes ascending limb to pass between afferent & efferent arterioles
nephron absorption (picture)
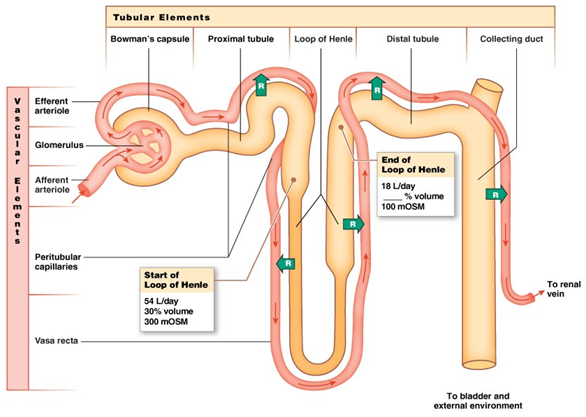
70% gets reabsorbed almost immediately
Loop of Henle is where solutes change concentrations
• About 100mOsmol at the end of the loop of Henle
• Must remove stuff without removing water
• Only 18L/day reaches the end of the loop
• Excrete about 1.5 L/day at the end of the tube
pressure gradient favors reabsorption
Nephron secretion (picture)
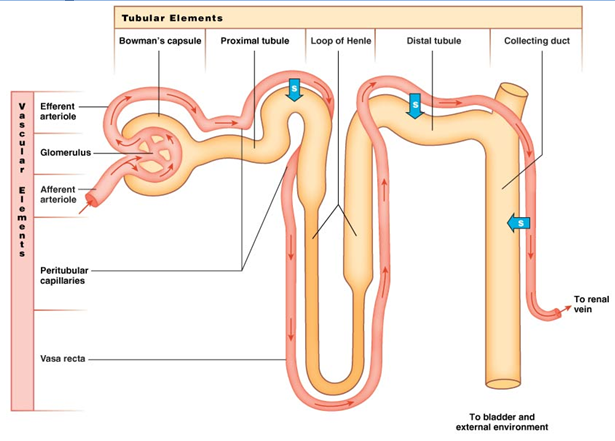
o After filtration, to adjust concentrations
o Happens via aided transport
o transfers solutes from the ECF to the lumen
o Na+ is the driving molecule with the sodium potassium pump
o uses transport molecules (active transport) and concentration gradients to fine scale adjust the concentrations in the lumen
nephron excretion (picture)
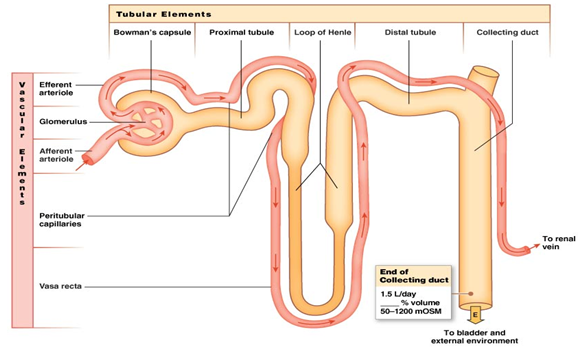
o about 1.5 L/day
o Amount Filtered- Amount reabsorbed+ amount secreted= amount of solute excreted
o most useful metabolites have been removed at this point
o ion and water concentration is highly variable depending on needs
Sodium (Na+) in kidney reabsorption
o Na+ is the main player because it sets up the electrical gradient (active transport)
o water equalizes concentrations by moving to the nephron from the lumen
o ECF has higher Na+ concentration than the ICF so Na+ follows its concentration gradient into cells and is actively pumped out of cells via the sodium-potassium pump
urea reabsorption in the kidneys (picture)
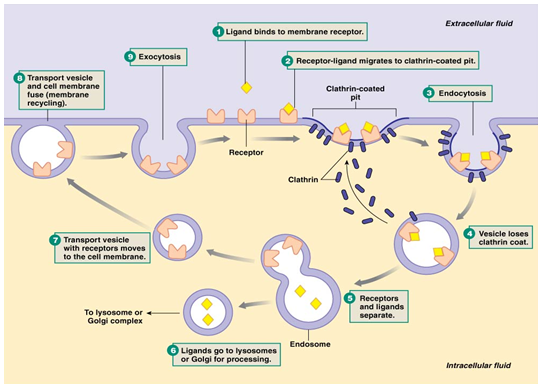
transports proteins into the epithelium and breaks them down
solute transport in the kidneys (picture)
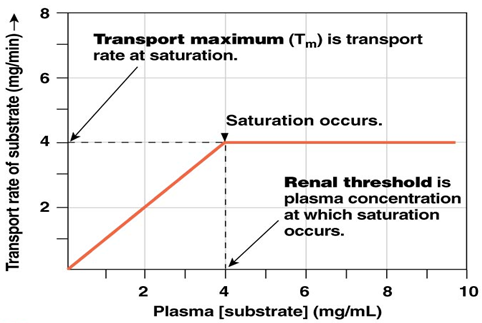
Saturation – Maximum rate of transport due to maximum carrier use (receptors and channels)
Filtration has a linear increase in the amount of glucose in the plasma and the glucose filtration rate
you can reabsorb up to 300 mg/mL and everything else gets excreted
clearance
easiest method to determine the Rate at which a solute disappears from the body due to excretion or metabolism
Provides a method for estimating GFR as well
Determines how well a nephron handles a filtered solute
Micturition
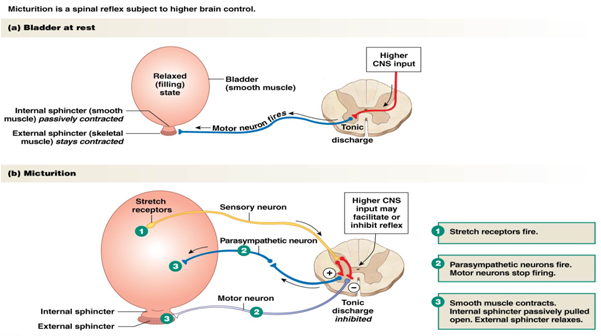
urination
what leaves the collecting duct must be excreted and the concentrations cannot be adjusted any further
Normal conditions: Motor neuron is leading to tonic contraction of the external sphincter
When you have to urinate
• Spinal reflex tells stretch receptors to fire-As you gain control of your bladder, more stretch receptors are present so that you can notice how full your bladder is instead of just whether you have to urinate or not
primary goal of the digestive system
move nutrients, water, and solutes from the external environment to the internal evironment
4 Basic Processes: Digestion- breaking down of food particles, Absorption, Motility, Secretion
gastrointestinal tract and secretion
hollow tube (lumen) passing through the body
the primary way pathogens can get into the body
• Secretions come from enzymes
• Substantial amount of fluid from secretions enter the digestive system
• 7.5/9 L of liquid is reabsorbed, the rest is excreted
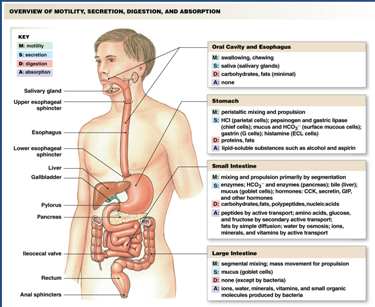
Gastrointestinal tract anatomy
mouth/ salivary glands- chewing and the secretion of saliva
stomach- mixes food with acid and enzymes to create a soupy mixture called chyme
small intestine- Ducts pour in enzymes from the liver to help break down and absorb the fluid and particles and nearly all the digested nutrients and secreted fluids are absorbed here
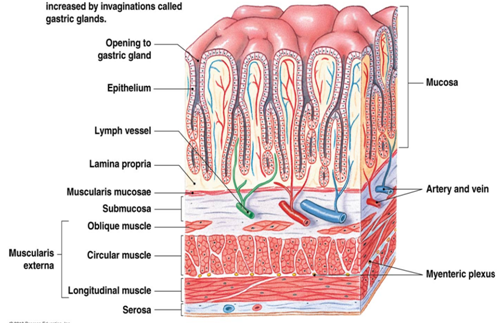
GI tract wall structure (picture)
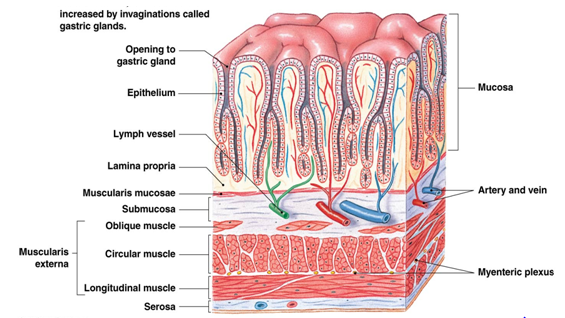
The stomach and wall function very similarly (only a few small differences)
Basic structure is similar in stomach and small intestine
• Mucosa- interfacing with the food and lumen
• Submucosa
• Muscularis externa
• Serosa
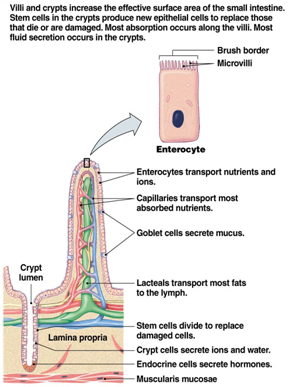
Mucosa (picture)
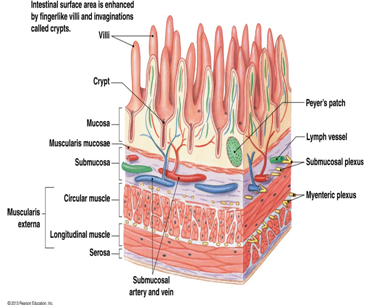
• layer of the GI Tract wall
o Gastric glands- Deep folds in mucosa
o Single epithelial tissue layer (enterocytes)
o Lots of goblet calls and other paracrine cells than excrete
o Makes up part of the intestinal space
o First line of defense by having many immune cells on the inside of the interstitial space
o villi- play a big role in absorption and mobility
o epithelial cell layer- function depends on their location in the tract (Transporting – enterocytes in small intestine, Secreting – endocrine & exocrine, Stem cells)
Muscularis externa
• layer of the GI Tract wall
- muscle layer
• Muscle rings- change the diameter of the lumen
• Longitudinal muscle- changes the length of the tube
o Longitudinal and muscle rings do not always agree
• Innervation for smooth muscle tissue is directly next to the layer
Submucosa
• layer of the GI Tract wall
- convergence of smaller vessels into larger muscles
•Basically the same for stomach and small intestine
Serosa
• layer of the GI Tract wall
- outermost layer
• Anchors the intestine and other organs within the abdominal cavity
o Must be anchored because the 2 muscle layers (muscle rings and longitudinal) must be working together so if they can move, then the muscles would just get tied into a knot
purpose of motility in the GI tract
o Two main purposes:
Move food through the GI tract
Mix food and break down into small pieces
• Food moves around a lot to absorb as many enzymes as possible to get broken down
GI smooth muscle contraction- migrating motor complex
• Normal pattern of contraction between meals
• Contraction begins in stomach and ends in large intestine
o Keeps things moving all in one direction
o Important in preventing infection
• Sweeps remnants to large intestine
GI smooth muscle contraction- peristalsis
• smooth muscle in the bottom 1/3 of the esophagus (the top 2/3 is skeletal muscle)
• peristaltic contraction pushed the food (bolus) into the receiving segment which pushes it forward more down the esophagus and into the stomach
• segmental contractions are responsible for mixing by alternating contracting segments so that there is little or no net forward movement and the bolus is exposed to as much intestinal wall (where enzymes are located) as possible
single unit smooth muscle in the GI tract (picture)
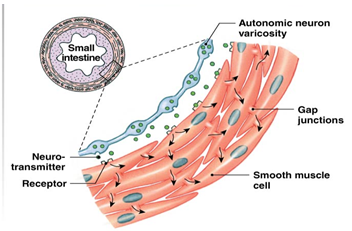
o Groups of cells connected by gap junctions
o Signal passes quickly through gap junctions
o Tonic or phasic contractions
GI tract contraction- slow wave potential
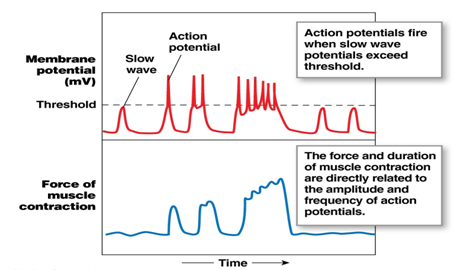
• Dependent on Ca2+ signaling
• Graded contractions
• More Ca2+ àstronger and/or longer contraction
Things the digestive system secretes
Ions & Water, Digestive enzymes, Mucus, Saliva, Bile
• Wherever we move ions, water wants to follow (osmotic equilibrium)
acid secretion in digestion
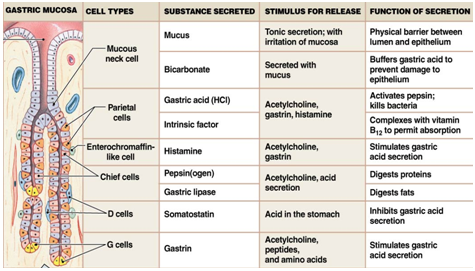
Parietal cells secrete acid
1-3 L of acid per day
Lumen of stomach can reach pH of 1(very acidic)
Parietal cell cytoplasm has pH=7.2 (pretty normal)
• Pumping out H+ extremely against its concentration gradient to transition from a pH of 1 to 7.2
• Very active process (uses ATP)
o Lumen net gain is a lot of chloride
o Bicarbonate goes into the interstitial fluid and eventually into the blood
o pancreas secretes bicarbonate to neutralize the acid that gets pumped into the lumen and enters the small intestine because we don't want a very acid fluid going into other tissues
bicarbonate secretion in digestion
Bicarbonate, water, Na+ & Cl- move into the lumen
H+ moves into ECF à blood
Sets up electrical gradient due to pumping of negative ions into the lumen
• Causes Na+ and water to pump through too
NaCl secretion in digestion
• Cryp cells from the small intestine and colon secrete salt solution
• Creates gradient for water to follow which creates an isotonic salt solution
enzyme secretion in digestion
o secreted by exocrine glands (Salivary glands and pancreas) or by epithelial cells in the mucosa of the stomach and small intestine
o Stored as proenzyemes
mucus secretion for digestion
o Made up of glycoproteins
o Forms protective coating over the GI mucosa and lubricates the contents of the gut
o Secreted by mucous cells (stomach), serous cells (salivary glands), and goblet cells (intestine)
o Also secretes salt solution
bile secretion for digestion
o Secreted by the liver (hepatocytes)
o Made up of:
o Bile salts – facilitate fat digestion (main goal)
o Bile pigments like bilirubin
o Cholesterol
o Drugs & other waste products
locations of digestive secretions
• Ions (acid, bicarbonate, salt)
• Digestive enyzmes (salivary glands & pancreas)
• Mucus (stomach, salivary glands, & intestine)
• Saliva (salivary glands)
• Bile (liver)
digestion and absorption
• Villi increase surface area for absorption
• Brush Border creates a border for protection
Not directly regulated
• Regulated by motility, feelings of hunger, etc.
3 major nutrients: carbohydrates, proteins, fats
Carbohydrates
• Starch, sucrose, glycogen, cellulose, lactose, maltose, glucose, fructose
o Must break giant polymers into smaller pieces (monosaccharides) before you can move it across a cellular border
o Amylase- breaks polymers into simpler molecules
Found in the saliva and gets secreted by the pancreas
o Enterocytes don’t use glucose (they use glucogen) so they don’t mess up the gradient
Proteins
• Most ingested protein are large molecules
• Not all proteins are processed equally (80% of protein is absorbed from eggs, only 30-40% absorbed from beans
• 30-60% of protein in lumen comes from dead cells & secretion
• endopeptidases and exopeptidases
endopeptidases vs exopeptidases
• Endopeptidases- breaks up initial peptide bonds
o Proteases are a more common name
o Proenzymes
o Ex: pepsin, trypsin
• Exopeptidases- break off amino acids from the amino or carboxyl ends of smaller proteins that have been broken up
o Carboxypeptidases are most important
protein transport in digestion
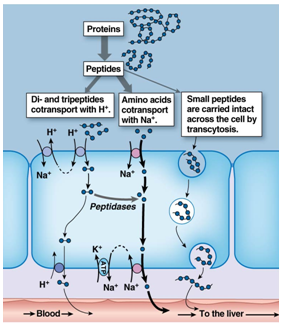
• Many different transport systems for the different amino acids
• Large proteins can be brought in via transcytosis
o Stimulates immune response and allergy responses
o Larger peptides are that are transported through the cell are more likely to cause an immune response so if you wait until a baby has more mature villi then they are less likely to transport those larger molecules and cause an allergic response
fats
• Triglycerides
• Cholesterol
• Phospholipids
• Long-chain fatty acids
• Fat-soluble vitamins
• Not water soluble
o Fat groups into large droplets
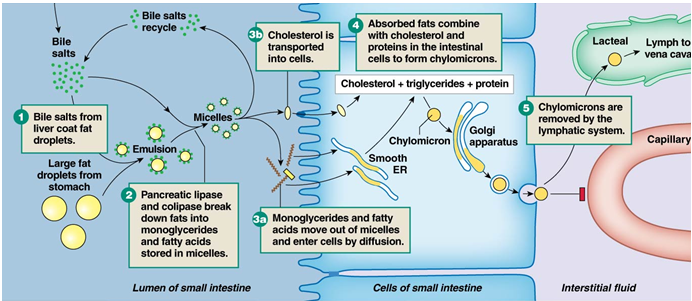
o Need to break up the droplets into smaller ones via Bile salts
bile salts
break up fats into smaller pieces
Bile salts interact with water
Fat droplets alone are relatively unstable (break into smaller ones)
• Bile salt ringed fat droplets are relatively stable
• Broken into smaller and smaller pieces
• Secreted into the lumen
micelles
combination of all the things that have been broken up into the lumen
• Small, disk-shaped droplets
• Diglycerides & monoglycerides, Phospholipids, Fatty acids, Cholesterol
• Migrate towards the microvilli and brush border for secretion
• Water soluble
o Does not need transport protein and will go through the membrane without a problem
• Once they pieces get through the membrane into the cytoplasm they reform into larger molecules that get secreted by the golgi apparatus
• Too big to go into the capillaries or normally secrete (A few fatty acids can pass to the capillaries but it is fairly infrequent)
fat digestion and absorption (picture)
nucleic acid digestion
• DNA & RNA polymers are small part of diet
• Broken down into nitrogenous bases & monosaccharides
• Nitrogenous bases require active transport for absorption
vitamin digestion
• Fat-soluble vs. water-soluble
• Fat-soluble vitamins are packaged into micelles and absorbed (vitamins A, D, and K)
• Water-soluble are absorbed by mediated transport (all B and C vitamins)
• Olestra- fat that cannot be absorbed
o Was added to chips but caused negative side effects when too much was ingested
mineral digestion
• Generally occurs via active transport
• Iron & calcium are actively regulated
ion and water digestion
• Most absorption occurs in small intestine
• Na+ & Cl- absorbed by multiple pathways
• K+ & water absorbed via paracellular transport
digestive system regulation signaling
o Neural, endocrine & local signals
Long reflexes (integrated in CNS)
Short reflexes (integrated within GI tract)
Peptide hormones & reflexes
• Paracrine system (stomach)
integration of digestive reflexes
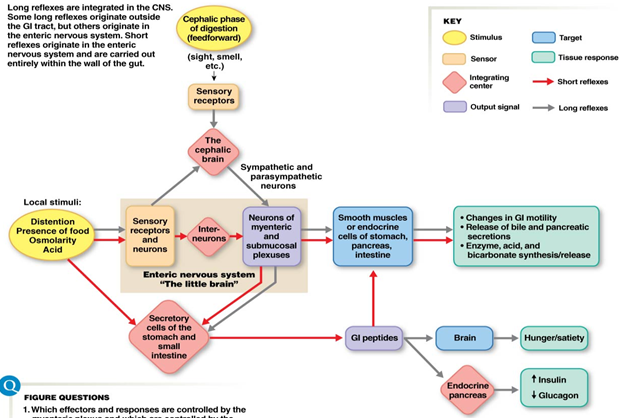
Everything is happening within GI tract\same responses we would normally see just input from the CNS is not required
Function of components of the GI tract in digestive signaling
Muscularis are in charge of secretion and regulates motility and control
o Peptides are a major class of signaling molecule
o Act as hormones or paracrine signals
Could affect other hormones as well
o Inhibit or excite secretion & motility
o Can work on either side of epithelial layer
enteric nervous system
Acts as an independent integrating center like the brain or spinal cord
Does not have a specific bundle or ganglia of nerve cells like the CNS for processing specific signals
Nerve network responds to sensory stimuli and initiates reflex
• Everything is reflex responses since there is no integrating center
shared characteristics between the enteric nervous system and the CNS
• Intrinsic neurons à interneurons
• Neurocrine molecules
• Glial support cells
• Tight capillaries around ganglia à blood-brain barrier
• Acts as an integrating center
digestive system summary (picture)
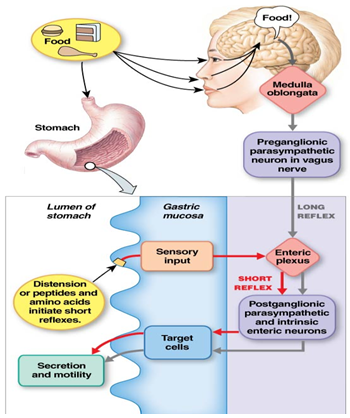
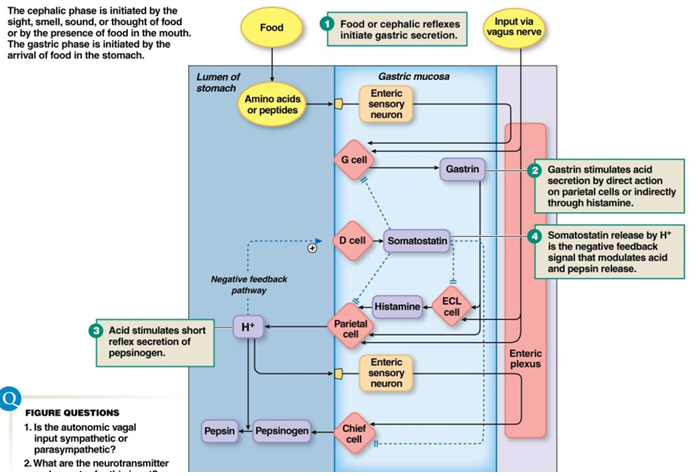
cephalic phase of digestion
Feedforward response
• Smelling, seeing, or thinking about food triggers digestion
Anticipation or stimulus of food in mouth causes stimulation via medulla
Food in mouth causes: Salivary response (Lubricates, Digests - salivary amylase (starts breaking down carbohydrates), Protects – Lysozyme), Mastication = chewing, Deglutition= swallowing
steps of swallowing
tongue pushes bolus against soft palate
breathing is inhibited as the bolus passes the closed airway (epiglottis folds down to help keep swallowed material out of the airways and upper esophagael sphincter relaxes)
food moves downward into the esophagus propelled by peristaltic waves and
gastric phase reflex (picture)
Stomach function- storage
o Bring in 3.5L of food, liquid, & saliva per day
Relaxed stomach holds 45mL of liquid, after a normal meal it expands to 1.5L, after a large meal it can stretch to 2.5-3L
o Regulates amount of food that goes into small intestine for digestion
o Upper stomach (fundus) stores food
stomach function- digestion
o Lower stomach (antrum) continues digestion
o Peristalsis mixes food with enzymes & acid to break down food
Only 10% of digestion happens in the stomach, the rest happens in bile, etc.
secretory cells of the gastric mucosa
integration of cephalic and gastric phase secretion
stomach function- protection
o Mucous neck cells secrete mucuous- bicarbonate barrier
o Gastric juice pH = 2
o Enterocyte cell surface pH = 7
intestinal phase
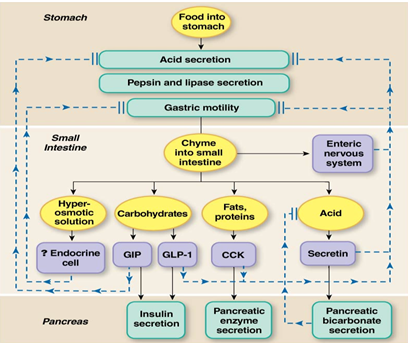
Chyme enters small intestine
Started to break down proteins by pepsin in stomach
Rate of entry of chyme determines intestinal response (secretion, motility, nutrient use)
intestinal phase secretion
• Bicarbonate (pancreas)- Neutralizes stomach acid
• Mucus (goblet cells)- Lubricates & protects epithelium
• Bile (gallbladder)- Fat digestion
• Digestive enzymes (enterocytes & pancreas)- Break down food particles
• 5.5L of total stuff in the lumen after secretion
hepatic portal system (picture)
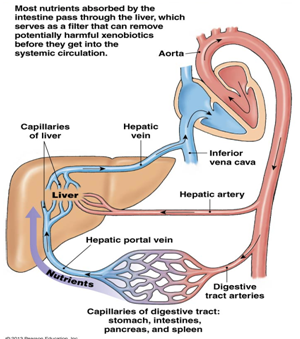
• after the transport of organic nutrients and ions through the duodenum and jejunum most absorbed nutrients move into the capillaries in the villi and then into the hepatic portal system.
• specialized region of the circulation that has 2 sets of capillary beds: one that picks up absorbed nutrients in the intestine and another that delivers the nutrients to the liver
absorption in the small intestine
7.5L of 9L reabsorbed
Most happens in duodenum & jejunum
Move into capillaries & then the hepatic portal system
As you move solutes water will follow
digestion in the intestines
• most digestion occurs in the small intestine
• Protein -Broken down by many peptidases & proteases à small peptides & amino acids
• Carbs- Digestible polysaccharides broken down into monosaccharides & absorbed
• Fats- Bile salts enter at the duodenum to allow digestion & absorption
• By large intestine down to 1.5 L of stuff
differences between large intestine and small intestine walls
Large intestine has:
Colonocytes
Mucosa (Smooth, no villi)
Muscularis (Discontinuous longitudinal layer)
large intestine digestion and absorption
o Traditionally thought that little to no digestion/absorption occurs here
o Recent research increasingly points to importance of gut bacteria for digestion
gut microbiome
o Around 500 species of bacteria in your gut
o Key for breaking down nutrients
o Three main categories: Prevotella (Carbs & simple sugars), Bacteroides (Proteins),Ruminococcus
Absorption of nutrients is dramatically affected if these bacteria are missing
o Byproduct: gas production
o babies develop a gut microbiome which varies depending on the way the birth was given, how much the baby is interacted with (exposure) and whether the baby drank breast milk ir formula
o stool transplant
large intestine motility
o Chyme enters colon & mixes via segmental contractions
o Forward movement is minimal
o Occurs via mass movement
Decreases diameter of colon
Pushes bolus forward
Gastrolic reflex
o Pushes bolus into rectum
defecation
• Distension of rectal wall initiates
• Internal anal sphincter relaxes
• Peristalsis pushes material forward
• External anal sphincter relaxes & feces move out of anus
• Emotions and the limbic system can affect defecation
diarrhea
• Abnormal water absorption causes watery feces
o Osmotic-Unabsorbed solutes pull water into feces (Ex: Lactose, sorbitol, Olestra, polyethylene glycol)
o Secretory-Bacterial toxins enhance Cl- secretion, Increased fluid secretion causes increased motility
M cells
• Specialized epithelial cells
• Sample gut content
• Transport content to interstitial fluid
• If bad stuff present, launch immune response
o Cytokines are released and trigger an immune response
• Irritable bowel syndrome- M cells can misrecognize normal foods and cause an immune response to normal food
vomit reflex
Protective reflex
Force contents out of stomach and duodenum
Regulated by medulla
Caused by: Cytokines, drugs, pain, disturbed equilibrium
Reverse peristalsis- smooth muscle wave moves from small intestine, through the stomach, up the esophagus, and out the mouth
appetite vs. satiety
Regulated by two hypothalamic centers
• Feeding center
o Tonically active
o Removal results in stopping eating
• Satiety center
o Inhibits feeding center
o Removal results in overeating which causes obesity
glucostatic theory
o a theory about how food uptake is regulated
o Glucose metabolism regulates food intake
o Low blood glucose levels causes a suppression of satiety center which causes hunger
lipostatic theory
o Lipid level regulates food intake
o Body seeks to maintain an “ideal” weight
o Low lipid level à hunger
o Some research support for this theory
Leptin – protein hormone made in adipocytes that indirectly regulates food intake
Neuropeptide Y directly regulates food intake
energy output
• Transport work- Moving molecules between compartments, moving materials into/out of body, Includes gradients for solutes
• Mechanical work, Muscle contraction, movement of vesicles down filaments
• Chemical work, Growth, maintenance, & storage
metabolic rate
o Oxygen consumption (indirect calorimetry)
Easiest way to measure
Measure O2 used and convert that into glucose using the glucose pathway
o Estimate of glucose metabolism indirectly
o Glucose metabolism is most efficient using aerobic pathways
• Metabolic rate (kcal/day)= L O2 consumed/day * kcal/L O2
energy storage
• Get energy from proteins, carbohydrates & fats
• Store energy for immediate use primarily as glycogen (Glycogen is more compact for storage than glucose)
• Long term storage as fat
metabolism
o Sum of all chemical reactions in the body
Extract energy from nutrients
Use energy for work
Store energy for later work
anabolism (small to larger molecules) vs. catabolism (larger to smaller molecules)
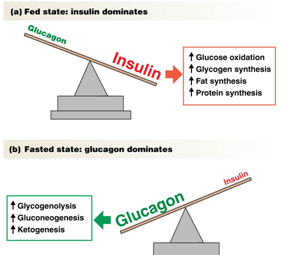
fed state vs. fasted state
Fed State vs Fasted State
o Fed state
AKA absorptive state
Following a meal
Anabolic pathways (smaller to larger molecules) active
most glucose is stored as glycogen in fats
o Fasted state
AKA postabsorptive state
Used up nutrients from food already
Catabolic pathways active (larger to smaller molecules)
most glucose is used right away (in the form of glycogen)
o Body turns incoming proteins into amino acids that can be used where they are needed
If there is too much protein the proteins can be turned into glucose and used for energy
hormone regulation of metabolism
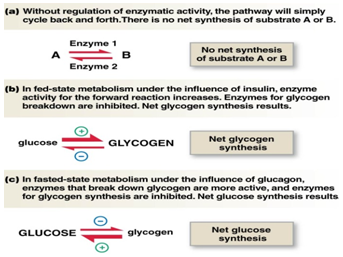
insulin drives the production of glycogen from glucose
fed-state metabolism- carbohydrates
• Absorbed by intestine as monosaccarides (glucose mostly)
o About 30% of the glucose that goes through the liver is immediately metabolized
o The remaining 70% is sent out to the blood and circulated to the areas where it is needed
o If it is not needed it is stored as glycogen
fed-state metabolism- protein
• Absorbed by intestine as amino acids
• Diffuse into blood via hepatic portal vein
• Sent to the liver
• Excess amino acids get stored as fat
fed-state metabolism- fats
o Triglycerides + phospholipids + cholesterol + lipid-binding proteins
o More protein = heavier
o Range from VLDL (very low density lipoproteins) to HDL (high density lipoproteins)
o Protein bound with lipids makes them more soluble to cell membranes
o cholesterol
cholesterol
o Range from VLDL (very low density lipoproteins) to HDL (high density lipoproteins)
Cholesterol levels are determined by the number of lipoproteins in the lipoprotein-cholesterol complex
o Most found as low-density lipoprotein cholesterol (LDL-C)
“Lethal cholesterol”
Uses apoprotein B to diffuse through membranes
o Second most common is high-density lipoprotein cholesterol (HDL-C)
“Healthy cholesterol”
Uses apoprotein A to diffuse through membranes
o Elevated LDL-C level is largest risk factor associated with heart disease
Can manage through diet, exercise, drugs
nutrient disorders
• Diabetes mellitus – abnormal glucose metabolism
• Kidney & liver disorders – abnormal plasma protein levels
• Heart disease – abnormal cholesterol levels
o No studies that show causation between high dietary cholesterol and blood cholesterol levels
o Is a correlation between high blood cholesterol and heart disease
fasted vs fed state metabolism nutrients (picture)
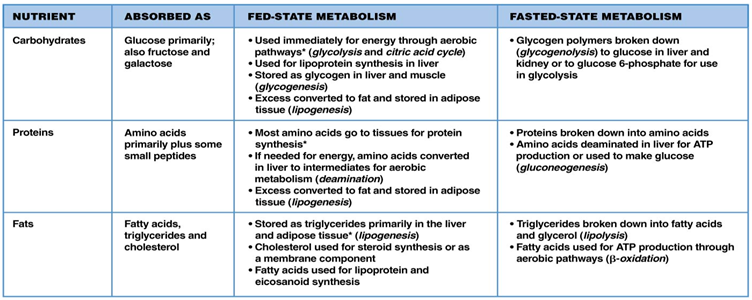
fasted state metabolism
After all nutrients from a meal have been cleared from digestive tract & plasma glucose concentrations start to fall
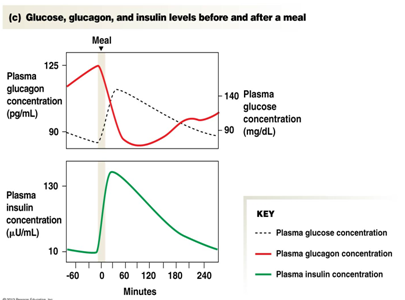
• After a meal blood glucose rises and fasted state begins when the glucose begins to fall
Plasma glucose level a key regulator
Catabolism hallmark of postabsorptive state
glycogenolysis (carbohydrate fasted state metabolism)
glycogen can be converted directly to glucose 6-phosphate by the addition of a phosphate
glycogen that is broken down first to glucose then phosphorylated "costs" the cell an extra ATP
most glycogen is found in the liver
amino acid catabolism (protein fasted state metabolism)
deamination- removal of the amino group from an amino acid creates ammonia and an organic acid
body does not like ammonia (toxic) so it gets secreted
free amino acid pool used for energy production
creates pyruvate, acetyl CoA, etc. that can be used in glycolysis and the citric acid cycle
lipolysis (fat fasted state metabolism)
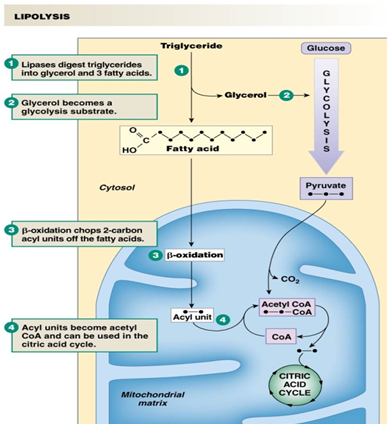
• Primary fuel-storage molecule
• Excess acetyl CoA production à ketones
o Useful in the citric acid cycle
• Basis for fad diets (Atkins, South Beach)
metabolism regulation (picture)
o Primarily regulated by endocrine cells
o Pancreas secretes insulin & glucagon
o Ratio of two hormones is what drives metabolism
o Insulin and glucagon are both always present so the ratios of them are what matter
o Short half lives, so they need to be replaced regularly
GLucose, glucagon, and insulin levels before and after a meal (picture)
insulin

Peptide hormone
Stimuli for insulin secretion:
• Increased plasma glucose
• Increased plasma amino acids
• Feedforward effects of other hormones involved in digestion
• Autonomic division activity
o “rest and digest”
glucagon
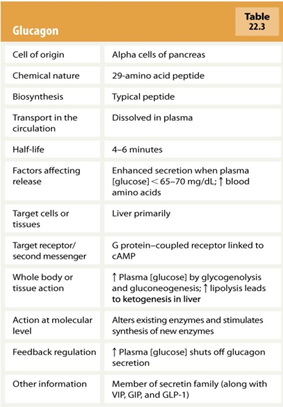
o Secreted by alpha cells in pancreas
o Whatever insulin does, glucagon does the opposite
o Low plasma glucose causes glucagon release
o Triggers catabolism
o Glycogenolysis & gluconeogenesis to generate new glucose
o Liver is primary target
metabolism regulation dysfunction
o Diabetes mellitus- Abnormally elevated plasma glucose levels (AKA hyperglycemia)
o Type 1 – insulin deficiency due to beta cell destruction
Fasted state: in the absence of insulin, there are no GLUT4 transporters in the membrane, Fed state: insulin signals the cell to insert GLUT 4 transporters into the membrane, allowing glucose to enter the cell
Damaging to blood vessels, eyes, kidneys & nervous system
8.3% of the U.S. population
o Type 2 – insulin resistant
Variety of problems: Atherosclerosis, Neurological changes, Renal failure, Blindness
heat loss
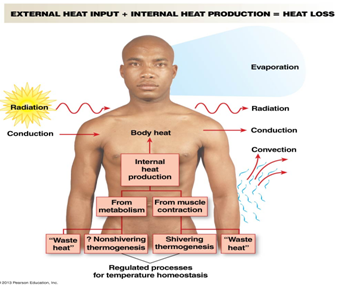
conduction, radiation, convection, evaporation
thermoregulation
Thermoneutral zone (82-86°F)
Normal metabolism generates enough heat to maintain body temperature
above that range causes gain of heat and the need to cool down, likewise for below that range
sweating
sweating
• Evaporative cooling
• Use 2-3 million sweat glands in skin
• Sympathetic control
• Secretion of hypotonic solution
• Dependent on humidity
cutaneous blood flow
• Use convection by passing blood close to surface
• Sympathetic control
• Heat conservation- Close to zero blood flow through cutaneous layer
• Heat loss- 1/3 of cardiac output to cutaneous layer
thermogenesis
• Shivering
o Skeletal muscle contraction generates heat
• Non-shivering
o Brown fat- fat found in babies between the shoulder blades which is just now being discovered in adults
o More pronounced in babies and non-humans
variation in temperature regulation
• Circadian patterns: Daily, menstrual cycle
• Postmenopausal hot flashes
• Fever-Pyrogens
Cytokines produced by immunocytes
Increase body temperature
Enhances activity of WBCs
major functions
Recognize and remove foreign invaders
Recognize and remove abnormal body cells
Remove dead or damaged cells
immune system dysfunction
• Incorrect response- Fail to recognize self from non-self (Ex: Autoimmune diseases)
• Overactive response- Respond at a greater level than threat posed (Ex: Allergies)
• Lack of response- Failure of immune system to respond (Ex: Acquired immunodeficiency syndrome (AIDS))
bacteria
• Divides by self replicating
• Circular DNA, Unicellular, Small, Cell wall
• Prokayoric (no nucleus)
• No membrane bound organelles
• Antibiotics work well to kill bacteria
virus
• Needs a host to reproduce
• DNA or RNA
• Use host cell machinery
• Small genomes
• Integration of DNA
lymphoid tissue
• Found throughout body
• Thymus gland
• Bone marrow
• Lymph nodes
• Diffuse tissues
Cells of the immune system
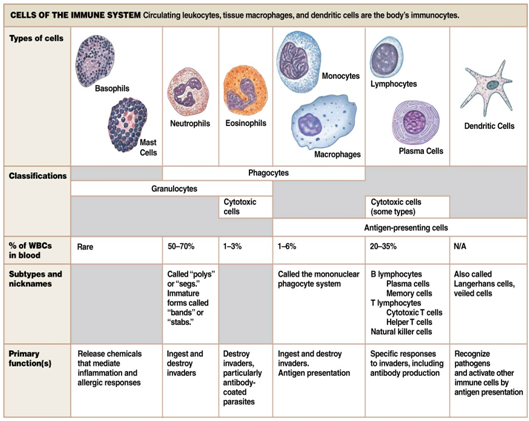
Neutrophils
• Phagocytes
• Most abundant WBC- 50-70% of white blood cells
• Release pyrogens
o Fever response
Basophils
• Important for inflammatory & allergic responses
• Granulocytes
o Histamine, Heparin
eosinophils
• Rare
• Allergic & parasitic response
• Granulocytes
o Cytotoxins
Monocytes and Macrophages
• Monocytes à macrophages
• Trash cans of immune system
o Pick up and take out mostly everything
o Anything abnormal, aging
• Antigen-presenting cells
lymphocytes
• Key part of acquired immunity
• B lymphocytes
• T lymphocytes and Natural killer (NK) cells- play important roles in defense against intracellular pathogens, such as viruses
dendritic cells
• Non-circulating
• Antigen-presenting cells
• Found in skin
immunogen, antigen, antibody
• Immunogen- Anything that triggers the body’s immune response
• Antigen- Immunogen that reacts with immune response
• Antibody- Proteins secreted by immune cells that bind to antigens to make them more visible to immune response
goals of an immune response
• Detection and identification of foreign substances
• Communication to other immune cells
• Coordination of response
• Suppression of target
types of immunity
• Innate Immunity- Present from birth, Nonspecific, immediate response
• Acquired Immunity- Specific response, Slower response
lymphoid tissue
Found throughout body
Thymus gland
Bone marrow
Lymph nodes
Diffuse tissues
immune response
Epithelium- the protective barrier of skin and mucous membrane is the body's first line of defense
Secretions- salivary glands and the glands in airways secrete mucus and immunoglobulins to trap and disable inhaled or ingested pathogens
Stomach acid- the low pH of the stomach helps destroy swallowed pathogens
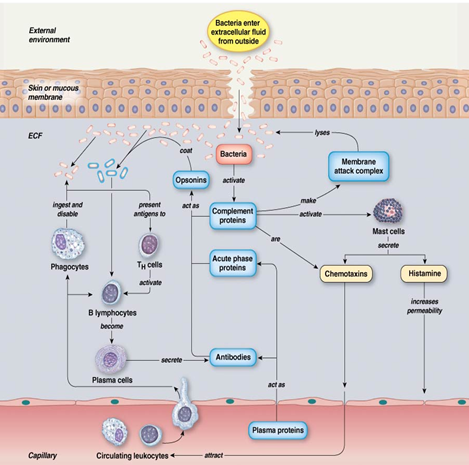
phagocytes
• Innate immunity
• Attracted by chemotaxins
• Secrete own chemotaxins (cytokines) to attract more phagocytes
• Chemotaxins bind to PRRs
• Secrete inflammatory cytokines
• Ingest pathogen
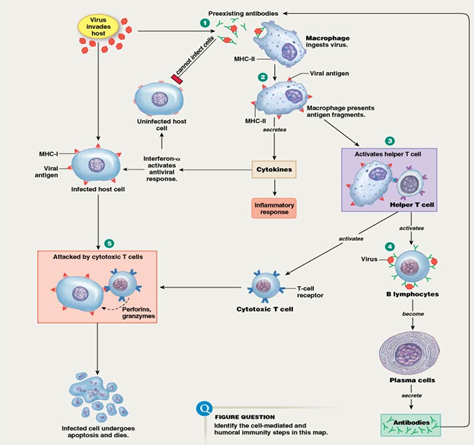
natural killer cells
• Innate immunity
• Key for viral infections and cancer cells
• Rapid response
• Trigger apoptosis in infected cells
inflammatory response for innate immunity
• inflammatory response is key for innate immunity
• Attracts immune cells
• Produces physical barrier to prevent spread of infection
• Promotes tissue repair
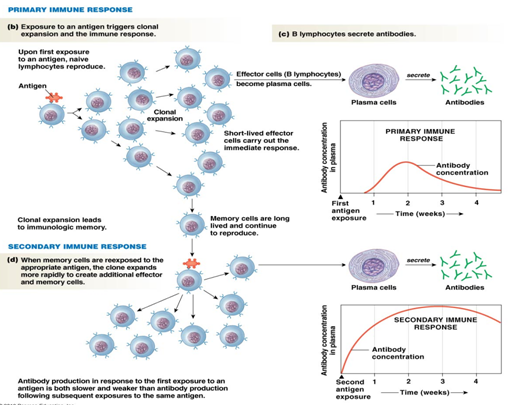
B lymphocytes
• antibody production and antigen presentation, become plasma cells
• memory cells: coordinate immune response much more quickly and strongly when exposed to the same antigen a second time
• effector cells: short lived plasma cells that carry out the immediate immune response and secrete antibodies
T lymphocytes
o Cytotoxic – Attack & destroy
o Helper – Coordinate immune response
major histocompatibility complex (MHC)
• tissue rejection- want similar HLA antigens for tissue transplant (blood groups)
Active and Passive immunity
Active immunity
• Body responds to pathogen & creates antibodies
• Ex: chicken pox, vaccines
Passive immunity
• Receive antibodies made from another organism
• Ex: Motheràfetus, breast milk
Antibodies (AKA immunoglobulins) (picture)

o Activate B lymphocytes
o Act as opsonins
o Enhance phagocytosis
o Trigger cytotoxic responses
o Activate complement proteins
o Activate mast cells
Bacteria Immune Response (picture)
virus immune response (picture)
allergen immune response (picture)

Inflammatory immune response to a non-pathogenic antigen
Wide range of triggers and severity
Key player: Histamine
vaccination immune response (picture)